
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 5
Congenital teratoma of the neck: A case report
Romaissa Kadraoui*; Manal Merbouh; Houssam Eddine Sahraoui; Youssef Mouaffak; Said Younous
Pediatric Intensive Care Unit, University Hospital Mohammed VI of Marrakech, Morocco.
*Corresponding Author : Romaissa Kadraoui
Pediatric Intensive Care Unit, University Hospital Mohammed VI of Marrakech, Morocco.
Email: roma-sa@hotmail.com
Received : Jul 01, 2024
Accepted : Jul 22, 2024
Published : Jul 29, 2024
Archived : www.jcimcr.org
Copyright : © Kadraoui R (2024).
Abstract
Congenital teratomas are relatively rare neoplasms, which occurs in about 1:20,000 to 1:80,000 births, and only 1.5% to 5% of which are neoplasm of the cervical. They can be diagnosed through ultrasound during pregnancy and, if not properly handled, have a high mortality rate. Airway compression is a secondary complication following mortality. We report 1 case collected in the paediatric intensive care unit of the CHU MOHAMED VI in Marrakech, in which we highlight that there is still a lack of antenatal diagnosis, despite improvements in the management of newborns. Although congenital teratomas are a rare condition with complex treatment, it is possible to achieve a satisfactory outcome when adequate planning and protocol are established.
Keywords: Congenital; Teratoma; Neck; Surgical treatment.
Citation: Kadraoui R, Merbouh M, Sahraoui HE, Mouaffak Y, Younous S. Congenital teratoma of the neck: A case report. J Clin Images Med Case Rep. 2024; 5(7): 3186.
Introduction
Fetal teratomas are rare, the reported incidence is between 0.07 and 2.8 in 1000 pregnancies [1]. It can be clinically dramatic, although essentially benign [2]. Most commonly found in the sacrococcygeal region, these tumors are rare in the neck region. The cervical area is exceptionally affected [3]. The symptoms are mostly attributed to the mass effect of these lesions, making the cervical tumors potentially lethal [4].
Most teratomas occur as an isolated lesion, but sometimes are part of a syndrome, such as Klinefelter syndrome, trisomy 13, trisomy 21, or Beckwith-Wiedemann syndrome [5]. Mortality is significant but prognosis is good with airway control and complete surgical excision [6]. The aim of our work by reporting a rare case of congenital teratoma is to produce a review about its etiology, diagnosis, prognosis and treatment.
Case report
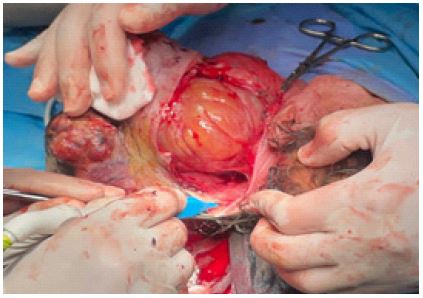
The newborn was female, with no previous history, and was admitted with a left cervical mass since the birth. Examination revealed a tonic, responsive and spontaneously gesticulating newborn with a heart rate of 102 beats/min and a respiratory rate of 32 cycles/min, with no signs of inflammation or dyspnea. A voluminous, painless, polylobed, latero-cervical cystic mase, about 43/42 cm in diameter, with telangiectasias and active bleeding. Biological tests showed an elevated alpha-fetoprotein level of 66400. Cervical CT revealed a triple-component laterocervical mass with locoregional extension and early endocranial extension. Cervical MRI revealed a well encapsulated left cervical mass independent of the subarachnoid spaces, with a very heterogeneous signal. Treatment consisted of total surgical excision of the mass at 30 days of age. Anatomopathological study was in favor of a pluritissular teratoma, with an immature neuroblastic component estimated at 10% of blastema, and a mature component at 90%. The evolution was not good, the patient died.


Discussion
Teratomas are known to occur anywhere in the body the commonest location being sacral region. Cervical presentation constitutes 1.6-9.3% of all pediatric teratomas, roughly equating to 1 per 40,000 births. They predominate in females (3/4 of the cases) [7]. Its volume, preventing normal growth of the foetus, may be responsible for hypotrophy or prematurity. The germ cells or primary gonocytes migrate to the yolk sac during the 1st weeks of intrauterine life and colonise the sexual cord, forming undifferentiated primitive gonads. They may stop during their migration to transform and form a benign or malignant germ cell tumour, which may be located from the head to the coccyx of the child [8,9].
Mature teratomas consist of well-differentiated tissues and may be pure or have a histologic component of a mixed germ cell neoplasm. Immaturity does not equate to malignancy, as was previously thought and less than 5% of congenital cervical teratomas are malignan [10]. Immature teratomas may be a component of a malignant germ cell tumor of mixed histology. The malignant component of mixed histology tumors that contain teratoma is usually of germ cell origin (yolk sac tumor, germinoma, embryonal carcinoma, or choriocarcinoma) and only rarely of somatic origin [11]. Clinically, a cervical teratoma appears as a large single mass, although multiple lesions may occur. Airway obstruction is the main complication and is related to the size and site of the lesion occurring in 80% to 100% of cases. Peripartum mortality is often related to difficulty in establishing an airway after delivery [17]. The diagnosis of congenital cervical teratomas may be made in the antenatal, perinatal or postnatal periods. With the advent of routine antenatal ultrasonography in populations, the number of unexpected cervical teratomas presenting at or after delivery has reduced [12,13]. Antenatal diagnosis may also be made following targeted ultrasonographic evaluation for polyhydramnios, which is present in 20% of cases [14]. Polyhydramnios occurs secondary to impaired foetal swallowing and is more commonly observed in larger tumours [15,16]. The differential diagnosis is done with a metastasis from thyroid carcinoma, cystic squamous cell carcinoma of cervical lymph node arising, follicular adenomas of the thyroid, lymphangiomas, and bronchial cysts [3]. The prognosis is mainly respiratory, when the volume of the mass is large and compresses the airways. This is why antenatal diagnosis is the key to effective management. Two techniques for artificial ventilation from birth before clamping the umbilical cord have been described, using a programmed caesarean section: EXIT (Ex-Utero Intra Partum Technique) where the fetal head is exteriorised to allow exploration of the airways, and intubation or even a tracheotomy if necessary; OOPS (Operation on Placenta Support) where the newborn is exteriorised in its entirety and placed on a surgical table to examine the airways. These techniques require maximum uterine relaxation, which may be responsible for serious uterine haemorrhage, and complications for the newborn such as thrombocytopenia, ascites or pleurisy [18,19]. The EXIT and OOPS procedures are not entirely undangerous for the mother. Uterine relaxation necessary to avoid placental separation may increase hemorrhage from the uterus. This complication should be discussed with the parents before deciding on the procedure. In addition, they should be informed that a caesarian delivery may be necessary in future pregnancies [20]. In addition to the OOPS and EXIT procedures, other techniques have been proposed for managing neonates with complicated airways. Extra Corporeal Membrane Oxygenation (ECMO), cannulation of the umbilical vessels, or open fetal surgery, have all been suggested, but to the best of our knowledge, were never performed in patients with congenital cervical teratomas [21,22]. With good presurgical planning and complete surgical excision there is no recurrence and few complications. A regular and long-term follow-up is necessary to detect early recurrences [23]. The recurrence can occur in less than 10% of operated patients and can be treated with further surgery or chemotherapy. the prognosis is mainly respiratory, when the volume of the mass is large and compresses the airways. Antenatal diagnosis allows good management [24].
Conclusion
Cervical teratomas are rare. Treatment is surgical. An early complete surgical approach to congenital cervical teratomas allows good results, with low rates of complication and recurrence.
References
- Simonini C, Strizek B, Berg C, Gembruch U, Mueller A, et al. Fetal teratomas-A retrospective observational single-center study. Prenat Diagn. 2021; 41(3): 301-307. doi: 10.1002/pd.5872.
- Rothschild MA, Catalano P, Urken M, Brandwein M, Som P, et al. Evaluation and management of congenital cervical teratoma: case report and review. Archives of Otolaryngology-Head & Neck Surgery. 1994; 120(4): 444-448.
- Sellami M, Mnejja M, Ayadi L, Charfeddine I, Boudawara T, et al. Congenital teratoma of the neck: A case report and literature review. Egyptian Journal of Ear, Nose, Throat and Allied Sciences. 2015; 16(1): 101-104.
- Mohanty MK, Sahu P, Jaiswal AA, Singal R, Gupta S, et al. A huge immature cervical teratoma; antenatal diagnosis, and its management-an unusual entity. Journal of Clinical Neonatology. 2013; 2(1): 42-45.
- Paradis J, Koltai PJ: Pediatric teratoma and dermoid cysts. Otolaryngol Clin North Am. 2015; 48(1): 121-136.
- Elmasalme F, Giacomantonio M, Clarke KD, Othman E, Matbouli S. Congenital cervical teratoma in neonates case report and review. European journal of pediatric surgery. 2000; 10(04): 252-257.
- Uchiyama M, Iwafuchi M, Naitoh S, Matsuda Y, Naitoh M, et al. A huge immature cervical teratoma in a newborn: report of a case. Surgery today. 1995; 25: 737-740.
- Azizkhan R, Haase GM, Applebaum H, Dillon PW, Coran AG, et al. Diagnosis, management, and outcome of cervicofacial teratomas in neonates: A Childrens Cancer Group study. Journal of pediatric surgery. 1995; 30(2): 312-316.
- Sayan A, Karaçay Ş, Bayol Ü, Arıkan A. Management of a rare cause of neonatal airway obstruction: Cervical teratoma. 2007.
- Batsakis JG, El-Naggar AK, Luna MA. Teratomas of the head and neck with emphasis on malignancy. Annals of Otology, Rhinology & Laryngology. 1995; 104(6): 496-500.
- Silberman R, Mendelson IR. Teratoma of the neck: Report of two cases and review of the literature. Archives of Disease in Childhood. 1960; 35(180): 159.
- Shine NP, Sader C, Gollow I, Lannigan FJ. Congenital cervical teratomas: Diagnostic, management and postoperative variability. Auris Nasus Larynx. 2006; 33(1): 107-111.
- April MM, Ward RF, Garelick JM. Diagnosis, management, and follow‐up of congenital head and neck teratomas. The Laryngoscope. 1998; 108(9): 1398-1401.
- Rosenfeld CR, Coln CD, Duenhoelter JH. Fetal cervical teratoma as a cause of polyhydramnios. Pediatrics. 1979; 64(2): 176-179.
- Hirose S, Sydorak RM, Tsao K, Cauldwell CB, Newman KD, et al. Spectrum of intrapartum management strategies for giant fetal cervical teratoma. Journal of pediatric surgery. 2003; 38(3): 446-450.
- Jordan RB, Gauderer MW. Cervical teratomas: an analysis. Literature review and proposed classification. Journal of pediatric surgery. 1988; 23(6): 583-591.
- Bianchi B, Ferri A, Silini EM, Magnani C, Sesenna E. Congenital cervical teratoma: A case report. Journal of oral and maxillofacial surgery. 2010; 68(3): 667-670.
- Sichel JY, Eliashar R, Yatsiv I, Gomori JM, Nadjari M, et al. A multidisciplinary team approach for management of a giant congenital cervical teratoma. International journal of pediatric otorhinolaryngology. 2002; 65(3): 241-247.
- Hasiotoua Maria, Vakaki Marina, Pitsoulakis George, et al. Congenital cervical teratomas. Int J Pediatr Otorhinolaryngol. 2004; 68(9): 1133-9.
- Liechty KW, Crombleholme TM, Flake AW, Morgan MA, Kurth CD, et al. Intrapartum airway management for giant fetal neck masses: the EXIT (ex utero intrapartum treatment) procedure. American journal of obstetrics and gynecology. 1997; 177(4): 870-874.
- Kelly MF, Greco R, Berenholz L, Wolfson P, Rizzo KA, et al. Approach for oxygenation of the newborn with airway obstruction due to a cervical mass. Annals of Otology, Rhinology & Laryngology. 1990; 99(3): 179-182.
- Stocks RMS, Egerman RS, Woodson GE, Bower CM, Thompson JW, et al. Airway management of neonates with antenatally detected head and neck anomalies. Archives of Otolaryngology–Head & Neck Surgery. 1997; 123(6): 641-645.
- Benouaiche L, Couly G, Michel B, Devauchelle B. Diagnosis and management of cervicofacial congenital teratomas: about 4 cases, literature review and restatement. In Annales de Chirurgie Plastique et Esthetique. 2006; 52(2): 114-123.
- Marina NM, Cushing B, Giller R, Cohen L, Lauer SJ, et al. Complete surgical excision is effective treatment for children with immature teratomas with or without malignant elements: A Pediatric Oncology Group/Children’s Cancer Group Intergroup Study. Journal of clinical oncology. 1999; 17(7): 2137-2143.