
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
The silent bronchial intruder: An insight into endobronchial hamartomas
Joana Vieira Naia*; Lurdes Ferreira; Rui Rolo
Pulmonology Department, Hospital of Braga, Braga, Portugal.
*Corresponding Author : Joana Vieira Naia
Pulmonology Department, Hospital of Braga, Braga, Portugal.
Email: joanavnaia@gmail.com
Received : Jul 05, 2024
Accepted : Jul 26, 2024
Published : Aug 02, 2024
Archived : www.jcimcr.org
Copyright : © Naia JV (2024).
Keywords: Endobronchial hamartoma; Benign lung neoplasm.
Citation: Naia JV, Ferreira L, Rolo R. The silent bronchial intruder: An insight into endobronchial hamartomas. J Clin Images Med Case Rep. 2024; 5(8): 3190.
Introduction
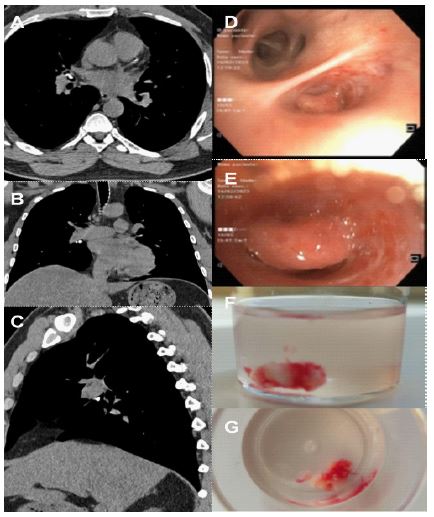
We present a 45-year-old non-smoking male, with a history of obesity and hyperuricemia, who was referred to a pulmonology appointment after performing a chest computed tomography, which revealed an irregular bone-density foreign body in the lumen of the middle lobar bronchus with 12 mm of size (Figure 1A-C). There were no lung-related symptoms relevant to this case and physical examination was unremarkable. The patient underwent a flexible videobronchoscopy that showed a firm and stiff endobronchial lesion, completely obstructing the middle lobar bronchus (Figure 1D and E), which was removed with biopsy forceps (Figure 1F and G). After removal, the middle lobar bronchus was completely unobstructed. Histological examination revealed a pulmonary hamartoma.
Pulmonary hamartomas are the most common benign neoplasms of the lung and most of them are in the peripheral parenchyma (90%). The endobronchial subtype represents nearly 10% of all lung hamartomas and is a rare and slow growing tumor [1].
The management of endobronchial hamartomas must be individualized, depending on symptoms, location of the lesion, and the preference/fitness of the patient. Bronchoscopy plays an essential role in the diagnosis and management of these tumors [2]. While the prognosis for these patients is good, there is a possibility of recurrence and transformation into malignancy. Therefore, follow-up is crucial [1].
Declarations
Contribution: Joana Vieira Naia: Investigation of the patient, writing of the manuscript. Lurdes Ferreira: Investigation of the patient, manuscript review. Rui Rolo: Investigation of the patient, manuscript review.
All the authors have read and approved the final version of the manuscript and agreed to be accountable for all aspects of the work.
Funding of the research: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of interest: The authors declare not to have any conflicts of interest that may be considered to influence directly or indirectly the content of the manuscript.