
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 5
US detection of CB layer within a TB
J Halevy-Politch1*; A Craft2
1Technion I.I.T., Haifa 32000, Israel.
2Mi-Rei Associates, Haifa, Israel.
*Corresponding Author : J Halevy-Politch
Technion I.I.T., Haifa 32000, Israel.
Tell: +972-4-834-2473;
Email: yapo@actcom.co.il
Received : Jul 10, 2024
Accepted : Aug 02, 2024
Published : Aug 09, 2024
Archived : www.jcimcr.org
Copyright : © Halevy-Politch J (2024).
Abstract
Background: A thin layer of Cortical Bone (CB) is located in a Trabecular Bone (TB), such as the wrapping around the Mandibular Canal (MC), located in the lower jaw. During an implantation surgery, this thin layer of CB, and the MC can be damaged - what should be prevented also by intraoperative monitoring.
Methods: Ultrasound (US) was applied in this study, enabling to obtain in Real-Time (RT) the distance/depth of the Front-Surface (FS) of a thin CB sample. This depth was measured from the entrance of the US to TB up to the FS of the thin CB.
Results: Small samples of thin CB were inserted at several depths of TB. The depths of the CB samples were measured by the developed US system and it was compared to a mechanical measurement. For most cases, an agreement within less than 2%, was obtained between these measurements.
Conclusion: It was demonstrated that the new US device provides depth information of thin CB sample located in a TB. These US measurements were performed with an accuracy that can prevent a damage to the thin CB during a surgery, or during other invasive treatments.
Keywords: Cortical Bone (CB); Detection; Implant; Trabeculae; Ultrasound (US).
Citation: Halevy-Politch J, Craft A. US detection of CB layer within a TB. J Clin Images Med Case Rep. 2024; 5(8): 3200.
Introduction
This investigation is looking for a detection method of a thin layer of dense material inside a softer one. By providing to such a detection system, also a Real-Time (RT) ability - an Intraoperative (IO) measuring solution is gained. Such cases, of layers with different densities, exist generally in nature; Here we will concentrate in the human body.
The deposition of the matrix has a lamellar pattern that provides the dense microstructure to the Cortical Bone (CB). The cancellous (Trabecular) Bone (TB) microstructure, due to its high fluid content (90%), behaves bio-mechanically as a solid open porous material [1]. The relationship between bone density and its modulus of elasticity is not linear [2], because it depends on the integrity of the trabecular mesh and on the chemical properties of the matrix that can be altered by age and systemic illness.
The mandible (as an example of an organ in the human body), consists of an outer layer of Cortical Bone (CT) (approximate thickness of ~1 mm). The alveolar process is occupied by the roots of the teeth with none or only a very small amount of trabecular bone in tooth bearing areas, while the central part of the mandibular body consists of Trabecular Bone (TB). The bone mass and bone activity in the TB vary with their function [3]. As the function is different in the three regions of the mandible, incisor, premolar and molar, and depending on the state of dentition, a variation in bone structure in the TB within a single mandible would be expected [4,5].
Detection of a thin CB located inside a volume of TB is the case that a surgeon is fronted during an implantation surgery, especially in the lower jaw. Here, there is located, from the anatomic point of view, the Mandibular Canal (MC), surrounded by a thin protecting layer of CB [6-8].
Meticulous treatment planning and increasingly sophisticated diagnostic tools, such as: Conventional X-ray, CT, MRI and various navigational software, are today, the gold standard in implantology [9].
The canal that opens at the mental foramen (mandibular canal), houses the inferior alveolar nerve and blood vessels; it begins at the posterior end of the body of the mandible and runs through the length of it, almost parallel to the lower border [10]. A knowledge of the position of the inferior dental (mandibular) canal in vertical as well as in buccolingual dimensions is of paramount importance during site preparation for implants, where Ultrasonic (US) measuring method was proposed and implemented during appropriate surgical studies [11-13], and similarly in brain and spinal cord, including vertebrae surgeries [14-16].
Material and methods
General
The attention is given here to the Ultrasound (US) reflections, by applying a single US transducer that Transmits (Tr) these signals and Receives (Rc) their echoes. The US propagates through the TB and while impinging the front surface of the CB (denser material), reflections are obtained. These are finally received by the US transducer followed by further amplification, filtering, data processing and finally displayed. The method for estimating the velocity (Speed of Sound = SOS) in TB [17], from transmission, attenuation and reflection processes in TB and pulse-echo measurements, was applied here. The monitoring system measures the time between the transmitted and received signals. For a more accurate measurement, the received US signals were coherently processed [18-21]. Thus, from an apriori knowledge of the SOS in the TB and in the saline solution, the depth of the CB layer was assessed.
The electronic parameters during the experimental measurements
Pulse Repetition Frequency (PRF) = 500 Hz;
The US frequency fUS = 5 MHz
The average was performed on 500 recorded signals.
The US parameters during the experimental measurements
Type of the US transducer: Panametrics, C310, f=5MHz
Transmission US modes: 1, 2 and 6 pulses per burst.
The mechanical parameters during the experimental measurements
Drilled depths in TB: 0, 2, 4 and 6 (mm).
CB within TB was fixed during the above drills.
The depth of CB was chosen to be different at every set of experiments.
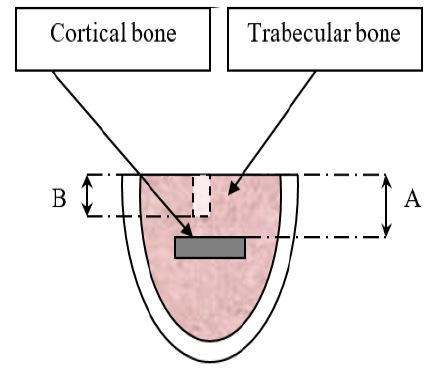
Experiments were performed on several TB samples that were from a porcine Hip. A thin and small plate of CB was inserted in the TB at a depth ‘A’ from its upper surface. A bore of 2 mm (in diameter) was drilled in the TB. This was performed in several samples and in each one of them - at a different depth. Using this method, the upper surface of the CB sample was detected (as its attenuation is high, causing to a secondary reflection to be low) - as described schematically in Figure 1.
Note: All samples of CT and TB were obtained from a slaughter house.
The experimental sample
Figure 1: Describes the geometry of the measured sample that consists of B, with a thin and small plate of CB inserted in it.
Experiments and results
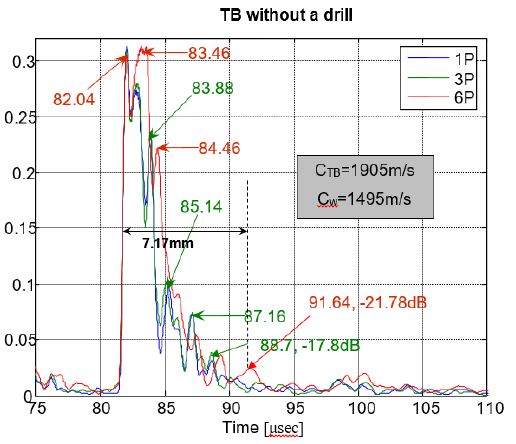
US detection of a thin CB in TB, without a drilled bore in TB
The presented reflections were obtained after coherent processing [18-21] of the detected signals.
The ordinate describes the attenuation [dB] relative to the first peak;
The abscissa describes the time [μsec].
The numbers in colors, describe the peak values, as obtained with time, for each transmission type (i.e., no. of pulses/burst).
Conclusion
Comparison of US to mechanical depth measurements
The depth of the CB (as described in Figure 1), was obtained from US reflections width, as 7.17 mm (as shown in Figure 3); When it was measured mechanically, the CB depth was found to be 7.21 mm. The difference between these measurements is 0.55%, thus enabling US depth measurements of this kind with good reliability.
The attenuation is relative to the first peak, which is in this case -21.78 dB, as shown in the graph of Figure 3, and it provides about 30 dB/cm. As the measurements were performed at 5 MHz, the attenuation can be expressed also, as 6 dB/MHz.
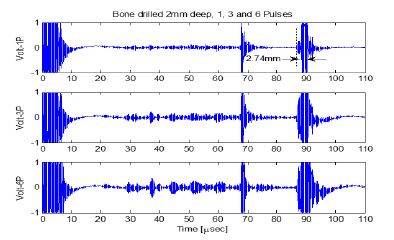
Drilled bore in TB, in depth of 2 mm
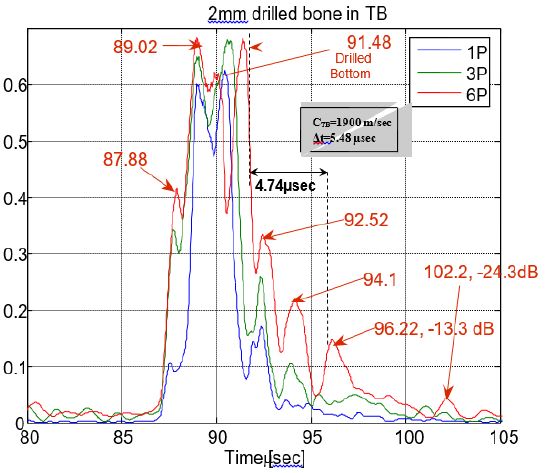
The ordinate describes the attenuation (decrease) in dB, relative to the first peak.
The abscissa presents the time [10-6 sec = μsec].
The red numbers describe the time (μsec) and the attenuation (dB) at a certain point.
Drilled bore - comparison measurements: The reflected signal, from the bottom of the drilled bore in TB, was obtained after 1.3 μsec, for a US velocity in saline solution as Cw = 1,495 m/sec. Thus, it provides a distance of 1.944 mm. The difference between mechanically and US measurement of this distance is 2.8%.
The Time of Flight (TOF) from the bottom of the drilled bore in TB to the upper surface of the CB sample (see Figure 1), was 5.48 μsec; For a measured velocity in TB of CTB = 1,900 m/sec, it provides a distance of 5.2 mm.
Accordingly, the total distance, from the entrance of the US signal into the drilled bore, to the upper surface of the CB, is 7.194 mm (US measurement). Mechanically, this distance was found as 7.21 mm. This provides a difference of 0.016 mm, or 0.22%.
Experiment where the TB bore was of 4 mm
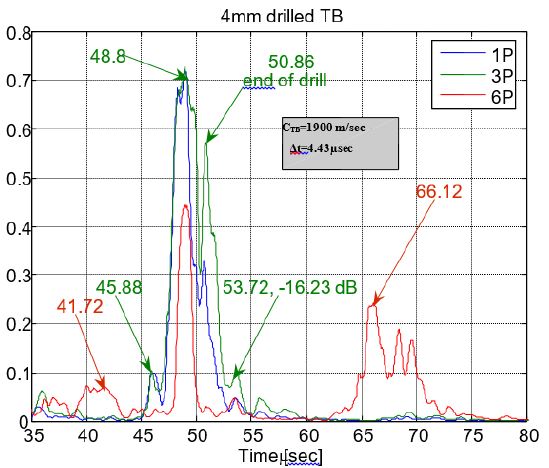
Total distance/depth, comparison of US with mechanical measurement: By taking the distance from the bottom of the drilled bore in TB to the upper surface of the CB as
dTB = 0.5·Δt·CTB = 0.5·4.43·10-6·1.9· 103 = 4.2 mm.
By adding the distance in the drilled bore (filled with a saline solution)
dw = 2.1·10-6·1.495·103 = 3.13 mm.
Thus, the total depth is
dtotal = 4.2+3.13 = 7.33 mm.
Therefore, the difference related to the mechanical measurement is 0.12 mm, or in percentage 1.7%.
The ordinate describes the attenuation (decrease) [dB], relative to the first peak.
The abscissa is the time [μsec].
Red and Green numbers describe the time [μsec], while the Green describes also the relative attenuation (relative to the peak) at the measured point [dB].
Summary
In this work, we were interested to evaluate the reliability of US depth measurement of a thin CB sample that was inserted in the TB. Mechanical measurements were also applied, for comparison purposes.
The ‘experimental sample’ was designed and built in a way that will simulate the Mandibular Canal (MC) that is wrapped by a thin layer of a CB. There were prepared several ‘experimental samples’, where the CB was placed in different depths of the TB.
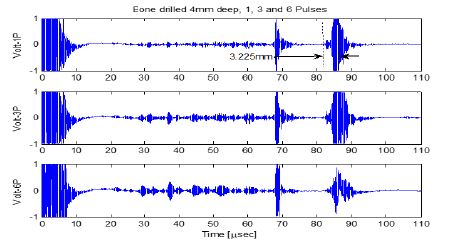
US measurements of the reflected signal were performed, where in all these experiments, the transmitted US frequency was 5 MHz, using a pulsed mode of 1, 3 and 6 pulses per burst.
The received signals by the US transducer, were fed through a calibrated pre-amplifier, to a coherent signal processing circircuitry. From there it was fed to the input of the oscilloscope - and on its screen the time-response curves were obtained. On the mentioned screen, were also performed the attenuation and time difference measurements.
The mechanical measurements were obtained by means of a caliper (with a resolution of 10-2 mm) and by a calibrated drill (with graduations of 10-1 mm).
The US and the mechanical measurement were repeated 10 times at every condition, from where their mean value with the Standard Deviation (STD) were assessed.
Table 1: The reflected pulse widths (μsec) for 1, 3 and 6 pulses/burst, as a function of the drilled depth in TB (related to Figures 3, 5 and 7).
Table 1: Summarizes the reflected pulse-widths (μsec), relating to Figures 3, 5 and 7.
| Depth of drilled bore in TB (mm) | Reflected pulse width, for 1 pulse/burst (μsec) | Reflected pulse width, for 3 pulses/burst (μsec) | Reflected pulse width, for 6 pulses/burst (μsec) |
|---|---|---|---|
| 0 | 3.1 | 5.2 | 6.6 |
| 2 | 4.1 | 5.5 | 7.2 |
| 4 | 2.5 | 3.92 | 7.08 |
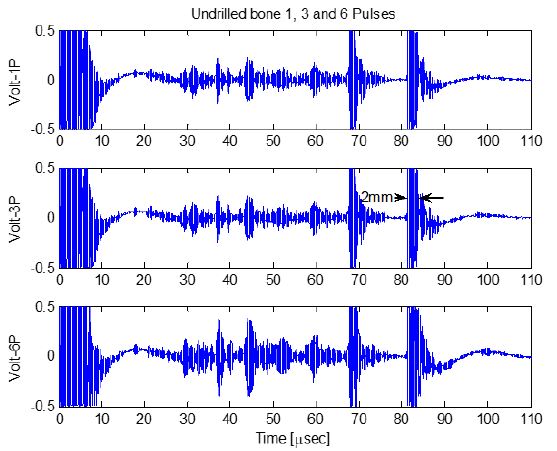
Without a drilled bore, the width of the main reflected pulse is similar to the transmitted one.
With 2 mm drilled bore, the widths and amplitudes of the reflected signals are similar; although the reflected pulse is wider as the no. of pulses/burst increases.
With 4 mm drilled bore: for 1 pulse/burst the reflection is in the center of the main reflected signal. It is wider for 3 pulses/burst and much more wider (with side-lobes) for 6pulses/burst.
Conclusion
By comparing the depth of the CB sample within the TB, by the US measurement versus the mechanical one, it was found that without a drilled bore in TB: they differ by 0.55%.
By comparing the depth of the drilled bore, between US and mechanical measurements, the difference was 2.8%. This difference was due to the accuracy of mechanical engraving on the drill, which was not better than 0.1 mm.
The total distance/depth, from the entrance to the drilled bore to the upper surface of the CB was 0.22% - for a drilled bore in TB of 2 mm.
The total distance/depth, by comparing US with mechanical measurements (for drilled bore of 4 mm) was 1.7%.
In conclusion, the differences between the obtained results with the US and the mechanical methods, was smaller than 3%.
According to the above conclusion, the US measuring method was applied during clinical experiments in real-time and intra-operatively - thus enabling to obtain better, faster and reliable surgical results [11-16]; Moreover, the patients were safer and also don’t accumulate the x-ray radiation.
As for US measuring system, using a single pulse/burst, it provides a satisfying accuracy during the interpretation process; However, if higher energy is required, there exist the possibility to transmit 3 or more pulses per burst, but more attention is required during the interpretation process of the obtained signals, due to the difference in the temporal-coherence signal processing [19-22].
References
- Morgan EF, et al. Trabecular bone modulus-density relationships depend on anatomic site. J Bionechanics. 2003; 36: 897-904.
- B Zdravkov, J Čermák, M Šefara, Jf Janků. Pore classification in the characterization of porous materials: A perspective Central European Journal of Chemistry. 2007. https://doi.org/10.2478/s11532-007-0017-9.
- Carl E Misch, Roberts WE, Bone physiology and metabolism. J. Calif Dent Assoc. 1987; 15: 54-61.
- Curry JD. The mechanical adaptations of bones, Princeton U. Press. 1984.
- Nordin BEC, Metabolic bone and stone disease. Churchill Livingstone Publ. 1973; 1: 309. English, ISBN-10. 0443009430.
- Nina von Worwern. Variations in structure within the trabecular bone of the Mandible. Scand. J. Dent. Res. 1977; 85: 613-622.
- Starkie C, Stewart D. The intra-mandibular course of the inferior alveolar nerve. J. Anat. 1931; 65: 319-323.
- Lang J. Clinical Anatomy of the Masticatory Apparatus and Peripharyngeal Space. New York; Thieme Medical Publ. Inc. 1996; 19-40.
- Albrektsson T, Zarb G, Worthington P, et al. The long-term efficacy of currently used dental implants. Int. J. Oral Maxillofacial Implants 1986; 1: 1-25.
- J Halevy-Politch, I Rusnak. Implant-screw loosening: Review of the Existing methods their applications (Review Article). J. Clinical Images and Med. Case Rep. ISSN2766 Open Access. 2024; 5(23): 880. DOI: www.doi.org/10.52768/2766-7820/2822.
- Harry Sicher E. Lloyd Du Brul, Oral Anatomy. 2023; 1: 50-53.
- N Rosenberg, A Craft, J Halevy-Politch. Intraosseous monitoring and guiding by ultrasound: A feasibility study. Ultrasonics. 2014; 54: 710-714.
- E E Machtei, H Zigdon, L Levin, M Peled. Novel Ultrasonic Device to Measure the Distance from the Bottom of the Osteotome to Various Anatomic Landmarks, J. Periodontol. 2010; 1044-1051. Doi:10.1902/jp.201009021.
- H Zigdon-Giladi, M Saminsky, R Elimalech, E E Machtei. Intraoperative measurement of the distance from the bottom of the osteotomy to the mandibular canal using a novel ultrasonic device. and guiding by ultrasound: A feasibility study, Clinical Implant Dentistry and Related Res. 2015; 18(5): 1034-1041. https://doi.org/10.1111/cid.12362.
- Halevy-Politch J, Zaaroor M, Sinai A, Constantinescu M. New US Device versus imaging US to assess tumor-in-brain. Chinese Neurosurgical Journal, Research Article, Open Access. 2020; 1 - 13. https://doi.org/10.1186/s41016-020-0205-1.
- Zaaroor M, Sviri G, Constantinescu M, Halevy-Politch J. Intraoperative spinal cord remote monitoring with a modified US A-scope. J. Clinical Case Report, (Ref. 123;8(7):1219). ISSN: 2381-912X. 2021.
- N Rosenberg, J Halevy-Politch. Intraosseous monitoring of drilling in lumbar vertebrae by ultrasound: an experimental feasibility study. PLOS ONE. 2017. https://doi.org/10.1371/journal.pone.0174545.
- I Rusnak, N Rosenberg, J Halevy-Politch. Trabecular bone attenuation and velocity assess by ultrasound pulse-echoes. Applied Acoustics. 2020; 157: 107007. https://dou.org/10.1016/j.apacoust.2019.107007.
- KD Donohue, JM Bressler, T Varghese, NM Bilgutay. Spectral correlation in ultrasonic pulse echo signal processing IEEE Trans. on Ultrasonics, Ferroelectrics, and Freq. Control. 1993; 40(4): 330-337. DOI: 10.1109/58.251281.
- A Gardner. A unifying view of coherence in signal processing. Signal Processing. Get rights and content. 1992; 29(2): 113-140. https://doi.org/10.1016/0165-1684(92)90015-O
- WA Gardner. Signal interception: A unifying theoretical framework for feature detection. IEEE Trans. Comm. 1988.
- JA Cadzow, et al. Linear modeling and the coherence function. IEEE Trans. Acoust. Speech Signal Process. 1987.