
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Intra-operative test electrode and electrical auditory brainstem response prior to cochlear implantation in CHARGE syndrome
M Jabri*; G Hamza; M Mourai; M Loudghiri; W Bijou; Y Oukessou; S Rouadi; R Abada; M Roubal; M Mahtar
Department of Otolaryngology, Head and Neck Surgery, Ibn Rochd University Hospital, Faculty of Medicine and Pharmacy, Hassan II University, Casablanca, Morocco.
*Corresponding Author : M Jabri
Department of Otolaryngology, Head and Neck Surgery, Ibn Rochd University Hospital, Faculty of Medicine and Pharmacy, Hassan II University, Casablanca, Morocco.
Email: jabrimeryeme2@gmail.com
Received : Jun 20, 2024
Accepted : Jul 11, 2024
Published : Jul 18, 2024
Archived : www.jcimcr.org
Copyright : © Jabri M (2024).
Abstract
Introduction: Assessing auditory nerve excitability is crucial in determining candidacy for Cochlear Implantation (CI). Pre-operative tests, such as Electrical Auditory Brainstem Response (EABR), are utilized to evaluate the function of the auditory pathway. However, uncertainties about auditory pathway excitability may persist despite these tests.
Objective: This article aims to present the inaugural case in our department where intra-cochlear test electrodes were employed to verify pre-operative EABR outcomes and validate auditory pathway excitability just before CI implantation.
Methods: We utilized intra-cochlear test electrodes to simulate CI stimulation in a 2-year-old patient with a suspicion of cochlear nerve agenesis. This approach aimed to obtain auditory brainstem response results comparable to those observed post-implantation.
Results: The application of intra-cochlear test electrodes successfully validated the pre-operative EABR outcomes, confirming the excitability of the auditory pathway. This was further corroborated by the promontory stimulation test and intraoperative EABR.
Conclusion: The use of intra-cochlear test electrodes represents a significant advancement in CI candidacy assessment methods. This case marks a milestone in our exploration of improved techniques to evaluate auditory nerve excitability, particularly in complex cases such as suspected cochlear nerve agenesis.
Keywords: Promontory stimulation; Electrical stimulation; Cochlear implant; Auditory nerve; Charge syndrome; Cochlear nerve deficiency.
Citation: Jabri M, Hamza M, Loudghiri M, Bijou W, Oukessou Y, et al. Intra-operative test electrode and electrical auditory brainstem response prior to cochlear implantation in CHARGE syndrome. J Clin Images Med Case Rep. 2024; 5(7): 3174.
Introduction
Cochlear implantation remains a cornerstone in the management of severe to profound Sensorineural Hearing Loss (SNH), offering significant auditory rehabilitation for individuals facing such challenges. In doubtful candidacy of Cochlear Implant (= CI) patients, intraoperative tests have been conducted to assess nerve excitability and auditory pathway integrity. These tests include promontory testing and electrical auditory brainstem responses via intra-cochlear stimulation. Here, we present a clinical case of suspected bilateral cochlear nerve agenesis, where the performance of these two tests helped determine the indication for cochlear implantation. This article introduces the first case in our department where intra-cochlear test electrodes were utilized to confirm pre-operative EABR results and assess auditory pathway excitability immediately before Cochlear Implant (CI) surgery. The case involves a 2-year-old patient diagnosed with Charge syndrome, representing a notable advancement in our pursuit of enhanced CI candidacy assessment techniques.
CHARGE syndrome is characterized by congenital multiple anomalies (coloboma, heart defect, choanal atresia, retarded growth and development, genital hypoplasia and ear anomalies/deafness [1,2].
These anomalies were first reported by Hall and Hittner in 1979, after which the acronym was proposed by Pagon et al. In 1981. The diagnostic criteria, initially proposed by Blake et al. In 1998 and later updated by Verloes, emphasize the importance of semicircular canal hypoplasia or aplasia and are widely used today for the clinical diagnosis of CHARGE syndrome is a congenital disorder with an incidence of approximately 1 in 10000 births. It is an autosomal dominant disorder that does not have sex-linked expression [3].
Among the various clinical manifestations of CHARGE syndrome, otologic symptoms and signs are consistently prominent, included as major criteria in both Blake’s and Verloes’ clinical criteria. Characteristic temporal bone anomalies are reported to be present in 98% of CHD7 mutation positive cases, along with external ear malformations and hearing loss found in over 90%. Analysis of temporal bone Computed Tomography (CT) findings has revealed aplasia or hypoplasia of the semicircular canal, cochlear dysplasia, atresia of the Bony Cochlear Nerve Canal (BCNC), oval window atresia, and ossicular malformations as common characteristics of CHARGE syndrome
Presentation of the case
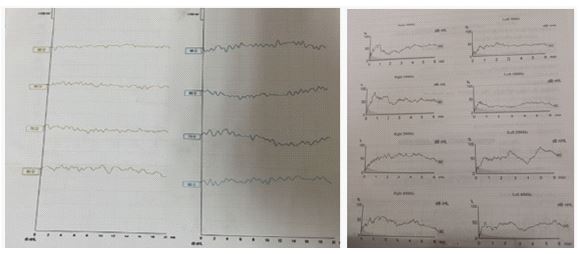
We present the case of a 2 years old female patient with no history of consanguinity. She was born prematurely at 28 weeks of gestation and stayed in the neonatology unit for a month. She has Charge syndrome and underwent surgery for choanal atresia and persistent ductus arteriosus. The patient is well vaccinated according to the National Immunization Program (NIP). There is no history of trauma or meningitis. The medical history goes back to the age of 6 months when the parents noticed a lack of reaction to noises. She had a motor developmental delay, managed through psychomotor rehabilitation with favourable progress. The Otoscopy showed normal findings bilaterally, with no external ear malformation. The speech therapy assessment indicates that she is a good candidate for cochlear implantation. The ABR and ASSR were performed and no auditory threshold was found (Figure 1). The otoacoustic emissions were present in both ears.
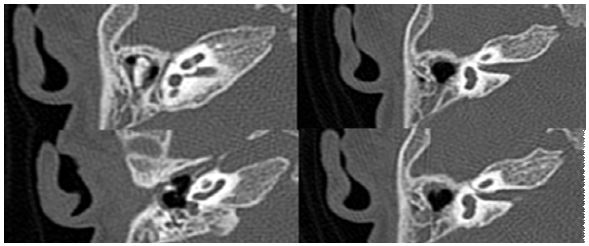
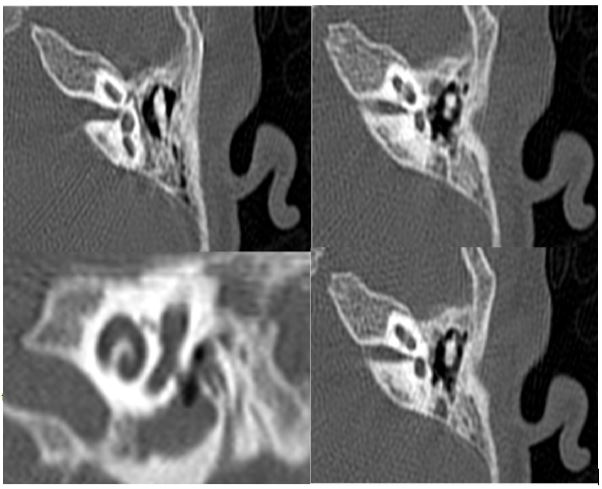
A CT-Scan and an MRI were performed, The CT-Scan showed signs of CHARGE syndrome with densification of the modiolus and a hypoplasia of the cochlear nerve canal measured at 0.7 mm on the right ear and 0.6 mm on the left one. Moreover, there was a hypoplasia and a deformation of the vestibule more pronounced on the left along with an agenesis of the superior and lateral semi-circular canals and a partial agenesis of the posterior semi-circular canals” (Figures 2,3).
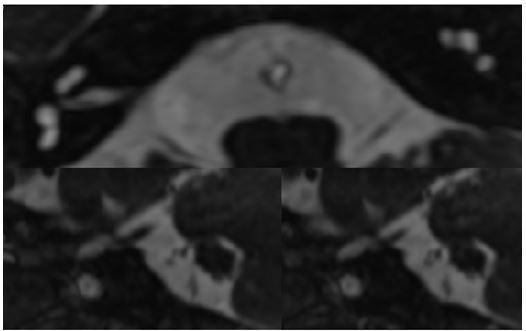
The MRI revealed the agenesis of the semi-circular canals bilaterally with no visualization of the cochlear nerves nor continuity between the fundus of the internal auditory canal and the base of the modiolus along with a hypoplastic appearance of the vestibules (Figure 4).
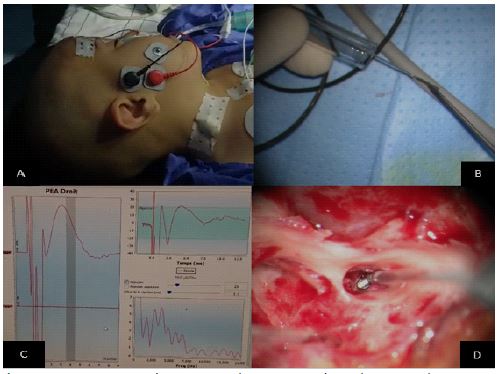
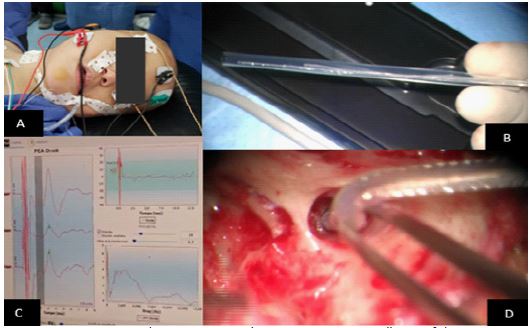
The therapeutic decision was to perform a cochlear implantation in the right ear with the consent of the parents and the cooperation of the MED-EL™ team, with Intraoperative electrophysiological tests including promontory stimulating test and electric intraoperative ABR prior to the implant using the MED-EL auditory nerve test system = ANTS
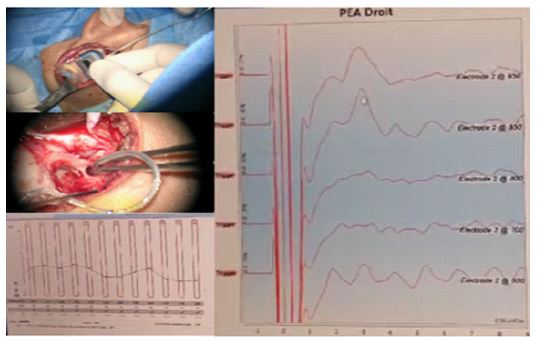
The promontory stimulating test was inconclusive in our case (Figures 5,6) and the ANTS revealed a V wave confirming the presence of auditive nerve fibers (Figures 7,8). Thus, the patient underwent the cochlear implantation (Figure 9). Impedance measurements were highly satisfying; EABR confirm the presence of the V wave with a stimulation at 850 cu. Post-Operatively, the patient underwent a structured rehabilitation program encompassing auditory-verbal therapy and cochlear implant programming. Regular follow-up evaluations are scheduled to facilitate the fine-tuning of device settings and monitoring of auditory progress. The hindsight we have gained is not enough to assess the outcome of the cochlear implantation accurately.


Discussion
The prevalence of hearing loss in children has been reported to be between 1-6 of 1000 [4,5]. In congenital severe sensorineural hearing loss (SNHL) or deafness, treatment with a cochlear implant is the therapy of choice. Preoperative radiological imaging is essential for visualizing the anatomy of the inner ear. Recommendations regarding the imaging modality are inconsistent [6,7]. Most centers perform both Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) [8].
A prerequisite for successful cochlear implantation is an intact cochlear nerve, as cochlear implantation surgery is contraindicated in the setting of cochlear nerve aplasia, whereas in cochlear nerve hypoplasia, this treatment may be considered. Therefore, precise radiological evaluation of the vestibulocochlear nerve by high-resolution MRI of the temporal bone is required.
Approximately 60% of congenital sensorineural hearing loss is a result of genetic inheritance, of which 30% are syndromic and 70% are non-syndromic. The remaining 40% is acquired or environmental in etiology [6].
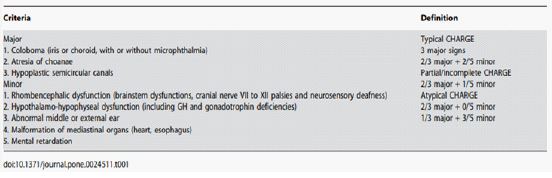
Charge syndrome is a rare genetic disorder with an estimated incidence of 1 in 12,000 to 1 in 15,000 live births [3-9]. The diagnosis is primarily clinical. Among the various clinical manifestations of CHARGE syndrome, otologic symptoms and signs are consistently prominent, included as major criteria in Verloes’clinical criteria (Figure 10). Magnetic Resonance Imaging (MRI) of the temporal lobe shows absent or hypoplastic semi-circular canals (this malformation may predict the presence of a CHD7 gene mutation). The diagnosis is confirmed by genetic testing [9], although this was not possible in our case due to limited resources. Cochlear nerve hypoplasia is often associated with CHARGE syndrome. Patients with this condition may benefit from cochlear implantation, especially if they have a larger cochleovestibular nerve diameter and no severe mental retardation. Auditory brainstem implantation is an alternative for those who do not improve with cochlear implants. Radiological findings frequently indicate cochleovestibular nerve deficiency, highlighting the importance of early intervention for better auditory rehabilitation outcomes [9].
Assessing cochlear nerve function is crucial before proceeding with cochlear implantation in patients with cochlear nerve deficiency. Promontory Electrical Stimulation Testing (PST), introduced by House and Brackmann [10], aids in distinguishing between sensory and neural hearing loss by providing information on auditory nerve function. PST involves electrical stimulation on the cochlear promontory through a myringotomy to elicit an auditory sensation. If auditory stimulus is noted, it is presumed the nerve is functional and considered further for co chlear implantation However, due to its rarity and maintenance challenges, PST has become obsolete, limiting the assessment of patients with questionable cochlear nerve function [11].
Electrical Auditory Brainstem Response (EABR) serves as a valuable alternative for evaluating auditory pathway integrity when standard evaluation methods are inconclusive. Intra-operative EABR using a test electrode correlates well with EABR using cochlear implant stimulation, offering advantages such as reusability and external stimulation [12,13].
Several monitoring methods have been developed to overcome limitations in cochlear nerve assessment. Patel et al. [14] introduced CI evoked Electrical Auditory Brainstem Response (E-ABR) and neural response imaging testing for real-time auditory nerve monitoring. Cochlear Nerve Action Potential (CNAP) monitoring, which involves placing the electrode on the cochlear nerve, provides high-amplitude waveforms in shorter intervals compared to conventional auditory brainstem response (ABR), facilitating cochlear nerve monitoring during surgery. It has also been used for the cochlear nerve monitoring with vestibular schwannoma surgery with cochlear implantation [15].
Recently, an Auditory Nerve Test System (ANTS; MED-EL Corporation, Innsbruck, Austria) was developed [17] with three components: an auditory nerve test electrode comprising an 18 mm electrode with three intracochlear contacts and an extracochlear ground, a stimulator box, and a connector cable. The stimulator box is connected to the CI programming hardware to send biphasic pulses to the Electrode Array, which can Evoke E-ABR [13]. E-ABR confirmation during surgery with ANTS could lower the risk of opening a CI only for monitoring purposes.
In our case, the promontory stimulating test was inconclusive and ANTS was perfomed which revealed a V wave confirming the presence of auditive nerve fibers. Thus, the patient underwent a cochlear implantation.
Conclusion
Intra-operative Electrical Auditory Brainstem Response (EABR) using an ANTS emerges as a promising tool for assessing auditory nerve excitability before cochlear implantation. Our study underscores the importance of such intra-operative assessments, particularly in cases with doubtful pre-operative results. The consistency between intra-operative EABR using the test electrode and traditional CI stimulation methods confirms the reliability of this approach. Moreover, our findings underscore the growing trust in pre-operative objective tests, such as pre-op. EABR, in evaluating CI candidacy. Despite the preliminary nature of our data, intra-operative EABR using the test electrode demonstrates feasibility and reliability, offering valuable insights into auditory nerve function during surgery. Further research is warranted to validate these findings on a larger scale and explore additional applications of this technique in cochlear implantation procedures. Overall, intra-operative EABR with a test electrode holds promise as a valuable adjunct in optimizing CI candidacy assessment and improving outcomes for patients with hearing loss.
Conflicts of interest statement: All authors declare that they have no conflicts of interest.
References
- Ideura M, Nishio S ya, Moteki H, Takumi Y, Miyagawa M, et al. Comprehensive analysis of syndromic hearing loss patients in Japan. Sci Rep. 2019; 9: 11976.
- Hittner HM, Hirsch NJ, Kreh GM, Rudolph AJ. Colobomatous microphthalmia, heart disease, hearing loss, and mental retardation--a syndrome. J Pediatr Ophthalmol Strabismus. 1979; 16(2): 122‑8.
- N U, M S. Pubmed. CHARGE Syndrome. 2024. Disponible sur: https://pubmed.ncbi.nlm.nih.gov/32644625/.
- Kim YS, Kim Y, Jeon HW, Yi N, Lee SY, et al. Full etiologic spectrum of pediatric severe to profound hearing loss of consecutive 119 cases. Sci Rep. 2022; 12(1): 12335.
- Sorge M, Sorge I, Pirlich M, Fuchs M, Meuret S, et al. Diameter of the Cochlear Nerve Canal predicts Cochlear Nerve Deficiency in Children with Sensorineural Hearing Loss. Rofo. 2022; 194(10): 1132‑9.
- Chin O, Dharsono F, Kuthubutheen J, Thompson A. Is CT necessary for imaging paediatric congenital sensorineural hearing loss? Cochlear Implants International. 2020. Disponible sur: https://www.tandfonline.com/doi/abs/10.1080/14670100.2019.1669291
- Wang B, Cao K, Wei C. [Cochlear implantation in patients with auditory neuropathy assisted by intra-operative EABR and the therapeutic effect evaluation]. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2013; 27(10): 449‑54.
- Lee SY, Kim SH, Bae YJ, Kim EH, Koo JW, et al. Appropriate Imaging Modality for the Etiologic Diagnosis of Congenital Single-Sided Deafness in Children. J Clin Med. 2018; 7(12): 515.
- Bergman JEH, Janssen N, Hoefsloot LH, Jongmans MCJ, Hofstra RMW, et al. CHD7 mutations and CHARGE syndrome: the clinical implications of an expanding phenotype. J Med Genet. Mai 2011; 48(5): 334‑42.
- House WF, Brackmann DE. Electrical promontory testing in differential diagnosis of sensori-neural hearing impairment. The Laryngoscope. 1974; 84(12): 2163‑71.
- Kelly EA, Levine S, Gravel KE, Hart DL, Huang T. Utilization of Nerve Integrity Monitor for Promontory Stimulation Testing Prior to Cochlear Implant. Otol Neurotol. 2018; 39(2): 60‑2.
- Polterauer D, Mandruzzato G, Neuling M, Polak M, Müller J, et al. Intra-operative test electrode and electrical auditory brainstem response after preoperative assessment in cochlear implant candidacy: Comparison of electrical auditory brainstem response results by using an auditory nerve test electrode and system intra-operatively after an pre-operatively objective promontory stimulation test to check integrity of the patient’s auditory pathway. Current Directions in Biomedical Engineering. 2023; 9(1): 725‑8.
- Lassaletta L, Polak M, Huesers J, Díaz-Gómez M, Calvino M, et al. Usefulness of Electrical Auditory Brainstem Responses to Assess the Functionality of the Cochlear Nerve Using an Intracochlear Test Electrode. Otol Neurotol. 2017; 38(10): 413‑20.
- Patel NS, Saoji AA, Olund AP, Carlson ML. Monitoring Cochlear Nerve Integrity During Vestibular Schwannoma Microsurgery in Real-Time Using Cochlear Implant Evoked Auditory Brainstem Response and Streaming Neural Response Imaging. Otol Neurotol. 2020; 41(2): 201‑7.
- Sanna M, Piccirillo E, Kihlgren C, Cagliero G, Guidi M, et al. Simultaneous Cochlear Implantation After Translabyrinthine Vestibular Schwannoma Resection: A Report of 41 Cases. Otol Neurotol. 2021; 42(9): 1414‑21.
- Hosoya M, Nagaoka Y, Wakabayashi T, Shimanuki MN, Nishiyama T, et al. A novel intraoperative continuous monitoring method combining dorsal cochlear nucleus action potentials monitoring with auditory nerve test system. Journal of Otolaryngology - Head & Neck Surgery. 2023; 52(1): 67.
- Dhanasingh A, Hochmair I. Special electrodes for demanding cochlear conditions. Acta Otolaryngol. 2021; 141(1): 157‑77.