Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Large parietal abscess: A late complication of an anastomotic fistula
Soukayna Bourabaa*; Yahia Zain-Al-Abidine Khedid
Emergency General Surgery Department, Faculty of Medicine and Pharmacy, Mohamed V University, CHU Ibn Sina, Rabat, Morocco.
*Corresponding Author : Soukayna Bourabaa
Emergency General Surgery Department, Faculty of Medicine and Pharmacy, Mohamed V University, CHU Ibn Sina, Rabat, Morocco.
Email: soukayna.bourabaa@um5r.ac.ma
Received : Jul 07, 2024
Accepted : Jul 29, 2024
Published : Aug 05, 2024
Archived : www.jcimcr.org
Copyright : © Bourabaa S (2024).
Keywords: Anastomotic fistula; Drainage; Emergency; Parietal abscess.
Citation: Bourabaa S, Zain-Al-Abidine Khedid Y. Large parietal abscess: A late complication of an anastomotic fistula. J Clin Images Med Case Rep. 2024; 5(8): 3193.
Description
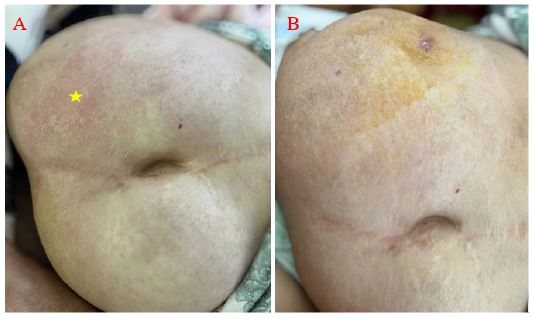
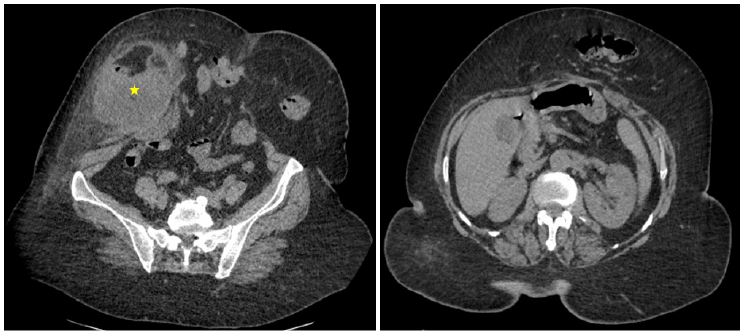
A 72-year-old patient with a history of poorly controlled hypertension and type 2 diabetes underwent surgery four months ago for a strangulated umbilical hernia complicated by a 50 mm perforation of the small intestine, requiring small bowel resection with digestive anastomosis. Postoperative course was complicated by anastomotic fistula development on postoperative day 8, which spontaneously resolved by day 17. She was readmitted to the emergency room with right iliac fossa pain persisting for 15 days, accompanied by fever and a vomiting episode. On examination, her BMI was 38 kg/m², and she was conscious with a Glasgow Coma Scale (GCS) of 15/15, normotensive at 14/9 mmHg, tachycardic at 100 beats per minute, and oxygen saturation was 94% in ambient air. Abdominal examination revealed a midline laparotomy scar with a non-complicated left paraumbilical hernia and a warm, tender swelling in the right iliac fossa and right flank (Figure 1). Laboratory findings showed signs of inflammation with a leukocytosis of 17,470 cells/mm³ and elevated CRP at 282 mg/l. Abdominal CT scan revealed a significant midline hernia with a 120 mm defect, accompanied by a large mass adjacent to the hernia measuring 108 x 90 mm, appearing to involve digestive structures (Figure 2). The initial management aimed to control the infection, so emergency radiological drainage was performed. Initially, it yielded 700 cc of purulent fluid, which gradually decreased to 0 cc over the course of a week. Cytobacteriological examination of the drainage fluid identified penicillin-resistant Escherichia coli, leading to adjustment of antibiotic therapy based on the antibiogram. The patient was discharged on day 8 post-drainage with good clinical and laboratory progress. She was followed up in outpatient clinic after 15 days in a satisfactory general condition.