
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Looking beyond retinopathy of prematurity
Subina Narang1; Sonia Bariya1; Alisha Kishore1; Suksham Jain2*
1Department of Ophthalmology, Government Medical College and Hospital, Chandigarh, India.
2Department of Paedatrics, Government Medical College and Hospital, Chandigarh, India.
*Corresponding Author : Suksham Jain
Department of Paedatrics, Government Medical College and Hospital, Chandigarh, India.
Tell: 91-9646121587;
Email: subina_navya@yahoo.com
Received : Jun 28, 2024
Accepted : Jul 12, 2024
Published : Jul 19, 2024
Archived : www.jcimcr.org
Copyright : © Jain S (2024).
Keywords: Osteogenesis imperfecta; Retinopathy of prematurity.
Citation: Narang S, Bariya S, Kishore A, Jain S. Looking beyond retinopathy of prematurity. J Clin Images Med Case Rep. 2024; 5(7): 3177.
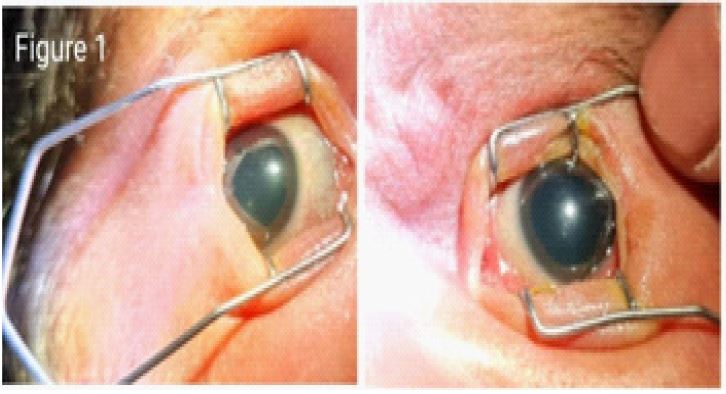
Case summary
A 2050 gm, 34 weeks gestational age term female with a family history of Osteogenesis Imperfect (OI) was referred for ROP Screening. She was on oxygen support for respiratory distress. On examination, both eye sclera showed blue-grey discoloration (Figure 1). Fundoscopy of both eyes showed Stage 1, Zone II Retinopathy of Prematurity (ROP) (Figure 2). X-ray legs confirmed a fracture of the shaft of left femur with decreased mineralization of bone falling into type III Osteogenesis Imperfecta (OI) with anterior bowing of both tibia (Figure 3). The parents refused any genetic testing, as the elder male child had tested positive for OI and died 6 months after diagnosis.


Discussion
OI is a genetic connective tissue disorder due to abnormal synthesis or processing of type I collagen (90%); Type I-IV are autosomal dominant, Type VI-XIII are autosomal recessive [1]. Bone fragility in OI is not an isolated phenomenon but a part of the spectrum of abnormalities associated with basic collagen defect [2]. In the index case, an early diagnosis was clinched due to a high index of suspicion of the condition as there was a family history of the disease in the elder sibling. The spectrum ranges from milder forms of bone susceptibility to the most severe forms like underdeveloped lungs incompatible with life. It is difficult to ascertain the cause of ROP in the present case as the baby had no high-risk factors like small gestational age and lower birth weight except oxygen support for respiratory distress. Patients with OI may also have an accompanying bleeding tendency secondary to capillary fragility caused by abnormal collagen support around blood vessels [3]. Multiple reports on bleeding diathesis in OI till date. We for the first time report ROP in osteogenesis imperfecta. Preterm babies with osteogenesis imperfecta may require an early eye examination for ROP screening.
Conflict of interest: No.
Financial disclosure: No.
References
- Sam JE, Dharmalingam M. Osteogenesis Imperfecta. Indian J Endocrinol Metab. 2017; 21(6): 903-908.
- Mondal RK, Mann U, Sharma M. Osteogenesis imperfecta with bleeding diathesis. Indian J Pediatr. 2003; 70(1): 95-6.
- Ganesh A, Jenny C, Geyer J, Shouldice M, Levin AV. Retinal hemorrhages in type I osteogenesis imperfecta after minor trauma. Ophthalmology. 2004; 111(7): 1428-31.