
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Device closure of post-infarct ventricular septal rupture
Rajeev Bhardwaj*; Saurav Mittal; Tania Pruthi
Department of Cardiology, MM Institute of Medical Sciences and Research, Mullana, Ambala, India.
*Corresponding Author : Rajeev Bhardwaj
Department of Cardiology, MM Institute of Medical Sciences and Research, Mullana, Ambala, India.
Email: rajeevbhardwaj_dr@yahoo.com
Received : July 01, 2024
Accepted : Jul 17, 2024
Published : Jul 24, 2024
Archived : www.jcimcr.org
Copyright : © Bhardwaj R (2024).
Abstract
Ventricular Septal Rupture (VSR) is rare but dreadful complication of Myocardial Infarction (MI). With medical treatment, mortality is very high. Even with surgery, the perioperative morbidity and mortality is high, though results are better than medical therapy. Device closure is less invasive than surgery and is a good alternative, especially in patients with cardiogenic shock. We present a case of VSR, in a patient of anterior wall MI, who was successfully managed by device closure’.
Keywords: Myocardial infarction; Septal rupture; Device closure.
Citation: Bhardwaj R, Mittal S, Pruthi T. Device closure of post-infarct ventricular septal rupture. J Clin Images Med Case Rep. 2024; 5(7): 3182.
Introduction
Ventricular Septal Rupture (VSR) is rare but dreaded complication of Acute Myocardial Infarction (AMI). In pre -thrombolytic era around 1-3% patients of AMI developed VSR [1,2]. In GUSTO-1 trial, the VSR was confirmed in 0.2% cases, indicating that incidence decreased after thrombolysis [3]. Rupture usually occurs 3-8 days after AMI. Patient suddenly develops cardiogenic shock, wih new murmur at apex. The condition has a high mortality and requires early intervention.
Case
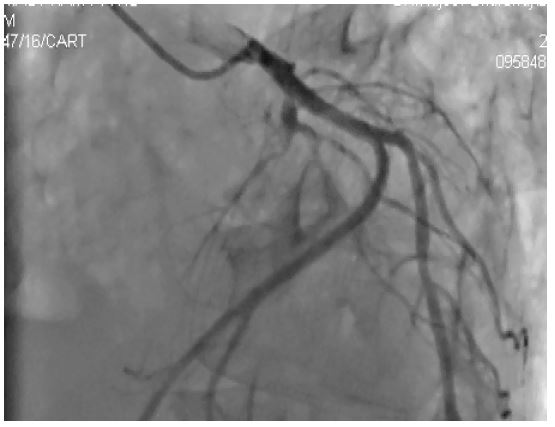
71 years male patient had chest pain around 2 weeks back, which lasted for around 2-3 hours. He did not seek any medical advice, as he thought it to be muscular in origin. He did not have any sweating or breathlessness at that time. He continued his normal activities, though he had some fatigue. For last four days, he developed breathlessness on walking a few steps. He also had history of (H/O) PND. On examination, his BP was 90/60 mmHg, heart rate 92/min. His JVP was raised. Chest showed bilateral basal crepts. His heart sounds S1 and S2 were normal. There was left ventricular S3 at apex. Pan systolic murmur was heard at apex, radiating to parasternal area. ECG showed Q waves and T wave inversion from V1 to V6, Echocardiography showed akinetic anterior wall. There was evidence of apical VSR, with left to right shunt (Figure 1). There was no mitral regurgitation. Left Ventricular (LV) Ejection Fraction (EF) was 32%. Coronary angiography showed total occlusion of Left Anterior Descending (LAD) artery in proximal part (Figure 2). Right coronary and left circumflex arteries were normal. LV angiography showed evidence of apical VSD (Figure 3). Surgeons did not take up the case due to high risk. So, it was decided to take up the case for device closure
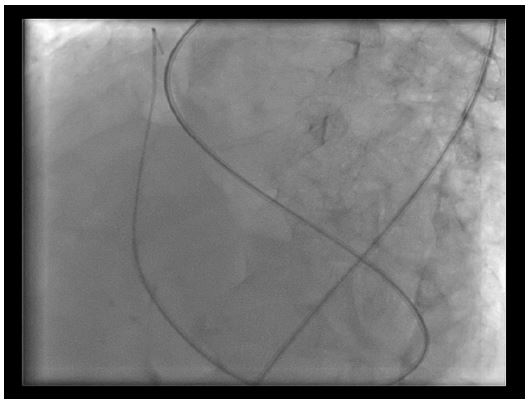
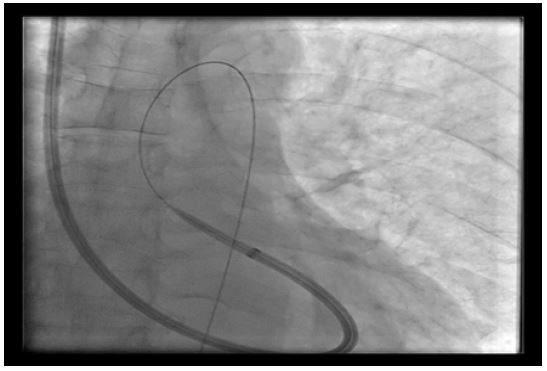
Right femoral approach was taken. VSD was crossed from Left Ventricular (LV) side with right Judkin’s catheter and Amplatzer wire was passed through it into the Pulmonary Artery (PA) (Figure 4). From internal jugular venous approach, this wire was snared from PA, out of internal jugular vein, making arterio-venous loop (Figure 5). 12F Mullin sheath was then negotiated from venous side into LV (Figure 6). Then 16 mm Amplatzer VSD occluder was deployed (Figure 7). Patient tolerated the procedure well and was discharged after 4 days, after his heart failure was well controlled. His echocardiography showed well placed device (Figure 8). He is on regular follow up for more than 4 years and is presently in NYHA class 1.


Discussion
In 1847, Latham first mentioned the diagnosis of VSR. VSR usually occurs in full thickness myocardial infarction, (Transmural) and is rare now due to aggressive reperfusion approach in management of STEMI. Female gender, late or no reperfusion, first MI, prior stroke and higher Killip class are risk factors for VSR [4,5]. LAD supplies most of the anterior part of IVS and VSD in anterior wall MI is apical in location. Dominant RCA supplies the posterior part of septum and VSR in inferior wall MI involves the basal septum. Patient usually presents with sudden left ventricular failure or flush pulmonary oedema 3-7 days after stable MI. Auscultation will reveal loud pansystolic murmur, heard over the precordium, which has to be differentiated from acute mitral regurgitation. Urgent echocardiography will differentiate the two.
Becker has proposed 3 types of VSR [6].
Type I: Sudden in onset, slit-like tear, within 24 hours.
Type II: Subacute, erosion of infarcted myocardium.
Type III: Late presentation, aneurysm formation, and rupture, associated with older infarcts.
In Shock registry [5], LAD artery was responsible for 42% cases of VSR and RCA for 46%. Apical VSRs are typically simple, occurring at the same level on both sides of septum. On the other hand, basal VSRs are usually complex, taking serpegenous course. With medical treatment the mortality of post MI VSR is very high. In GUSTO trial, 30 day mortality in 34 patients subjected to surgical repair was 47%, in contrast to 94% in 35 patients kept on medical therapy [3]. Medical management involves afterload reduction with intravenous nitroprusside and/or intra-aortic balloon counterpulsation to decrease shunting. Intravenous diuretics may reduce pulmonary congestion. Vasopressors are usually required to stabilize the patients for surgical repair.At present surgery is recommended to all Patients with Post MI VSR (PIVSR). ACCF/AHA guidelines propose that these patients should be operated immediately irrespective of the hemodynamic status due to high mortality associated with delay [7]. However, the 2017 European Cardiology Society’s Acute Myocardial Infarction Management Guidelines recommend that due to high mortality associated with early surgery, in patients who are stable, surgery should be delayed. Early surgery has higher risk because of fragile myocardium and risk of residual shunt8. Papalexopoulou et al. [9] evaluated six large studies including 3,238 patients who underwent surgery for PIVSR. In-hospital mortality was 52.4% in patients who underwent surgical repair in the first 3 days to 4 weeks and 7.56% in patients who underwent delayed surgical treatment 1-4 weeks later. Still there is no consensus on the timing of surgery. Delayed surgery has better prognosis, but by 3-4 weeks, many patients would have succumbed, waiting for surgery, on medical therapy. So broadly, early surgery should be done in patients with VSR size >15 mm, patients in cardiogenic shock or if there is hemodynamic detedeterioration. In hemodynamic stable patients, surgery should be delayed for 3-4 weeks,as by that time marginal tissue scar occurs after VSR maturity.
Transcatheter device closure is an alternative to surgery, especially for high surgical risk cases or residual shunt after surgical closure. Thiele et al. [10] reported 29 cases in a single centre over a 6-year period. Closure was done within one to three days of MI. Procedural success was 86%. However, 17% patients died in catheterization laboratory only. Only 35% survived one month. Holzer et al. [11] in US did device closure in PIVSR after 2 weeks of MI. Procedural success was in 16 out of 18 patients. One month survival was 72%. This clearly shows the value of delayed intervention, but at the cost of overall survival. Our case came 2 weeks after MI, had not taken any treatment for MI, as he was not aware of his disease. Device closure was done after around 16 days of MI and patient tolerated the procedure well and had good longterm health. VSR size was 10 mm, but due to apprehension of friable margins, and risk of embolization, larger device size was chosen.
References
- Pohjola-Sintonen S, Muller JE, Stone PH, et al. Ventricular septal and free wall rupture complicating acute myocardial infarction: experience in the Multicenter Investigation of Limitation of Infarct Size. Am Heart J. 1989; 117: 809-818.
- Radford MJ, Johnson RA, Daggett WM Jr, et al. Ventricular septal rupture: a review of clinical and physiologic features and an analysis of survival. 1981; 64: 545-553.
- Crenshaw BS, Granger CB, Birnbaum Y, et al. Risk factors, angiographic patterns, and outcomes in patients with ventricular septal defect complicating acute myocardial infarction. 2000; 101: 27-32.
- Crenshaw BS, Granger CB, Birnbaum Y, et al. Risk factors, angiographic patterns, and outcomes in patients with ventricular septal defect complicating acute myocardial infarction. 2000; 101: 27-32.
- López-Sendón J, Gurfinkel EP, Lopez de Sa E, et al. Factors related to heart rupture in acute coronary syndromes in the Global Registry of Acute Coronary Events. Eur Heart J. 2010; 31: 1449-56.
- Menon V, Webb JG, Hillis LD, et al. Outcome and profile of ventricular septal rupture with cardiogenic shock after myocardial infarction: a report from the SHOCK Trial Registry. SHould we emergently revascularize Occluded Coronaries in cardiogenic shocK? J Am Coll Cardiol. 2000; 36: 1110-6.
- Becker AE, van Mantgem JP. Cardiac tamponade. A study of 50 hearts. Eur J Cardiol. 1975; 3(4): 349-58.
- Endorsed Endorsed by the Latin American Society of Interventional Cardiology PCI WRITING COMMITTEE, Levine GN, Bates ER, Blankenship JC, Bailey SR, et al. 2015 ACC/AHA/SCAI focused update on primary percutaneous coronary intervention for patients with ST-elevation myocardial infarction: An update of the 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention and the 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation. 2016; 133: 1135-47.
- Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, et al. ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018; 39: 119-77.
- Papalexopoulou N, Young CP, Attia RQ. What is the best timing of surgery in patients with post-infarct ventricular septal rupture? Interact Cardiovasc Thorac Surg. 2013; 16: 193-96.
- Thiele H, Kaulfersch C, Daehnert I, Schoenauer M, Eitel I, et al. Immediate primary transcatheter closure of postinfarction ventricular septal defects.Eur Heart J. 2009; 30: 81-88.
- Holzer R, Balzer D, Amin Z, Ruiz CE, Feinstein J, et al. Transcatheter closure of postinfarction ventricular septal defects using the new Amplatzer muscular VSD occluder: results of a U.S. Registry.Catheter Cardiovasc Interv. 2004; 61: 196-201.