
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Challenging urological reconstruction in post-tuberculosis contracted bladder and renal complications: A rare case report
Maged Almogahed*; Dawei Wu; Jialin Gao; Jinguo Wang
Department of Urology, The First Bethune Hospital of Jilin University, Changchun, Jilin province, 130012 China.
*Corresponding Author : Jinguo Wang
Department of Urology, The First Bethune Hospital of Jilin University, Changchun, Jilin province, 130012 China.
Email: jinguo@jlu.edu.cn
Received : Jun 16, 2024
Accepted : Jul 15, 2024
Published : Jul 22, 2024
Archived : www.jcimcr.org
Copyright : © Wang J (2024).
Abstract
Background: Genitourinary Tuberculosis (GUTB) represents a manifestation of extrapulmonary tuberculosis associated with significant urinary tract complications, such as contracted bladder and renal insufficiency. This report delineates a rare instance of GUTB culminating in considerable urological impairment, necessitating complex reconstructive procedures.
Case presentation: A 53-year-old male, previously diagnosed with tuberculosis and having already received a left nephrectomy, was diagnosed with bladder contracture, right distal ureteral stenosis, right hydronephrosis, and renal insufficiency. The extensive urinary tract damage was addressed through urological reconstruction, incorporating the placement of double “J” stents and the construction of an ileal neobladder.
Interventions: The surgical intervention, aimed at addressing severe bladder damage, involved meticulous planning and execution. It began with a midline abdominal incision. When the damage was necessitated, a partial cystectomy was performed, removing up to half of the bladder. To restore urinary functionality, a neobladder was constructed from intestinal tissue. This new bladder, or ileal neobladder, was then connected to the urethra and any remaining parts of the original bladder. Utilizing such sophisticated techniques ensures the reinstatement of a more natural urination process, significantly improving the patient’s quality of life.
Outcomes: The postoperative period was marked by a notable enhancement in the patient’s urinary function and overall quality of life, demonstrating the efficacy of tailored surgical interventions in the treatment of severe complications stemming from GUTB.
Conclusion: This case underscores the critical need for heightened clinical vigilance and the employment of customized, innovative surgical approaches in the treatment of GUTB, especially in cases with non-standard presentations. Furthermore, it highlights the pivotal role of prompt diagnosis and timely surgical intervention in averting long-term adverse outcomes.
Keywords: Genitourinary Tuberculosis (GUTB); Contracted bladder; Ileal neobladder; Hydronephrosis; Renal insufficiency.
Citation: Almogahed M, Wu D, Gao J, Wang J. Challenging urological reconstruction in post-tuberculosis contracted bladder and renal complications: A rare case report. J Clin Images Med Case Rep. 2024; 5(7): 3178.
Introduction
Genitourinary Tuberculosis (GUTB), recognized as the second most prevalent form of extrapulmonary tuberculosis, manifests through the hematogenous dissemination of the causative organisms during the primary phase of infection [1]. The kidney frequently serves as the initial site of involvement in urinary tuberculosis, with subsequent involvement of other parts of the urinary tract occurring through direct extension via urine. Chronic tuberculosis of the bladder typically develops as a secondary complication of renal tuberculosis, which may be accompanied by bilateral or unilateral renal scarring, ureteral strictures, Vesicoureteral Reflux (VUR), or unilateral renal insufficiency. The insidious onset of the disease and challenges in diagnosis often result in delayed treatment, potentially leading to severe consequences, including extensive fibrosis and scarring of the bladder [2,3].
Despite rigorous surveillance, monitoring efforts, and the administration of supervised treatment utilizing contemporary antimicrobial chemotherapy, the incidence of the disease is persistently rising, resulting in numerous fatalities in a silent manner. Genitourinary Tuberculosis (GUTB) represents a predominant form of Extrapulmonary Tuberculosis (EPTB), frequently impacting the kidneys through hematogenous spread from active or latent foci within the lungs [4]. Furthermore, the infection disseminates to other components of the Genitourinary System (GUS) via the urinary tract. Initially, patients exhibit nonspecific lower urinary tract symptoms, often resulting in diagnostic delays. Concurrently, the mycobacterium insidiously compromises the urinary system through either caseous necrosis or a fibrosing reaction. Consequently, over 50% of patients necessitate surgical intervention at some point in their lifetime [5].
Bladder Tuberculosis (BTB) represents a severe complication of renal tuberculosis, diagnosed in approximately 45.6% of cases of Urogenital Tuberculosis (UGTB). Bladder involvement consistently follows renal tuberculosis, initiating at the ureteral orifice and varying from patchy cystitis to a fibrosed, contracted bladder. Despite significant advancements in diagnostic methods, national reporting systems, and chemotherapy regimens, managing genitourinary tuberculosis remains a formidable challenge for urologists. It is estimated that around 55% of individuals with genitourinary tuberculosis necessitate surgical intervention [6].
Case presentation
A 53-year-old male with a documented history of Tuberculosis (TB) presented to our department for surgical intervention following an admission from an outpatient clinic due to complaints of “bladder spasm.” Despite a previous TB diagnosis, the patient did not exhibit typical TB symptoms such as fever, sputum production, dyspnea, or palpitations throughout the disease course. Furthermore, there were no reports of activity-induced shortness of breath, nausea, vomiting, frequent urination, urgency, or incomplete urination. The predominant clinical manifestation was gross hematuria and a sensation of bladder tightness, with the patient’s stools, diet, sleep, and weight remaining unaffected. The patient’s medical history was notable for the absence of hypertension, diabetes, coronary heart disease, blood transfusions or drug allergies, except for a noted food allergy and no history of vaccination. Surgical interventions in the patient’s history included a left nephrectomy seven months prior, necessitated by severe renal damage attributed to renal TB, leading to unmanageable symptoms and potential health risks, and a right percutaneous nephrostomy creation five months prior due to right hydronephrosis.
Upon examination, the patient displayed normal vital signs and consciousness, with no abnormal findings noted during a comprehensive physical examination encompassing multiple systems. Laboratory analyses revealed a negative urine PCT test from the nephrostomy and a negative urine PCT test from the urethra when the nephrostomy tube was temporarily closed. Laboratory analyses also showed elevated alkaline phosphatase levels at 135.9 U/L, with total protein (61.3 g/L) and albumin (36.4 g/L) within normal ranges. Urinalysis indicated hematuria (1+), significant leukocyte esterase activity (3+), a heightened white blood cell count (321.90), and positive nitrites. Additional findings included elevated uric acid (738 umol/L) and creatinine (135.0 umol/L). The urine analysis further revealed occult blood (1+), proteinuria (1+), and bacterial presence (1082.3/HPF). Lymphocyte levels were measured at 1.05x109/L, with a Platelet Distribution Width (PDW) of 8.6.
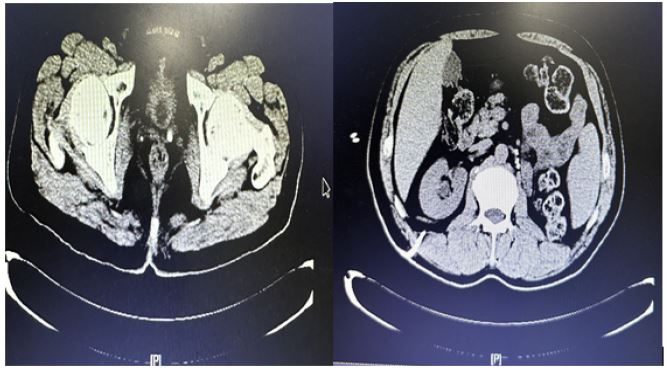
Diagnostic imaging demonstrated right hydronephrosis, suggestive of potential ureteral obstruction, with the absence of the left kidney corroborating the patient’s nephrectomy history. CT imaging of the whole abdomen underscored significant bladder contraction and dilation of the right ureter close to the bladder, reflecting the considerable impact of previous conditions on the current urinary tract complications.
Surgical technique
In the execution of this surgical procedure, the patient was positioned in a supine stance, with legs adequately parted to ensure optimal access to the operative field, adhering to established sterilization and draping protocols to maintain an aseptic environment. The operation commenced with a precision-guided midline abdominal incision, initiated above the pubic symphysis and extending 2.0 cm below the umbilicus, carefully penetrating the dermal, subcutaneous, and anterior rectus sheath layers, followed by a meticulous dissection along the Linea alba.
Retroperitoneal access was achieved, leading to the gentle liberation of the bladder. A thorough exploration of the pelvic anatomy revealed distinct tissue planes devoid of any tuberculosis activity. Progressing, a three-lumen F20 balloon catheter was inserted through the urethral orifice, verifying the urethral conduit’s integrity and the absence of tuberculous strictures. This was followed by the introduction of 40 ml of sterile saline into the bladder, assessing bladder distensibility within the pelvic cavity.
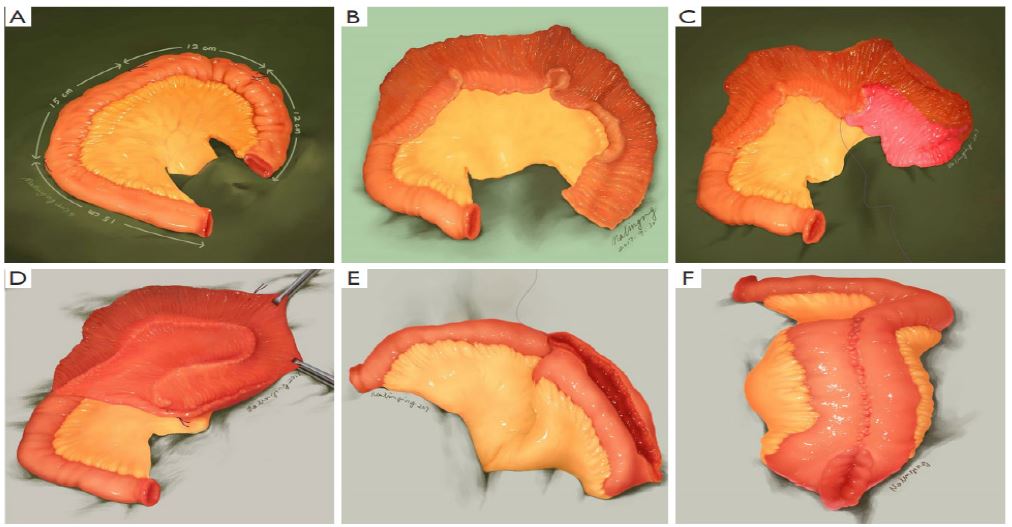
Utilizing an ultrasonic scalpel, the team performed a precise dissection of the bladder’s lateral walls, then retracted the peritoneal fold from the bladder’s apex posterior wall, fully mobilizing the bladder’s superior segment. A longitudinal incision on the bladder facilitated the evacuation of its contents, revealing thickened walls maintaining mucosal integrity and clear bilateral ureteral orifices. Attention shifted to the right ureter, which underwent isolation, dissection, and transection, with subsequent aseptic precautions to minimize contamination risk. An ileal segment was prepared, detubularized, and cleansed, followed by suturing with 3-0 absorbable sutures to form a spherical neoileal bladder. A critical step involved placing an F22 mushroom head drainage tube within the neobladder, secured with absorbable sutures, and externalized to serve as a drainage system for the neoileocystostomy. The procedure advanced by creating a small opening on the neobladder’s right posterior side, through which the right ureter was introduced and secured within the neoileal structure, supported by an F6 double “J” stent to facilitate urine flow from the renal pelvis to the neobladder.


The operation concluded with the careful closure of the peritoneum and neobladder’s mesentery, confirming the structural and vascular integrity of the new urinary reservoir, along with meticulous hemostasis and strategic drainage placement to mitigate postoperative risks. This detailed account exemplifies the integration of comprehensive planning, surgical expertise, and a commitment to patient welfare, reflecting the pinnacle of contemporary urological surgical practices.
Results and follow-up
At the 2-week postoperative evaluation, the patient exhibited overall health and satisfactory condition, accompanied by a minor elevation in serum creatinine levels, measured at 106.9. Subsequent renal scanning during this follow-up revealed minimal functionality of the right kidney, and the normal size of the right kidney are positive outcomes. After 2 months, all kidney function became normal. Urine PCR was negative after 2 months. Liver function is abnormal. Chemo stops. Urinary flow rate, residual urine the nephrostomy tube was taken out 1 month later, and the and the stent taken out 2 months later. No hydronephrosis by ultrasound.
Discussion
One side kidney TB, bacteria going down, bladder TB, then stenosis of the lower part of the ureter. The obstruction can manifest distally due to ureteral stenosis or proximally in cases of intrarenal stenosis [8]. Tuberculosis affecting the urethra and bladder originates from a descending infection through the urinary collecting system. In an experimental study, ureteral tuberculosis was identified in pigs inoculated in the kidney, presenting with complete occlusion of the ureter [9]. In ureteral tuberculosis, multiple stenoses emerge along the ureter, predominantly at the vesicoureteral junction [10,11].
In clinical settings, two types of tubercular bladder conditions are commonly encountered: one characterized by active tuberculosis with a bladder capacity of approximately 150-200 mL, and the other, a smaller, contracted variant often termed ‘thimble bladder [12]. Reconstructive surgery of the bladder is advocated in instances where gross anatomical distortion renders the Genitourinary System’s (GUS) normal functioning untenable. The primary objective of bladder augmentation is to enhance bladder capacity, thereby facilitating urine retention over a reasonable duration and establishing a low-pressure reservoir. The establishment of a low-pressure voiding mechanism is crucial for mitigating upper tract damage, primarily through the alleviation of vesicoureteric reflux and the prevention of complications associated with secondary infections of the upper urinary tract [13]. This case presented with bladder contracture, ureteral stenosis, and kidney hydronephrosis, which are uncommon complications of TB. It’s unusual for a patient to have such significant urinary tract issues without showing classic TB symptoms. The combination of bladder contracture, ureteral stenosis, and kidney hydronephrosis in the absence of typical TB symptoms makes this case noteworthy and challenging to diagnose. Augmentation, ureter reimplantation, urine control, and urination were good, and hydronephrosis was corrected.
The early detection of renal tuberculosis is crucial in preventing the progressive destruction of the kidney [14]. Recent advancements have facilitated the early and rapid diagnosis of renal tuberculosis from renal biopsy specimens utilizing real-time PCR with 35- and 40-Cycle Threshold (CT) cutoff values. Comparative analysis revealed that real-time PCR employing a CT cutoff of 40 exhibited superior sensitivity compared to real-time PCR with a CT cutoff of 35. Additionally, genital tuberculosis has been implicated in the infertility of both men and women, with the majority of cases remaining undiagnosed due to the disease’s asymptomatic presentation [15]. Consequently, a heightened index of suspicion is imperative for the accurate diagnosis of genitourinary tuberculosis. For the confirmation of genitourinary TB in both men and women using urine samples, PCR analysis targeting the MPT-64 protein gene has previously been established as the most sensitive method, when compared to alternatives such as intravenous urography, bladder biopsy, or urine culture [16]. The utility of PCR targeting IS6110 or the 16S rRNA gene has also been evaluated in urine samples for the diagnosis of genitourinary TB [17]. Nested PCR, targeting the MTP-40 protein gene of Mycobacterium tuberculosis, has been reported to achieve a sensitivity of up to 100% [18] to ascertain the tubercular etiology of female infertility [19].
In consideration of these findings, the development of early diagnostic tools for genitourinary TB, particularly those based on PCR techniques, marks a substantial progression in the identification of TB in patients exhibiting atypical symptoms. This advancement highlights the critical need to include genitourinary TB in the differential diagnosis for patients presenting with non-standard urinary tract symptoms, even in the absence of traditional TB indicators. Furthermore, the imperative for surgical intervention in cases of genitourinary TB, encompassing reconstructive surgeries, stems from the disease’s capacity to inflict significant anatomical alterations and functional degradation. An integrative approach combining multidrug chemotherapy with carefully considered surgical strategies emerges as the optimal treatment paradigm, aiming primarily at the preservation and rehabilitation of renal function. The deliberation over surgical options should meticulously evaluate the severity of the damage and the prospects for functional recuperation following the operation.
Conclusion
This case report elucidates the complex management of Genitourinary Tuberculosis (GUTB) complications, such as contracted bladder and renal insufficiency, through advanced urological reconstructive techniques. The utilization of double “J” stents and the construction of an ileal neobladder in a patient exhibiting non-standard manifestations of GUTB underscores the imperative for bespoke treatment protocols. This narrative accentuates the significance of prompt diagnosis and customized surgical approaches in enhancing patient outcomes in cases of GUTB. It highlights the pivotal role played by precise surgical execution and a comprehensive, multidisciplinary approach in addressing extensive urinary tract damage. Our findings advocate for the inclusion of GUTB in the differential diagnosis, especially in patients with atypical urinary tract presentations, to ensure timely and efficacious management of PCR.
Declarations
Consent for publication: Written informed consent was obtained from the patient for publication of this case report.
Funding: No funding
Conflict of interest: There is no conflict of interest that the authors of this case are aware of.
Authors’ contribution: Maged write case report , all author read the case and they approve to publish.
Acknowledgment: The authors acknowledge all the frontline healthcare workers who participated in the management tuberculosis case.
References
- Organization WH. Global tuberculosis report 2013: World Health Organization. 2013.
- Cek M, Lenk S, Naber KG, Bishop MC, Johansen TEB, Botto H, et al. EAU guidelines for the management of genitourinary tuberculosis. European urology. 2005; 48(3): 353-62.
- Gupta N, Kumar R, Mundada O, Aron M, Hemal A, Dogra P, et al. Reconstructive surgery for the management of genitourinary tuberculosis: a single center experience. The Journal of urology. 2006; 175(6): 2150-4.
- Zajaczkowski T. Genitourinary tuberculosis: historical and basic science review: past and present. Central european Journal of urology. 2012; 65(4): 182.
- Figueiredo AA, Lucon AM. Urogenital tuberculosis: update and review of 8961 cases from the world literature. Reviews in urology. 2008; 10(3): 207.
- Figueiredo AA, Lucon AM, Junior RF, Srougi M. Epidemiology of urogenital tuberculosis worldwide. International journal of urology. 2008; 15(9): 827-32.
- Hong P, Ding G-P, Hao H, Yang K-L, Zhuang L-Y, Cai L, et al. Laparoscopic radical cystectomy with extracorporeal neobladder: our initial experience. Urology. 2019; 124: 286-91.
- Muneer A, Macrae B, Krishnamoorthy S, Zumla A. Urogenital tuberculosis—epidemiology, pathogenesis and clinical features. Nature Reviews Urology. 2019; 16(10): 573-98.
- Eastwood JB, Corbishley CM, Grange JM. Tuberculosis and the kidney. Journal of the American Society of Nephrology. 2001; 12(6): 1307-14.
- Abbara A, Davidson RN. Etiology and management of genitourinary tuberculosis. Nature Reviews Urology. 2011; 8(12): 678-88.
- Indudhara R, Vaidyanathan S, Radotra B. Urethral tuberculosis. Urologia internationalis. 1992; 48(4): 436-8.
- Gupta NP, Kumar A, Sharma S. Reconstructive bladder surgery in genitourinary tuberculosis. Indian Journal of Urology. 2008; 24(3): 382-7.
- Wesolowski S. Late Results of Cystoplasty in Chronic Tuberculous Cystitis 1. British Journal of Urology. 1970; 42(6): 697-703.
- Mehta PK, Raj A, Singh N, Khuller GK. Diagnosis of extrapulmonary tuberculosis by PCR. FEMS Immunology & Medical Microbiology. 2012; 66(1): 20-36.
- Rana T, Singh UB, Kulshrestha V, Kaushik A, Porwal C, Agarwal N, et al. Utility of reverse transcriptase PCR and DNA-PCR in the diagnosis of female genital tuberculosis. Journal of medical microbiology. 2011; 60(4): 486-91.
- Dinnes J, Deeks J, Kunst H, Gibson A, Cummins E, Waugh N, et al. A systematic review of rapid diagnostic tests for the detection of tuberculosis infection. Health technology assessment. 2007; 11(3).
- Van Zyl L, Du Plessis J, Viljoen J. Cutaneous tuberculosis overview and current treatment regimens. Tuberculosis. 2015; 95(6): 629-38.
- Altez-Fernandez C, Ortiz V, Mirzazadeh M, Zegarra L, Seas C, Ugarte-Gil C. Diagnostic accuracy of nucleic acid amplification tests (NAATs) in urine for genitourinary tuberculosis: a systematic review and meta-analysis. BMC infectious diseases. 2017; 17: 1-9.
- Bhanu NV, Singh UB, Chakraborty M, Suresh N, Arora J, Rana T, et al. Improved diagnostic value of PCR in the diagnosis of female genital tuberculosis leading to infertility. Journal of medical microbiology. 2005; 54(10): 927-31.