
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Hand in glove appearance
*Corresponding Author : Srikant Malegaonkar
Department of Pulmonary Medicine, Institute of Medical Education and Research (PGIMER), Chandigarh, India.
Email: kmsrikant@gmail.com
Received : Jul 15, 2024
Accepted : Aug 05, 2024
Published : Aug 12, 2024
Archived : www.jcimcr.org
Copyright : © Malegaonkar S (2024).
Citation: Malegaonkar S. Hand in glove appearance. J Clin Images Med Case Rep. 2024; 5(8): 3203.
Description
40-year-old man presented to our pulmonology clinic with complaints of persistent cough with expectoration and breathlessness since past 2 months. Elucidation of medical history revealed patient to be an asthmatic with use of inhaled bronchodilators through Metered Dose Inhaler (MDI) on an as and when required basis. However, in past 2 months despite use of regular MDI there was no relief of symptoms. Apart from polyphonic wheeze on auscultation rest of general and systemic examination was unremarkable.
Our patient underwent evaluation on the lines of difficult to treat asthma, Chest roentgenogram done as part of the same revealed inhomogeneous opacities involving bilateral mid lung zones and ring shadows in left lower lung zone (Figure 1a). Axial cuts of Computed Tomography of chest (CT) done for better evaluation of chest roentgenogram changes showed mucus plugs occluding dilated bronchi. These mucus plugs gave characteristic hand in glove appearance on Chest roentgenogram and CT Chest (Figure 1b). The mucus characteristically had high attenuation when evaluated in soft tissue window termed High Attenuation Mucus (HAM) (Figure 1c). In view of above findings patient underwent Allergic Bronchopulmonary Aspergillosis (ABPA) workup which was positive. Patient received systemic corticosteroids along with inhaled bronchodilator resulting in significant improvement in his symptoms and radiology.
Allergic Bronchopulmonary Aspergillosis (ABPA) is a hypersensitivity reaction in response to colonization of airway with Aspergillus fumigatus occurring exclusively in patients with asthma or cystic fibrosis. Prevalence of ABPA among difficult to treat asthmatics is estimated to be about 1 to 2 percent [1]. Diagnosis of ABPA is made based on criteria given by International Society for Human and Animal Mycology (ISHAM) which includes presence of an predisposing condition along with demonstration of immune reaction to Aspergillus fumigatus fungi, eosinophilia and characteristic chest radiology.
Finger in glove appearance or opacities representing mucoid impaction in dilated bronchi with occlusion of the distal end and High - Attenuation Mucus (HAM) that is mucus having high attenuation values, appearing visually denser than paraspinal skeletal muscle are characteristic and pathognomonic of ABPA [2].
Primary therapy for ABPA includes use systemic corticosteroids to decrease inflammatory activity and thereby preventing irreversible lung damage. Antifungal agents like itraconazole are used in steroid dependent
ABPA is an important entity to be kept in mind while investigating difficult to treat asthmatic patients. Early recognition and treatment can spare patient from bronchiectasis or pulmonary fibrosis occurring in later stages of disease.
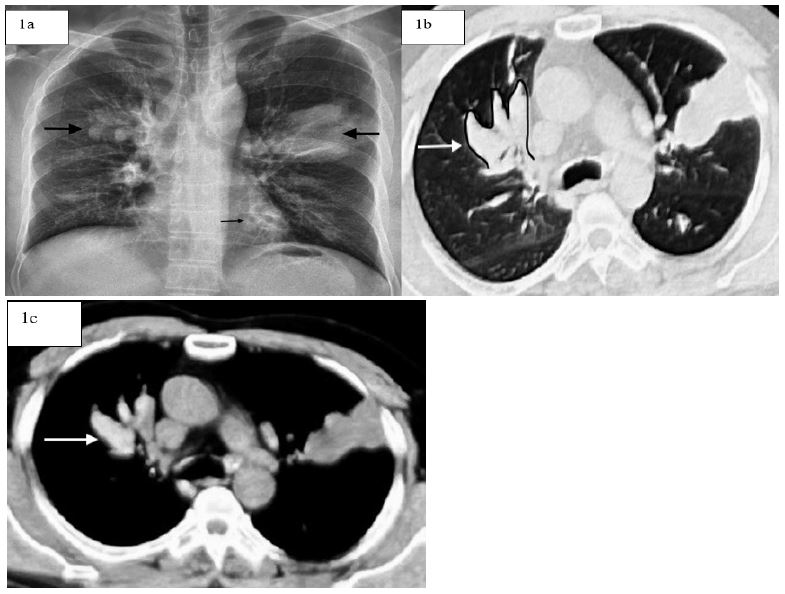
(b) CT Chest showing dilated airways with mucus plugging (white arrow) Hand in glove appearance.
(c) Non contrast CT Chest showing high attenuation mucus.
References
- Greenberger PA. Allergic bronchopulmonary aspergillosis. J Allergy Clin Immunol. 2002; 110(5): 685-92.
- Agarwal R, Khan A, Garg M, Aggarwal AN, Gupta D. Pictorial essay: Allergic bronchopulmonary aspergillosis. Indian J Radiol Imaging. 2011; 21(04): 242-52.
- Agarwal R, Sehgal IS, Dhooria S, Aggarwal AN. Developments in the diagnosis and treatment of allergic bronchopulmonary aspergillosis. Expert Rev Respir Med. 2016; 10(12): 1317-34.