
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Aplastic anemia and guillain-barre syndrome after COVID-19 mRNA vaccination
Ashraf Ullah1*; Haseeb Haider2; Usama Ali Cheema3
1Internal Medicine, May Hospital Lahore, Pakistan.
2CMH, Institute of Medical Sciences, Multan, Pakistan.
3EM, Butch International Hospital, Multan, Pakistan.
*Corresponding Author : Ashraf Ullah
Internal Medicine, May Hospital Lahore, Pakistan.
Email: k.ashrafullah@gmail.com
Received : Jul 02, 2024
Accepted : Jul 25, 2024
Published : Aug 01, 2024
Archived : www.jcimcr.org
Copyright : © Ullah A (2024).
Abstract
This case report highlights the occurrence of Aplastic Anemia (AA) and Guillain-Barre Syndrome (GBS) following COVID-19 mRNA vaccination. After receiving the Pfizer-BioNTech mRNA vaccine, a 40-year-old man reported with continuous vomiting, epistaxis, and other related symptoms. A bone marrow sample and diagnostic studies both indicated severe aplastic anemia. The patient also experienced the onset of Acute Motor Sensory Axonal Neuropathy (AMSAN), a GBS variation. In addition to the lack of other known causes, the temporal link between vaccination and the development of both illnesses raises the possibility of a correlation. In order to better understand any potential correlations between uncommon adverse events following COVID-19 vaccines and autoimmune illnesses, this case highlights the significance of monitoring and reporting these events. Additional study is required to examine these connections on a bigger scale and assess risk factors.
Categories: Neurology, Pathology, Hematology.
Keywords: Guillain Barre’s Syndrome (GBS); Aplastic anemia; AEFI; COVID-19; Vaccination.
Citation: Ullah A, Haider H, Ali Cheema U. Aplastic anemia and guillain-barre syndrome after COVID-19 mRNA vaccination. J Clin Images Med Case Rep. 2024; 5(8): 3189.
Introduction
The World Health Organization (WHO) labeled the recent “Covid-19” coronavirus epidemic a pandemic in March 2020 after it significantly harmed the world’s health and financial resources. Therefore, creating urgent vaccines has become essential to reducing such a burden. Although COVID-19 vaccinations have a high safety score and reported efficacy, their potential link to uncommon adverse effects is still being investigated. There have been numerous reported Adverse Events Following Immunization (“AEFIs”) using COVID vaccinations.
One of the first adverse reactions to the COVID-19 vaccine that affects the nervous system is the unusual neurological illness known as Guillain-Barre Syndrome (GBS) [1]. GBS, also known as acute idiopathic polyneuritis, acute idiopathic polyradiculoneuritis, or Landry’s ascending paralysis, is an autoimmune disease that affects between 1.1 and 1.8 people per 100,000 years. After age 50, the incidence rises to between 1.7 and 3.3 people per 100,000 annually [2].
In Europe and the United States, the incidence of acquired Aplastic Anemia (AA), a rare Bone Marrow Failure (BMF) illness, is 2-3 cases per million people per year, while it is greater in East Asia [3]. Autoantibodies play a role as immunological factors in the development of AA in addition to T cells and cytokines [4].
Case presentation
40-year-old male presented to the medical outpatient department with a complaint of persistent vomiting for 15 days and a recent onset of epistaxis lasting for 2 days. The vomiting started suddenly and occurred 1-2 times per day, with each episode producing approximately half a cup of undigested food particles. The vomiting episodes were associated with food intake. The vomitus did not contain blood but had a foul odor and appeared yellowish. The patient also reported abdominal pain, headache, and intermittent undocumented fever spikes occurring 2-3 times per day. Furthermore, there was a history of weight loss and anorexia.
Two days before the presentation, the patient experienced a spontaneous nosebleed following an episode of vomiting. The nosebleed resolved spontaneously with pressure application. A total of four episodes had occurred before the patient visited the outpatient department. Additionally, the patient had received a booster dose of the Pfizer-BioNTech mRNA vaccine 18 days before the presentation. During the general physical examination, signs indicative of anemia were observed in the patient. No remarkable findings were noted in the gastrointestinal system, and the initial assessments of the respiratory and cardiovascular systems were unremarkable. Initial investigations showed abnormal results on complete blood count, including a white cell count of 1.4x103/μL, platelet count of 15x103/μL, and hemoglobin level of 10.5 g/dL. A Pancytopenia workup was initiated based on these findings. Serological tests for hepatitis B, hepatitis C, and Human Immunodeficiency Virus (HIV) were negative. Tests for Epstein-Barr Virus (EBV), Cytomegalovirus (CMV), and dengue virus were also negative. Vitamin B12 and folic acid levels were within the normal range (910 pg/ml and 7.6 ng/ml, respectively). Additional tests, such as complete blood count with peripheral smear, Liver Function Tests (LFTs), and Renal Function Tests (RFTs), were performed and the results are provided in Table 1. A bone marrow biopsy confirmed the diagnosis of aplastic anemia, as shown in Figure 1.
Based on the patient’s history, physical examination, and investigations, a diagnosis of aplastic anemia was established. According to the modified Camitta criteria, the final diagnosis was severe aplastic anemia. No other potential causes were identified for the aplastic anemia, except for the recent vaccination against SARS-CoV-2.
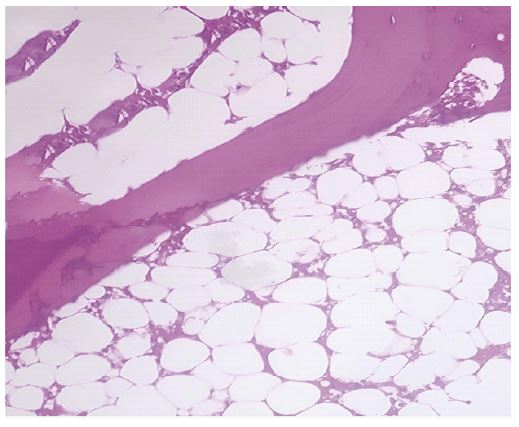
Table 1: Blood workup of patient showing various derangements.
| Hemogram | ||
|---|---|---|
| WBC count | 1.4 | 4-11 x109/ L |
| Total RBC 3.68 3.8-5.2 x1012/l | ||
| Hemoglobin | 10. 5 | 13-18 (g/ dL) |
| HCT 30.9 35-46% | ||
| MCV | 84 | 77-95 fl |
| Hemogram | ||
| MCH 27.7 26-32 (pg) | ||
| MCHC | 33 | 32-36 (g/ |
| dL) | ||
| Platelets 15 | ||
| 150-400 x109/L | ||
| Neutrophils | 28 | 40-80% |
| Lymphocytes 2 20-40% | ||
| Reticulocyt e s | 0.1 | 0.2-2% |
| % | ||
| Renal Function Tests | ||
| Urea | 55 | Oct-50 |
| mg/ dl | ||
| Serum Creatinine 1.2 0.5-0.9 mg/dl | ||
| Liver Functi on Tests | ||
| Bilirubin total 0.7 0.3-1.2 mg/ dl | ||
| Total protein | 5.6 | 5.7-8.2 g/ |
| dl | ||
| Albumin 3.1 3.2-4.8 g/dl | ||
| ALT | 252 | Up to 40 U/L |
| AST 142 Up to 40 U/L | ||
| ALP | 56 | 40-120 |
| U/ L | ||
| Serum Electrolytes | ||
| Sodium | 133 | 135-145 |
| mmol/L | ||
| Hemogram | ||
| Potassium 4.18 3.5-5 mmol/L | ||
| Chloride | 103 | 98-107 |
| mmol/L | ||
| Calcium 8.3 8.5-10.5 mg/dl | ||
WBC Count: White Blood Cells Count, RBC: Red Blood Cells, HCT: Hematocrit, MCV: Mean Corpuscular Volume, MCH: Mean Corpuscular Hemoglobin, MCHC: Mean Corpuscular Hemoglobin Concentration, ALT: Alanine Transaminase, AST: Aspartate Aminotransferase, ALP: Alkaline Phosphatase, ESR: Erythrocyte Sedimentation Rate.
On the seventh day of admission, the patient reported weakness and numbness in all four limbs. Upon examination of the motor system, generalized hypotonia and areflexia was observed in all limbs. The motor weakness was bilaterally symmetrical, more pronounced in the lower limbs (grade 1/5) compared to the upper limbs (grade 4/5). Sensory examination revealed bilateral paresthesia in the lower limbs, with no facial weakness or dysphagia.
Nerve conduction studies conducted at the time of presentation showed evidence of axonal sensorimotor polyradiculoneuropathy, characterized by weak F waves (Table 2).
Electromyography (EMG) performed at rest revealed significant denervation potentials. Neurophysiological investigations indicated modest amplitude motor and sensory responses in the lower limb, with no changes in velocity. Analysis of Cerebrospinal Fluid (CSF) aspiration showed a notable presence of albumin-cytologic dissociation. Based on the Brighton criteria, all these findings were consistent with acute motor sensory axonal neuropathy (AMSAN), a variant of Guillain-Barré Syndrome (GBS).
Table 2: Nerve conduction studies of lower limbs (A) and upper limbs (B).
| A. Motor Nerve Conduction Studies (NCS) | F-Wave Latency (ms) | Latency (ms) | Amplitude (µV) | Conducti o n velocity (m/s) | ||||
|---|---|---|---|---|---|---|---|---|
| Right Perone al | Distal | 40 (≤56) | 5.5 (≤6.5) | 0.8 (≥2) | 44 (44) | |||
| Proximal 14 (≤6.7) 1.6 (≥5) | ||||||||
| Left Perone al | Distal | 50 (≤56) | 3.9 (≤6.5) | 1.4 (≥2) | 47 (44) | |||
| Proximal 14.4 (≤6.7) 0.6 (≥5) | ||||||||
| Right Tibial | Distal | 5.0 (≤6.3) | 5.2 (≥3) | 46 (41) | ||||
| Proximal 15.6 (≤5.8) 1.9 (≥4) | ||||||||
| Left Tibial | Distal | 5.4 (≤6.3) | 6.5 (≥3) | 49 (41) | ||||
| Proximal 13 (≤5.8) 5.2 (≥4) | ||||||||
| Sensory NCS | ||||||||
| Right Sural 3.5 (≤4.4) 4.1 (≥6) 40 (≥40) | ||||||||
| Left Sural | 3.9 (≤4.4) | 3.1 (≥6) | 40 (≥40) | |||||
| B. Nerve Conduction Studies (NCS) | Lat en cy (ms ) | Amplitude (µV) | Conduction velocity (m/s) | |||||
| Right median | Distal | 4.1 (≤4. 4) | 4.2 (≥4) | 50 (≥49) | ||||
| Proximal 8.8 (≤4.4) 5.0 (≥4) | ||||||||
| Right Ulnar | Distal | 3.1 (≤3.3 ) | 8.1 (≥6) | 59 (≥49) | ||||
| Proximal 7.6 (≤4.5) 7.9 (≥7) | ||||||||
| Left Median | Distal | 3.6 (≤4.4 ) | 4.2 (≥4) | 60 (≥49) | ||||
| Proximal 8.4 (≤4.4) 3.8 (≥4) | ||||||||
| A. Motor Nerve Conduction Studies(NCS) | F-Wave Latency (ms) | Latency (ms) | Amplitude (µV) | Conducti o n velocity (m/s) | |||||
|---|---|---|---|---|---|---|---|---|---|
| Right Peroneal | Distal | 40 (≤56) | 5.5 (≤6.5) | 0.8 (≥2) | 44 (44) | ||||
| Proximal 14 (≤6.7) 1.6(≥5) | |||||||||
| Left Perone al | Distal | 50 (≤56) | 3.9 (≤6.5) | 1.4 (≥2) | 47 (44) | ||||
| Proximal 14.4(≤6.7) 0.6 (≥5) | |||||||||
| Sensory NCS | |||||||||
| Right Medain 2.0 (≤3.5) 25 (≥20) 60 (≥50) | |||||||||
| Right Ulnar | 1.9 (≤3. 0) | 26 (≥17) | 55 (≥50) | ||||||
| Left Median1.9 (≤3.5) 24 (≥20) 63 (≥50) | |||||||||
Based on the symptoms and investigations, a diagnosis of Guillain-Barre Syndrome (GBS) was made, with no other identified causative agents. Serological tests were conducted to rule out infectious agents such as Mycoplasma pneumoniae and varicella-zoster virus. The recent vaccination was the only factor that could be potentially associated with GBS, given the temporal relationship. It is worth noting that the occurrence of two rare autoimmune phenomena in a single patient following vaccination is not extensively documented in the literature.
The treatment approach for aplastic anemia involved supportive measures, blood transfusions, immunosuppressants, and stimulating factors. For the GBS, the patient was promptly transferred to the Intensive Care Unit (ICU). Fortunately, mechanical ventilation was not required, and Intravenous Immunoglobulins (IVIG) at a dose of 0.4 g/kg daily for 5 days were initiated. The patient responded positively to this treatment regimen and showed significant improvement. The patient was advised to undergo physiotherapy and to follow up after discharge. The patient visited the outpatient department once and demonstrated significant improvement in motor function, but unfortunately, they defaulted on further follow-up visits.
Discussion
According to reports, COVID-19 infections or vaccinations have been linked to the development of several autoimmune diseases. However, no standardized system has been established to assess the connections between vaccinations and the occurrence of autoimmune disorders.
Various vaccines are currently available, employing different mechanisms, such as modified mRNA vaccines, vector-based vaccines, inactivated COVID-19 viral vaccines, and vaccines utilizing recombinant protein components.
The onset of autoimmune disease following vaccination is rare. Only six documented cases of acquired Aplastic Anemia (AA) after vaccination have been reported [5]. It is not considered a common side effect of vaccination. Gathering data on adverse events related to SARS-CoV-2 mRNA vaccines is essential due to their unique mode of action. Post-vaccination, autoimmune diseases like autoimmune hepatitis, type 1 diabetes, immune thrombocytopenia, acquired hemophilia, and AA following COVID-19 infection have been reported. In our case, extensive investigations ruled out other causes and temporal associations linked AA to vaccination.
Epitope mimicry plays a key role in immune reactions [6]. Vaccine-induced antibodies have been suggested to share structural similarities with autoantibodies [7]. Extensive evidence supports the immune-mediated nature of Aplastic Anemia (AA), as shown by the success of immunosuppressive therapy. AA pathogenesis involves autoantibodies, T cells, and cytokines, although the exact role of autoantibodies in AA remains unclear. Allogeneic Hematopoietic Stem Cell Transplantation (HSCT) involves replacing the recipient’s hematopoietic and immune systems with those of the donor. Comparing vaccine antibody titers before and after allogeneic HSCT can help elucidate the pathophysiology of vaccine-associated autoimmune diseases.
To understand the connection between COVID-19 vaccination and the development of Aplastic Anemia (AA), it is crucial to investigate autoantibodies against stem cells, assess the importance of molecular mimicry between antigens encoded by mRNA vaccines and stem cells, and study the dynamics of T-cell subsets after vaccination [5].
Guillain-Barré Syndrome (GBS) is a common cause of acute flaccid paralysis characterized by acute inflammatory polyradiculoneuropathy. It presents with varying degrees of weakness, sensory abnormalities, and autonomic dysfunction. In two-thirds of patients, GBS is preceded by an upper respiratory or gastrointestinal infection. Notably, GBS cases have been reported following severe COVID-19 infection and vaccination. Several immunizations, including messenger RNA vaccines, adenovirus-vectored COVID-19 vaccines, and inactivated COVID-19 vaccines, have been associated with transient episodes of GBS [8]. The exact etiopathogenesis of GBS remains uncertain, but widely accepted theories involve molecular mimicry and immune- mediated mechanisms, such as the production of antiganglioside antibodies and complement activation [9].
In summary, the SARS-CoV-2 mRNA vaccination may have contributed to AA in this case. Further analysis is needed to investigate the association between AA and SARS-CoV-2 vaccinations in larger populations. Comprehensive epidemiological studies on the link between GBS and COVID-19 vaccination are lacking. However, reporting these rare adverse events promptly allows for timely identification and management of GBS cases and provides an opportunity for researchers to examine potential connections between AA, GBS, and COVID-19 vaccination.
Conclusion
It is essential to differentiate between autoimmune diseases and autoimmunity. Autoimmunity is a characteristic of a healthy and functioning immune system. In light of the COVID-19 vaccination, there appears to be a slightly increased risk of developing autoimmune diseases. The features of Guillain-Barre Syndrome (GBS) following vaccination are consistent with those seen before the COVID-19 era.
Future research should focus on examining the relationship between the timing of immunization and the onset of GBS and autoimmune illnesses, particularly in patients who have received mRNA vaccines. Additionally, it is important to conduct further epidemiological studies to assess the prevalence of autoimmune diseases following COVID-19 infection and SARS-CoV-2 vaccination. Preliminary research suggests that viral vector-based vaccines may pose a higher risk compared to other vaccine types. As more individuals receive vaccinations, it is hoped that reliable information regarding the actual incidence and risk factors associated with these conditions will become available.
Declarations
Human subjects: Consent was obtained or waived by all participants in this study.
Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following:
Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work.
Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work.
Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Acknowledgements: Ashraf Ullah carried out the Supervision and conceptualization. Haseeb Haider, Usama Ali Cheema,Mohammad Ahsan Anwaar and Shahzeb Saeed participated in the Writing and drafted the manuscript. Ali M. Abdelaziz and Muhammad Kamran conceived of the study, also participated in its design and coordination and helped to draft the manuscript.
References
- Aly AS, Alkolfat F, Mansour ER, Salama S. Guillain-Barre syndrome following COVID-19 vaccination: A case report and an updated review. Neuroimmunol Rep. 2022; 2: 100083. 10.1016/j.nerep.2022.100083.
- The Epidemiology of Guillain-Barré Syndrome Worldwide Neuroepidemiology Karger Publishers. 2023. https://karger.com/ned/article-abstract/ 32/2/150/210697/The-Epidemiology-of- Guillain-Barre-Syndrome.
- Pathogenesis of aplastic anemia. 2023. https:// pubmed.ncbi.nlm.nih.gov/31315542/.
- Dolberg OJ, Levy Y. Idiopathic aplastic anemia: Diagnosis and classification . Autoimmun Rev. 2014; 13: 569- 73. 10.1016/j.autrev.2014.01.014.
- Tabata S, Hosoi H, Murata S, Takeda S, Mushino T, et al. Severe aplastic anemia after COVID-19 mRNA vaccination: Causality or coincidence?. J Autoimmun. 2022; 126: 102782. 10.1016/j.jaut.2021.102782.
- Wraith DC, Goldman M, Lambert P-H. Vaccination and autoimmune disease: what is the evidence? The. Lancet. 2003; 362: 1659-66. 10.1016/S0140-6736(03)14802-7.
- Vaccination and autoimmune diseases: Is prevention of adverse health effects on the horizon? | Springer Link. 2023. https://link.springer.com/article/ 10.1007/s13167-017-0101-y.
- Tabatabaee S, Rezania F, Alwedaie SMJ, Malekdar E, Badi Z, et al. Post COVID-19 vaccination Guillain-Barre syndrome: Three cases. Hum Vaccines Immunother. 2022; 18: 2045153. 10.1080/21645515.2022.2045153.
- Guillain-Barré syndrome. 2023. https:// pubmed.ncbi.nlm.nih.gov/26948435/.