
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 5
Ancillary findings of tumor thrombus on F-18 FDG PET/CT besides intravascular FDG uptake
Deepanksh Datta; Rajesh Kumar*
All India Institute of Medical Sciences, Jodhpur, India.
*Corresponding Author : Rajesh Kumar
All India Institute of Medical Sciences, Jodhpur, India.
Tel: +91-9448107545;
Email: rajesh.nmd@gmail.com
Received : Jul 05, 2024
Accepted : Jul 17, 2024
Published : Jul 24, 2024
Archived : www.jcimcr.org
Copyright : © Kumar R (2024).
Abstract
Objective: The aim of the study is to investigate additional findings associated with tumor thrombus on F-18 FDG PET/CT other than intravascular metabolic activity such as direct or indirect extension with the primary tumor, association between metabolic activity of primary tumor & tumor thrombus and incidence of distant metastases.
Materials and methods: This is a retrospective study done in the Department of Nuclear Medicine at a tertiary care hospital in India. The patients with known malignancies and who underwent F-18 FDG PET/CT in the department for 27 months (2020-2023) were screened for tumor thrombus that comprised the study group. The morphological parameters analyzed included extension with the primary tumor (direct / indirect), incidence (presence or absence) of distant metastases, metabolic activities of the tumor thrombus, primary malignant site and distant metastases.
Statistical analysis: Descriptive statistics was done for data using SPSS v22.Metabolic values (SUV max) were expressed as median and inter-quartile range. Comparison between the metabolic activities of the tumor thrombus, primary tumor and distant metastases was calculated using Mann-Whitney U test.
Results: Of 2870 FDG PET/CT studies of patients with known malignancy screened, 12 patients had tumor thrombus and 25 vessels were involved. The most common primary sites of malignancy were lymphoma and liver (21.4% each) and the most common vessel involved was IVC and SVC (20% each). The median (inter-quartile range, IQR) of metabolic activity (SUVmax in g/ml) of primary tumor and tumor thrombus were 10.5 (12.5) and 5.5 (9.6) respectively. 60% of the tumor thrombus was contiguous with the primary tumor. 85.7% patients had distant metastases at the time of presentation of tumor thrombus. Significant association was noted between the metabolic activities of primary malignant site and tumor thrombus (p<0.05) on Mann Whitney U test. No significant association was noted between the metabolic activities of the tumor thrombus and distant metastases.
Conclusion: Tumor thrombus is usually a direct extension of the primary tumor with metabolic activity similar to the primary malignancy. However it can also present as a non-contiguous intravascular lesion away from the primary malignant site. It is usually associated with distant metastases at the time of presentation.
Keywords: Tumor thrombus; F-18 FDG PET/CT; Extension; Noncontiguous; Metastases.
Citation: Datta D, Kumar R. Ancillary findings of tumor thrombus on F-18 FDG PET/CT besides intravascular FDG uptake. J Clin Images Med Case Rep. 2024; 5(7): 3183
Introduction
Tumor Thrombus (TT) is a rare but aggressive feature of any solid malignancies that can occur in staging or post treatment status. It is defined as proliferation of tumor cells inside the vessel lumen that can occur either by primary malignancy invading the nearby vessel or by extension of the tumor into the vessel [1]. Its presence is reported to be associated with adverse outcomes and the surgical planning becomes more complex. Its incidence depends on type of primary malignancy and is most commonly seen in primary renal and liver malignancies [2]. Identification of TT is challenging as there are no specific clinical symptoms, nor it is restricted to any stage of malignancy. The CECT (Contrast-enhanced Computed Tomography) and CE-MRI (Contrast-enhanced Magnetic Resonance Imaging) can aid in distinguishing it from bland thrombus by presence of contrast enhancement and direct continuation of the primary tumor mass as characteristic of tumor thrombus. Multiple studies suggest intravascular uptake of F-18 FDG (F-18 2-fluoro 2-deoxy D-glucose) on PET/CT (Positron Emission Tomography) as confirmation of tumor thrombus [2-16]. With this study, we emphasis on the morphological features besides intravascular FDG uptake that can be associated with tumor thrombus such as
1. Contiguity or Non-contiguity with the primary malignancy: direct or indirect extension of the tumor,
2. Presence or absence of distant metastases at the time of diagnosis of TT, and
3. Association between the metabolic activities of TT and primary tumor.
Materials and methods
Study setting and patient criteria: This was a retrospective study conducted in a tertiary care referral university hospital in North India. This study was approved by the Institute Ethics Committee (IEC no. AIIMS/IEC/2023/4333).
All the F-18 FDG PET/CT scans of patients with biopsy proven malignancy performed in the department from February 2020 to May 2023, were screened for tumor thrombus. Presence of linear or focal intravascular FDG uptake with or without contrast enhancement was considered positive for tumor thrombus and included in the study. As few patients underwent non iodinated contrast PET/CT, intravascular contrast enhancement was not considered mandatory as the inclusion criteria.
Acquisition of 18-FDG PET/CT: F-18 FDG PET/CT imaging was carried out in accordance with the standard clinical PET/CT protocol as per the EANM guidelines [17]. The patients were intravenously injected with F 18 FDG; 3.7 MBq/kg body weight to a maximum dose of 370 MBq after a 4-6 h fasting period. All patients were imaged with an integrated PET CT system (Discovery GE MIDR 710). After 45-60 minutes of uptake period at rest, in a dimly lit quiet room, the images were acquired at 1 min per bed position. In the patients with serum creatinine and blood urea nitrogen under normal limits and with no other contraindications to iodinated contrast, the PET scan was acquired together with the CECT (contrast enhanced computed tomography) scan, otherwise a non-contrast CT was acquired. In those with the PET/CECT, a delay of 35 seconds was between the intravenous iodinated contrast injection and acquisition of CT scan.
Table 1: Study characteristics.
| Patients with Tumor Thrombus = N | 14 |
|---|---|
| Median Age in years (range); M:F | 55 (8-76); 7:7 |
| Primary malignant sites [N=14] | |
| Lung (n) [%] | 3 (21.4%) |
| Lymphoma | 3 (21.4%) |
| Liver | 2 (14.3%) |
| Bone | 2 (14.3%) |
| Kidney | 2 (14.3%) |
| Thyroid (poorly differentiated) | 1 (7.1%) |
| Cervix (poorly differentiated) | 1 (7.1%) |
| Veins Involved [N= 25] | |
| IVC n (%) | 5 (20%) |
| SVC | 5 (20%) |
| Iliac | External iliac =3 (12%)/ Common iliac= 2 (8%) |
| Brachiocephalic | 3 (12%) |
| Portal Vein | 2 (8%) |
| Renal / IJV/ Pulmonary | 1 (4%)/1 (4%)/ 1 (4%) |
| Extent of the tumor thrombus [N= 25] | |
| Continuous with Primary malignancy/direct | 15 (60%) |
| Non-contiguous/Indirect with primary | 10 (40%) |
Presence of intra-vascular FDG uptake (linear or focal) was considered positive for tumor thrombus, and served as the only inclusion criteria. This finding was supplemented by the presence of filling defect in the vessels on CECT if available. In those patients in which non-contrast PET/CT was done, the confirmation of PET positive tumor thrombus was confirmed by regional ultrasound or MRI. The findings on PET/CT were independently verified by two Nuclear Medicine physicians each with more than 5 years of experience. Those scans with either one disagreement were excluded from the study.
Parameters recorded
The morphological and metabolic parameters recorded and analyzed in this study were as follows;
1. Metabolic activities of the Tumor Thrombus (TT), primary tumor and distant metastases in terms of SUV max normalized to lean body mass (g/ml)
2. The extent of the tumor thrombus, i.e. direct extension /continuity, or non contiguity with primary tumor.
3. Imaging evidence of distant metastases at the time of diagnosis of TT.
Median and inter-quartile range of the metabolic parameters (SUVmax) were recorded. Association between the metabolic activities of the tumor thrombus, primary tumor and distant metastases was calculated using Mann-Whitney U test. Other morphological parameters (extent of thrombus and distant metastases) were nominal variables and percentage of incidence was calculated.
Results
The study and individual patient characteristics are shown in the Table 1 and Table 2 respectively. Of 2870 F-18 FDG PET/ CT studies screened, 12 patients had tumor thrombus with an incidence rate of 0.42%. 10 patients were diagnosed with tumor thrombus on their baseline PET/CT scans, and 2 patients (lymphoma, Carcinoma cervix) were diagnosed during their restaging scans which were suggestive of disease progression. Median age of the patients was 55 years (range: 8-76 years), and 50% (7/14) were males. The most common primary malignancies were liver and lymphoma (21% = 3/14 each). A total of 25 vessels were involved, of which the most common were IVC and SVC (20% = 5/25) each.
Table 2: Individual patient characteristics.
| Patient number | Age / Gender | Primary malignant site / SUVmax | Site of TT | SUVmax TT (g/dl) | Extension of TT | Distant metastases |
|---|---|---|---|---|---|---|
| 1. | 71/F | Thyroid/ 26 | RightIJV & Brachiocephalic vein | 10.4 | Direct | Lung,bone |
| 2. | 8/M | Anaplasticlymphoma/18.4 | SVC | 12.4 | Indirect | Peritoneum |
| 3. | 74/M | Liver/6.3 | Portalvein | 2.8 | Direct | Lung,ascites |
| 5. | 76/F | Lung/10.5 | SVC,Right brachiocephalic vein, Right atrium | 9.2 | Direct | Internalmammary nodes, pleura |
| 6. | 49/M | Renal/6.2 | Rightrenal vein, IVC, Right atrium | 8.9 | Indirect | None |
| 7. | 58/F | Renal/6.7 | InfrarenalIVC | 5 | Indirect | lung |
| 8. | 15/F | Bone/7 | Bilateralexternal & common iliac veins and IVC | 3.6 | Direct | lung |
| 9. | 72/M | Lung/17.7 | SuprahepaticIVC | 5.1 | Indirect | Bone,pleura, spleen |
| 10. | 32/F | Hodgkins’lymphoma/18.8 | InfrahepaticIVC | 14.2 | Direct | Liver,marrrow |
| 11. | 55/M | Lung/18.7 | SVC | 5.5 | Direct | Axillarynode, bone, liver |
| 12. | 63/F | Liver/ 9.2 | Rightlower lobar pulmonary vein | 2 | Indirect | Liver,peritoneum, ovaries |
| 13. | 21/M | Bone/2.9 | Externaliliac vein | 1.5 | Indirect | none |
| 14. | 75/M | Liver/6.1 | SuprahepaticIVC | 2.3 | Direct | Lung,ascites |
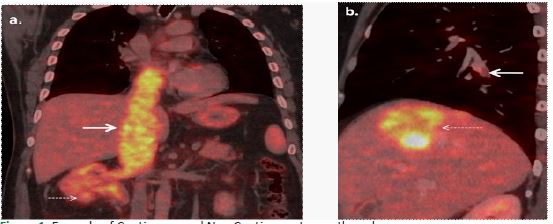
a) A case of primary renal cell carcinoma (dotted white arrows) with contiguous/direct extension of the tumor thrombus into IVC reaching up to right atrium (bold white arrows).
b) A case of primary cholangiocarcinoma (dotted white arrows) with non-contiguous tumor thrombus in right inferior pulmonary vein (bold white arrows), which was lateral confirmed on CT Pulmonary angiography.
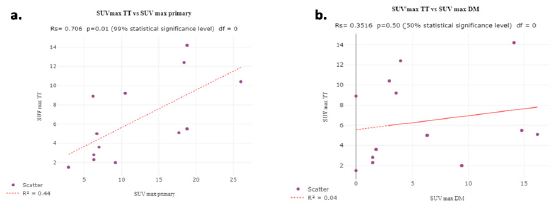
a) SUVmax TT and Primary malignancy.
b) SUVmax TT and Distant metastases.
Table 3: Distant metastases.
| Total n [%] | 12 [85.7%] |
| Lung / Pleura | 8 |
| Bone / Marrow | 5 |
| Non regional lymph nodes | 3 |
| Peritoneum | 2 |
| Liver / Spleen/ovaries/ascites | 1/1/1/1 |
85.7% (12/14) patients had imaging evidence of distant metastases on F-18 FDG PET/CT at the time of diagnosis of TT (Table 3), of which lung/pleura were the most common sites (67%= 8/12). 60% (15/25) of the tumor thrombi were contiguous with the primary tumor, i.e. direct extension of the primary tumor. However, 40% (10/25) of them were non-contiguous from the primary tumor, i.e indirect in nature. Figure 1 shows the examples of contiguous and non-contiguous tumor thrombi.
The median (and IQR) of the metabolic activity (SUV max) of primary malignant site and tumor thrombus was 10.5 (12.5) g/ml and 5.5 (9.6) g/ml respectively. In the cases of lymphoma, the group of nodes with the highest metabolic activity in the same region as that of the tumor thrombus was recorded. There was significant association noted between the metabolic activities of primary malignant site and tumor thrombus on Mann-Whitney U test (p< 0.05), with Pearson’s correlation coefficient < 0.05 (Figure 2a). No significant correlation was noted in the metabolic activities of the tumor thrombus and distant metastases (Figure 2b). Neither any correlation was noted between the metabolic activities of the distant metastases and primary malignant site (p value=0.07).
Discussion
Tumor Thrombus (TT) is a known aggressive feature of any malignancy, and is usually seen in renal and hepatocellular primaries [1]. Detection of TT is crucial for staging and further management of the malignancy. The primary objective of this study was to find the features of TT on F-18 FDG PET/CT other than the intravascular FDG uptake.
In this study, the most primary malignancies were lung and lymphoma besides liver, suggesting that any malignancy can exhibit this growth pattern. The majority of the patients had imaging evidence of distant metastases at the time of presentation of tumor thrombus. This is an interesting finding, and can be interpreted as both the tumor thrombus and distant metastases have the same route of hematogenous spread. It also explains the poor prognosis and lesser overall survival in the patients with TT [2].
The second parameter studied is the extension of the tumor thrombus with primary malignant site. Though majority of the thrombi were direct extension or invasion of the primary tumor into the adjacent vessel, still some of the thrombi were found in the vessels away from the primary tumor suggesting tumor embolus. This suggests that the intra-vascular tumor proliferation can occur anywhere inside the vessels along the vascular drainage of the primary tumor site.
In CECT and CE-MRI, one important feature to detect TT is the enhancement pattern of the expansile intravascular lesion similar to that of the primary tumor site that differentiates it from the bland thrombus [13]. There is significant correlation (p< 0.05) observed between the metabolic activities (SUVmax) of the primary tumor and tumor thrombus, suggesting both entities sharing similar cellular origin. This feature can be useful in equivocal cases or with suspicious false positive findings of intravascular FDG uptake. If the amount of intravascular FDG uptake is similar to that of the primary tumor then the likelihood of tumor thrombus is higher. We also tried to find the associaassociation between the metabolic activities of the tumor thrombus and the distant metastases, however could not find any significant correlation between them.
There are few limitations of this study like retrospective design, small sample size, and mostly visual or qualitative parameters studied. A larger study might be needed to improve the reliability of the correlation between the metabolic activity of primary tumor and tumor thrombus. However, given the low prevalence of tumor thrombus it is unlikely that any such study will be feasible in a single center, and prospective studies are suggested.
Conclusion
Tumor thrombus is usually associated with distant metastases at the time of diagnosis. It is mostly contiguous with the primary tumor, however few cases can also embolise away from the primary tumor along the vascular drainage pathways. There is significant association between the metabolic activities of the tumor thrombus and primary tumor.
Declarations
Financial disclosure: The authors declare that no funds, grants or other support was received during the preparation of the manuscript.
Conflict of interest: The authors declare that they have no potential conflict of interests.
Acknowledgement: None.
References
- LeGout JD, Bailey RE, Bolan CW, Bowman AW, Chen F, et al. Multimodality Imaging of Abdominopelvic Tumors with Venous Invasion. RadioGraphics. 2020; 40: 2098-2116.
- Quencer KB, Friedman T, Sheth R, Oklu R. Tumor thrombus: incidence, imaging, prognosis and treatment. Cardiovasc Diagn Ther. 2017; 7: S165-177.
- Gupta P, Kramer EL, Ponzo F. FDG Uptake in Tumor Thrombus in Inferior Vena Cava from Rectal Cancer on Positron Emission Tomography. Clin Nucl Med. 2005; 30: 342.
- Sharma P, Kumar R, Jeph S, Karunanithi S, Naswa N, et al. 18F-FDG PET-CT in the diagnosis of tumor thrombus: Can it be differentiated from benign thrombus? Nucl Med Commun. 2011; 32: 782-788.
- D’Souza MM, Jaimini A, Sharma R, Tripathi M, Singh D, et al. 18F-FDG PET/CT in the diagnosis of tumor thrombus from anaplastic thyroid carcinoma in a young boy. Iran J Nucl Med. 2010; 18: 52-56.
- Ravina M, Hess S, Chauhan MS, Jacob MJ, Alavi A. Tumor thrombus: Ancillary findings on FDG PET/CT in an oncologic population. Clin Nucl Med. 2014; 39: 767-771.
- Davidson T, Goitein O, Avigdor A, Zwas ST, Goshen E. 18F- FDG-PET/CT for the diagnosis of tumor thrombosis. Isr Med Assoc J. 2009; 1: 69-73.
- Batra S, Doval DC, Batra U, Suresh P, Dhiman A, Talwar V. Gallbladder cancer with tumor thrombus in the superior vena cava. Hepatobiliary Pancreat Dis Int. 2010; 9: 325-328.
- Jacquet T, Huchet V, Bedoui M, Jehanno N. Tumor Thrombus on 18F-FDG PET/CT in Stage IV Plasmablastic Lymphoma. Clin Nucl Med. 2022; 47: e140-1.
- Beadsmoore CJ, Cheow HK, Sala E, Lomas DJ, Gibbs P, et al. Hepatocellular carcinoma tumour thrombus in a re-canalised para-umbilical vein: detection by 18-fluoro-2-deoxyglucose positron emission tomography imaging. Br J Radiol. 2005; 78:841-844.
- Kaida H, Ishibashi M, Kurata S, Uchida M, Hayabuchi N. Tumor thrombus in the inferior vena cava from colon cancer detected by 18F-FDG-PET. Ann Nucl Med. 2007; 21: 185-188.
- Kurtovic J, Van Der Wall H, Riordan SM. FDG PET for Discrimination between Tumor Extension and Blood Thrombus as a Cause for Portal Vein Thrombosis in Hepatocellular Carcinoma: Important Role in Exclusion of Transplant Candidacy. Clin Nucl Med. 2005; 30: 408.
- Lee EYP, Khong PL. The Value of 18F-FDG PET/Contrast-Enhanced CT in Detection of Tumor Thrombus. Clin Nucl Med. 2013; 38: e60.
- Nguyen BD. Pancreatic Neuroendocrine Tumor with Portal Vein Tumor Thrombus: PET Demonstration. Clin Nucl Med. 2005; 30: 628.
- Peker AA, Toprak H, Yasin AI, Aydin M. Uncommon Testicular Germ Cell Tumor Thrombus in Azygos Vein Detected by FDG PET/CT. Clin Nucl Med. 2021; 46: e347-348.
- Probst S, Seltzer A, Chachoua A, Friedman K. Azygos venous tumor thrombus from renal cell carcinoma detected by F-18 FDG PET/CT. Clin Nucl Med. 2010; 35: 832-833.
- Boellaard R, Delgado-Bolton R, Oyen WJG, Giammarile F, Tatsch K, et al. FDG PET/CT: EANM procedure guidelines for tumour imaging: version 2.0. Eur J Nucl Med Mol Imaging. 2015; 42: 328-354.