
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Primary endometriosis mimicking a strangulated umbilical Hernia: A case report and review of literature
Michael E Aghahowa1,2*; Alu FE3,4; Okonkwo DI5,6; Osisanya K7,8; Duum CN9; Gali BM1,2
1Department of Surgery, College of Health Sciences, Nile University of Nigeria, Abuja, Nigeria.
2Department of Surgery, Asokoro District Hospital, Abuja, Nigeria.
3Department of Obstetrics and Gynecology, College of Health Sciences, Nile University of Nigeria, Abuja, Nigeria.
4Department of Obstetrics and Gynecology, Asokoro District Hospital, Abuja, Nigeria.
5Department of Anatomic Pathology, College of Health Sciences, Nile University of Nigeria, Abuja, Nigeria.
6Department of Anatomic Pathology, Maitama District Hospital, Abuja, Nigeria.
7Department of Surgery, Baze University, Abuja, Nigeria.
8Department of Surgery, Maitama District Hospital, Abuja, Nigeria.
9Department of Obstetrics and Gynecology, Maitama District Hospital, Abuja, Nigeria.
*Corresponding Author : Michael E Aghahowa
Department of Surgery, College of Health Sciences, Nile University of Nigeria, Abuja, Nigeria.
Email: Michael.ehienagudia@nileuniversity.edu.ng & mikeaghahowa@yahoo.com
Received : Jun 20, 2024
Accepted : Jul 26, 2024
Published : Aug 02, 2024
Archived : www.jcimcr.org
Copyright : © Aghahowa ME (2024).
Abstract
Endometriosis is a benign gynaecological condition characterised by the presence of functional endometrial glands and stroma outside the uterine cavity. It commonly develops in the pelvis but can be found in other extra-pelvic sites. Umbilical endometriosis is rare and primary (spontaneous) umbilical endometriosis associated with umbilical hernia can present a diagnostic challenge to the surgeon as the presenting painful swelling may mimic an obstructed hernia. We present a 34-year old nulliparous woman who presented with a tender umbilical nodule with no previous abdominal surgical scar and no known history of endometriosis. A surgical excision of the nodule with umbilical herniorrhaphy was done and histological examination of the excised tissue confirmed a primary umbilical endometriosis. Further gynaecological evaluation was unremarkable and the patient has remained symptom-free. A high index of suspicion and a histopathological examination of the excised surgical specimen are mandatory for the diagnosis of primary umbilical endometriosis in a woman of reproductive age presenting with a tender umbilical nodule.
Keywords: Primary umbilical endometriosis; Umbilical hernia; Villar’s nodule; Surgical excision.
Citation: Aghahowa ME, Alu FE, Okonkwo DI, Osisanya K, Duum CN, et al. Primary endometriosis mimicking a strangulated umbilical hernia: A case report and review of literature. J Clin Images Med Case Rep. 2024; 5(8): 3191.
Introduction
Endometriosis is the presence of functional endometrial glands and stroma outside the uterine cavity. It is a common benign gynaecological condition, affecting 5-10% of women of reproductive age and found in at least a third of women undergoing a diagnostic laparoscopy for pelvic pain or infertility [1]. The condition is oestrogen-dependent and tends to resolve after the menopause. It is usually found within the pelvis, located along the peritoneum lining the pelvic side walls, pouch of Douglas, uterosacral ligaments and urinary bladder and bowel. It occurs less frequently in extra-pelvic sites including the umbilicus, surgical scars (especially after caesarean sections and in laparoscopic port sites), and pleural cavity, and occasionally develops spontaneously [1,2]. Endometriotic tissues respond to hormonal changes and undergo cyclical bleeding and local inflammatory reactions. The cyclical episodes of bleeding and healing lead to fibrosis and adhesion formation. Affected women traditionally present with severe cyclical non-colicky pelvic pain restricted to around the time of menstruation which may start a few days before the commencement of menstruation, and continue until the end of menstruation. The pain may be in form of dysmenorrhoea, deep dyspareunia, and dyschezia. Endometriosis is frequently associated with irritable bowel syndrome. Extra-pelvic endometriosis can cause local symptoms like cyclical epistaxis, cyclical haemoptysis/haemopneumothorax, cyclical rectal bleeding, cyclical haematuria, and cyclical pain, swelling and bleeding at abdominal surgical scars and the umbilicus [1]. The aetiology of endometriosis is unknown but several theories have been postulated to explain it, including the Sampson’s theory of retrograde menstruation, implantation theory (surgical implantation, vascular and lymphatic spread); coelomic metaplasia; and genetic and immunological factors [3].
Diagnosis is mainly clinical aided by ultrasound scan and laparoscopy. Laparoscopy is the traditional method of diagnosis which is based on the accurate visual identification of endometriotic lesions [4]. It has the added advantage of allowing biopsy of the lesions for histological confirmation of diagnosis and for concurrent surgical diathermy ablation and/or excision of the endometriotic lesions. Magnetic Resonance Imaging (MRI) is the imaging technique of choice for diagnosis as it can detect lesions of >5 mm in size [5]. Management of endometriosis includes both medical and surgical treatment, with medical treatment reserved only for preoperative relief of symptoms as it is associated with side effects and limited to short-term use [6].
Extra-pelvic endometriosis is rare and often presents a diagnostic challenge to the surgeon when evaluating a female who presents with cyclical pain, bleeding and/or swellings [3]. Umbilical endometriosis is rare and develops mainly in surgical scars. Primary Umbilical Endometriosis (PUE) without previous pelvic surgery is however extremely rare [6-8]. We present a 34-year old female who had an undiagnosed primary umbilical endometriosis but presented with features mimicking a strangulated umbilical hernia.
Case presentation
A 34-year old unmarried nulliparous lady who presented to the surgical outpatient clinic with a history of an umbilical swelling of 4 years duration associated with recurrent umbilical pain especially during her menstruation and with associated dysmenorrhoea and lower abdominal and pelvic pain relieved by ingestion of NSAIDs, but with no visible bleeding from the umbilicus. The swelling gradually increased in size over the last one month prior to presentation. There were no specific intestinal or other associated symptoms. Her past surgical and medical histories were not significant. She had also not been evaluated by any gynaecologist.
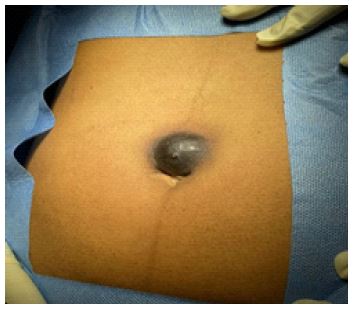
Examination showed a 3 cm by 4 cm nodular swelling around the upper edge of the umbilicus, darkish in colour, tender, irreducible, and not pulsating. The umbilicus was inverted. Abdominal ultrasound scan confirmed a swelling abutting on the umbilicus. The patient had excision biopsy of the nodule and a simple umbilical defect repair. Histopathological examination revealed the presence of endometrial glands and stroma predominantly within the dermis. Some of the glands were dilated and filled with red blood cells. Also seen were haemosiderin-laden macrophages, infiltrates of lymphoplasmatic inflammatory cells and intervening dense fibrotic stroma; the overlying epidermis was hyperplastic and there was no evidence of malignancy; all features are in keeping with endometriosis. She was referred to the gynaecologists for further evaluation following the histology report and the findings were unremarkable. The patient has remained free of symptoms for the past 6 months.

Discussion
Umbilical endometriosis is a rare presentation accounting for 0.5-1% of all extra-pelvic endometriosis [10]. Primary Umbilical Endometriosis (PUE) coexisting with an umbilical hernia, as seen in our patient, is also a rare entity and poses a diagnostic challenge to the Surgeon, as it may mimic an obstructed or a strangulated hernia, requiring a high index of suspicion to make a diagnosis [5,10-12]. It frequently develops in previous umbilical scars by implantation or following surgical manipulations, but very rarely presents as primary (spontaneous) umbilical endometriosis as seen in the case reported. Only a limited number of cases of PUE have been reported in the literature [3,13-15]. The umbilicus is a physiological scar with a predilection to endometriosis [10]. Haematogenous and lymphatic spread to the umbilicus and direct migration of endometrial cells through the round ligament or the remnants of the obliterated umbilical vessels may explain the occurrence of PUE [8]. Umbilical endometrioma (nodule) as seen in our case was first described by Villar in 1886, the so-called “Villar’s nodule” and is the typical presentation in umbilical endometriosis [7,9,12]. Most cases of PUE will present with cyclical symptoms related to menstruation. The accompanying pain may however be confused with the pain of a recurrent obstructed or strangulated hernia in a patient previously diagnosed with a hernia, especially where there is no visible bleeding or discharge from the umbilicus, and the patient had not had any abdominal surgery or prior gynaecological evaluation. This was the diagnostic difficulty we encountered in the case reported. Recognised differential diagnoses of umbilical endometriosis include an umbilical cyst, abscess, melanoma, lipoma, suture granuloma or a deposit of systemic malignancy [13]. Victory et al. [12] reported that 90% of cases of umbilical endometriosis will present with umbilical swelling, less than 50% will present with bleeding, and 80% with cyclical pain resulting from tissue inflammation, distension and cyclical changes, while up to 25% occur with pelvic endometriosis. There is usually discolouration of the nodule due to bleeding into the lesion with deposition of haemosiderin which can be demonstrated on histopathological examination as seen in our patient and shown in Figure 1.
In a case review series of five African patients, Makena et al. [11] reported an age range of 31-47 months, while duration of symptoms ranged between 3 months and 60 months. All the patients presented with umbilical swelling and pain with lesions ranging from 1.6 cm to 4 cm in diameter. Their findings were consistent with those of our patient who was 34 years of age and presented with a painful umbilical swelling of 48 months duration and measuring 3 cm by 4 cm. A similar review by Bindra et al. [14] and Adewole et al. [15] showed similar findings.
Although laparoscopy is the traditional method of diagnosis based on the accurate visual identification of endometriotic lesions, this is only applicable to pelvic endometriosis. Diagnosis in our patient was mainly based on clinical suspicion. Ultrasound imaging was useful in the preoperative evaluation of the nodule and assessment for involvement of surrounding tissues and to exclude other pelvic pathology. The diagnosis was however confirmed by histopathological examination of the excised nodule. MRI has been recommended as the imaging technique of choice for diagnosis of endometriosis [5]. This imaging technique is not usually readily available in low-resource setting like ours and where available the cost may be a challenge. It was not used in our patient. Surgical excision of the umbilical lesion with a hernia repair is considered the preferred treatment option and this was offered to our patient (Figure 2). All the reported cases in the literature had surgical management [3,11,14]. The surgical option also helped in providing tissue for histological diagnosis since the diagnosis was only a differential preoperatively.
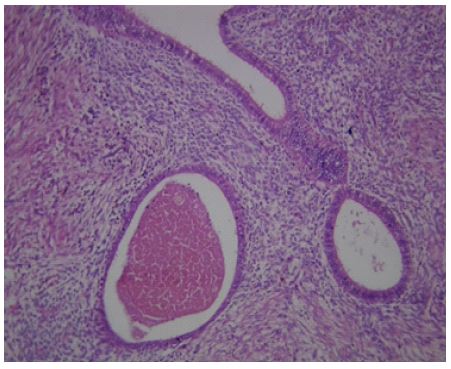
The histopathological appearance of an endometriosis section is usually characterized by irregular glandular lumina that are embedded in the stroma with an elevated vascular and cellular component similar to the stroma of the functional endometrium [6]. The histological findings of haemosiderin-laden macrophages, infiltrates of lymphoplasmatic inflammatory cells (Figure 3) and intervening dense fibrotic stroma with hyperplastic overlying epidermis in the case presented tend to point to lymphatic migration of endometrial cells as the probable aetiological factor. This further highlights the importance of always preserving surgical specimens for histopathological evaluation to aid in diagnosis, especially where preoperative diagnosis is a challenge.
Other treatment options include use of hormonal therapy like Gonadotropin-Releasing Hormone (GnRH) analogues or Danazol® which can be used preoperatively for relief of symptoms and to reduce the size of the lesion [1]. Their prolonged use is however associated with side effects. Our patient was referred to the Gynaecologists for further gynaecological evaluation for any associated pelvic endometriosis and follow-up.
Conclusion
PUE mimicking a strangulated umbilical hernia is a rare entity presenting a preoperative diagnostic challenge. A high index of suspicion and adequate clinical evaluation of a woman with a painful umbilical nodule, with specific enquiry on the cyclical nature of the pain and its association with her menstrual cycle, is key to the diagnosis of umbilical endometriosis in the presence of an umbilical hernia. Surgical excision with umbilical herniorrhaphy and histopathological examination of the surgical specimen are important management strategies.
Declarations
Conflict of interest: The authors declare no conflict of interest.
Financial support and sponsorship: Nil
Consent: The authors certify that a written consent was obtained from the patient to publish the clinical images and this case report.
Acknowledgement: We are grateful to the Departments of Surgery and Histopathology, Maitama District Hospital, Abuja, Nigeria, for allowing access to the records of the patient.
References
- Clark TJ. Benign conditions of the ovary and pelvis. In: Bickerstaff H and Kenny LC (editors): Gynaecology by Ten Teachers 20th Edition. CRC Taylor & Francis Group, Florida. 2019; 250-258.
- Yuen JS, Chow PK, Koong HN, Ho JM, Girija R. Unusual sites (thorax and umbilical hernial sac) of endometriosis. J R Coll Surg Edinb. 2001; 46(5): 313-5.
- Ismael H, Ragoza Y, Harden A, Cox S. Spontaneous endometriosis associated with an umbilical hernia: A case report and review of the literature. Int J Surg Case Rep. 2017; 30: 1-5.
- Simoglou C, Zarogoulidis P, Machairiotis N, Porpodis K, Simoglou L, et al. Abdominal wall endometrioma mimicking an incarcerated hernia: A case report. Int J Gen Med. 2012; 5: 569-71.
- Yu CY, Perez-Reyes M, Brown JJ, Borello JA. Magnetic Resonance Imaging appearance of umbilical endometriosis. J Comput Assist Tomogr. 1994; 18(2): 269-271.
- Bagade PV, Guirguis MM. Menstruating from the umbilicus as a rare case of primary umbilical endometriosis: a case report. J Med Case Rep. 2009; 3: 9326.
- Zollner U, Girschick G, Steck T. Umbilical endometriosis without previous pelvic surgery: A case report. Arch Gynecol Obstet. 2003; 267: 258-260.
- Ouédraogo NLM, Ilboudo S, Ouattara AK, Ouedraogo AS, Zida M, et al. A case report of Villar’s nodule in a woman without surgical history. Int J Surg Case Rep. 2018; 53: 186-188.
- Skidmore RA, Woosley JT, Katz VL. Decidualized umbilical endometriosis. Int J Gynaecol Obstet. 1996; 52: 269-273.
- Hansadah S, Begum J, Kumar P, Singh S, Balakrishnan D, et al. Umbilical Hernia as a Forerunner of Primary Umbilical Endometriosis: A Case Report. Medeni Med J. 2021; 36(4): 348-551.
- Makena D, Obura T, Mutiso S, Oindi F. Umbilical endometriosis: a case series. J Med Case Rep. 2020; 14(1): 14:42.
- Victory R, Diamond MP, John DA. Villar’s nodule: a case report and systematic literature review of endometriosis externa of the umbilicus. J Minim Invasive Gynecol. 2007; 14(1): 23-32.
- Odhar ZA, Muhi MR, Odhar HA. A Case of Primary Endometriosis Associated with an Umbilical Hernia. Cureus. 2022; 14(8): e27626.
- Bindra V, Sampurna S, Kade S, Mohanty GS, Madhavi N, et al. Primary umbilical endometriosis-case series and review of clinical presentation, diagnosis and management In J Surg Case Rep. 2022; 94: 107134.
- Adewole AA, Musa OA, Akintobi AO, Nzurumike CN, Mohammed UF, et al. Radical Excision (omphathalectomy) and laparoscopic management of associated pelvic endometriosis in a low-resource tertiary Hospital Afr J Reprod Health. 2021; 25(4): 167-173.