
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Pilocytic astrocytoma underlying failure to thrive
Ligia Modelli Rodrigues; Larissa Lyra; Cláudia B De Almeida; Tulio Konstantyner*
Department of Pediatric Nutrition, Federal University of Sao Paulo, Brazil.
*Corresponding Author : Tulio Konstantyner
Department of Pediatric Nutrition, Federal University of Sao Paulo, Brazil.
Email: tkmed@uol.com.br
Received : Jul 17, 2024
Accepted : Aug 06, 2024
Published : Aug 13, 2024
Archived : www.jcimcr.org
Copyright : © Konstantyner T (2024).
Abstract
Objective: This case report describes a poor weight gain secondary to organic causes in a young infant.
Case description: Girl, 8 months old, referred for investigation of difficulty gaining weight. Environmental causes were ruled out and the complementary tests carried out were within normal limits. Despite several attempts to provide adequate caloric-protein supply, there was no success in nutritional recovery. At 15 months of age, she began to present with myoclonus and daily vomiting. The investigation was expanded with an MRI that revealed a grade I benign polycytic astrocytoma. After resection, the patient began the weight-height recovery process.
Comments: In most cases, retardation in physical growth occurs due to environmental causes such as food deprivation, lack of stimulation or low understanding from caregivers. However, Every healthcare professional must pay attention to organic causes. The multidisciplinary approach contributes to the early identification of unusual and potentially treatable causes.
Keywords: Diencephalic syndrome; Failure to thrive; Hypothalamic neoplasms; Intracranial tumor; Pilocytic Astrocytoma; Russell’s syndrome.
Citation: Rodrigues LM, Lyra L, De Almeida CB, Konstantyner T. Pilocytic astrocytoma underlying failure to thrive. J Clin Images Med Case Rep. 2024; 5(8): 3205
Introduction
Failure to thrive is an important warning sign during pediatric follow-up. No consensus on the definition of failure to thrive exists; however, it is often defined as a weight-for-age value that falls below the 5th percentile on multiple measurements or a weight deceleration that crosses two major percentile lines on a growth chart [1,2]. Clinicians, especially pediatricians, should be aware of Diencephalic Syndrome (DS, otherwise known as Russell’s syndrome) as an unconventional and rare cause of failure to thrive during early childhood [2,3]. DS is directly related to neoplasms of the central nervous system especially in the hypothalamus and optic chiasm regions [1]. However, the features of DS can be variable, often resulting in delayed diagnosis, which may worsen prognosis.
Investigating the causes of poor weight gain is challenging. Complex non-specific clinical presentation often leads to misdiagnosis. The lack of awareness for this syndrome among pediatricians also contributes to diagnostic delay. A meticulous approach can lead to early diagnosis and intervention. The purpose of this report is to describe secondary poor weight gain due to an organic cause in young infants.
Case presentation
An 8-month-old girl was admitted to our university hospital for further assessment of poor weight gain. The infant was the second child of a non-consanguineous couple. No history of complications in the gestational, perinatal, or neonatal periods was observed. The patient was born at 38 weeks of gestation, with no complications. The birth weight was 3,090 kilograms (10th to 50th percentile), birth length was 48 cm (15th to 50th percentile), and head circumference was 34 cm (50th percentile). No changes in neonatal screening tests were observed. The patient’s family history was uneventful, and no genetic disorders were reported.
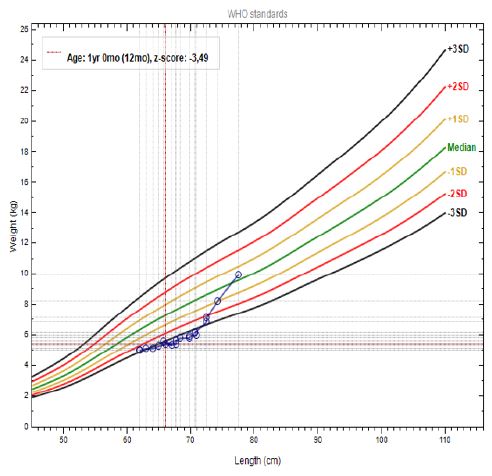
During evaluation, no delay in neuropsychomotor development was identified; prior to our evaluation, the patient had been evaluated by a speech therapist who ruled out any signs of dysphagia. No changes in the physical examination, in addition to the patient’s thinness (evinced by the weight-for-height curve with a score between -2 and -3), were found.
From the first month of age, the child’s weight gain slowed despite increased caloric intake. The patient remained exclusively breastfed until 2 months of age, but supplementation with infant formula was indicated from that age onwards due to low weight gain. At 5 months old, complementary feeding was started, but low acceptance was a constant maternal complaint.
In the 7th month, the patient underwent evaluation by a pediatric gastroenterologist, who raised the hypothesis of allergy to cow’s milk protein due to low weight gain and indicated the use of an amino acid-based formula. No significant effect on weight gain was observed after this dietary change.
During our follow-up, we estimated the patient’s total energy needs using the Dietary Reference Intakes (DRIs) and added an additional 100% to the daily needs for nutritional recovery [4]. Despite several attempts at adequate calorie-protein supply with dietary adjustments, the patient maintained a poor weight and height. Environmental causes such as food deprivation and lack of stimulus were ruled out, since the family (from the upper middle social class) had a good understanding of and adherence to nutritional recommendations.
Laboratory investigations (including electrolyte levels, complete blood count, renal function panel, liver parameters, and hormonal assays) were normal. Array, transfontanellar ultrasound, echocardiogram, and total abdominal ultrasound were performed, and the results were within normal ranges. To rule out mitochondrial disease, an examination was conducted for organic acids in the urine, where the abnormal result of these organic acids was attributed to the use of infant formula with a high content of medium-chain triglycerides.
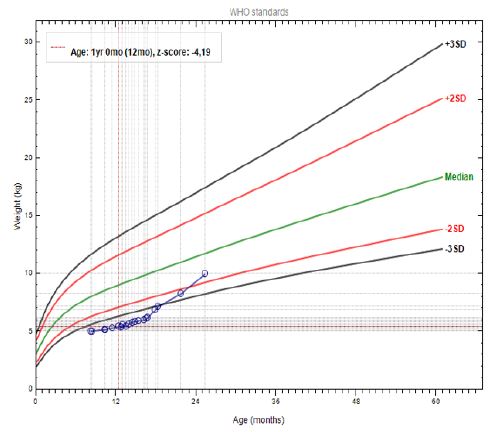
At 12 months old, we chose to offer a diet via enteral nasogastric tube to ensure the estimated calorie-protein supply without external interference; however, no success in weight gain was achieved, and the patient’s weight remained below the z score -3.
At approximately 15 months of age, the parents noticed the onset of constant hiccups. In addition, the child began to present with myoclonus in the upper and lower limbs, without a loss of consciousness, that was not associated with infectious symptoms. Her symptoms also evolved to include daily vomiting - a trait that was often not associated with diet. These complaints led to hospitalization and the investigation was expanded with a Magnetic Resonance Imaging (MRI) that revealed a grade I benign pilocytic astrocytoma in the brainstem region (Figure 1).
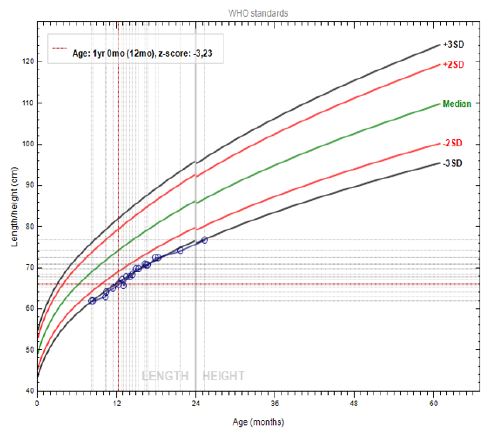
The patient underwent surgical resection of the tumor. After the tumor removal procedure, the child began the nutritional recovery process (Figures 2-4).

Discussion
DS was first described by Russell in 1951, based on a series of five children with hypothalamic neoplasms [2]. DS is characterized by progressive emaciation (despite normal or increased calorie intake), with normal linear growth and normal intellectual development, in association with central nervous system tumors [2,8]. Other symptoms of DS include locomotor hyperactivity, hyperalertness, hyperkinesia, euphoria, hiccups, vomiting, and nystagmus [2,5]. In a most recent review, onset of symptoms was 30.6 months [2]. DS is usually associated with a massive lesion in the diencephalon; however, similar symptoms have also been reported in posterior fossa brain tumors [5]. Most case reports do not report any delay in neuropsychomotor development.
The mechanisms underlying failure to thrive in DS have not been fully explained. Central factors modify fat distribution without altering growth velocity. Several case reports have confirmed an elevation in Growth Hormone (GH) that is secondary to the release of GH-releasing factors from the hypothalamus, promoting the mobilization of free fatty acids [6]. Some authors believe that β-lipotropin, a lipolytic peptide, is produced in excess by the tumor and could explain the decrease in subcutaneous tissue [1]. Brauner et al. reported reduction in leptin and insulin levels, with concomitant increase in ghrelin and human growth-hormone activity [7].
Although the pathophysiology of DS has not yet been clarified, this specific form of growth failure in the presence of elevated GH levels suggests a model of partial acquired resistance to GH [5]. Insulin-like growth factor 1 (IgF-1) concentration is usually normal [2].
Delays in diagnosis are common because of the rarity and non-specific symptoms of DS [3]. A case series of 11 patients with DS showed a mean age at diagnosis of 18 months. In other studies, it was found that the average age at diagnosis was 45.9 months and 12 months, both just with three patients [2,8].
In the case series of Brauner et al, the diagnosis was delayed about 12 months on average [7].
Our patient presented with a delay in linear growth velocity, as opposed to the expected clinical outcome in DS cases [2]. In the literature, we found one report of a 4-year-old girl with disseminated pilocytic astrocytoma in the diencephalon and brainstem, with a height less than that in the 3rd percentile. This knowledge raises the hypothesis that tumor location interferes with linear growth velocity [5].
The treatment of DS mainly addresses the primary disease. Generally, the treatment approaches surgical resection. Complete surgical resection is often impossible because of the central location of the tumor. Radiation therapy is often delayed because of radiation-induced damage to the developing brain. Conventional therapy for these patients consists of chemotherapy, usually with agents such as carboplatin and/or vinca alkaloids [9].
In a 1997 study of 43 children with low-grade gliomas, the three children who had dissemination in liquor were the only ones who developed the clinical features of DS. This suggests an association between DS and the early spread of gliomas. Astrocytomas associated with DS tend to be larger, more aggressive, and occur at younger ages [1].
Children with DS need nutritional support. The dietary intake should be always monitored during the treatment and the subsequent follow-up. The calculation of energy supply must often exceed 100% of the nutrient requirement to ensure adequate weight gain. Parenteral nutrition or enteral feeding with nasogastric tube may provide children unable to feed the nutrients necessary to ensure proper growth, to correct or prevent malnutrition [2]. The reintroduction of oral feeding should always be encouraged, seeking high-calorie-density diets.
Conclusion
Diencephalic syndrome is a rare cause of failure to thrive. Central nervous system tumors should be considered as an organic cause in any child presenting with poor weight gain despite adequate caloric intake. Early diagnosis and intervention may achieve better prognosis.
References
- Brauner R, Trivin C, Zerah M, Souberbielle JC, Doz F, et al. Diencephalic syndrome due to hypothalamic tumor: A model of the relationship between weight and puberty onset. Journal of Clinical Endocrinology and Metabolism. 2006; 91: 2467-2473.
- Conway M, Ejaz R, Kouzmitcheva E, Savlov D, Rutka JT, et al. Child Neurology: Diencephalic syndrome-like presentation of a cervicomedullary brainstem tumor. Neurology. 2016; 87(21): e248-e251.
- Densupsoontorn N, Jirapinyo P, Likasitwattanakul S, Sanmaneechai O, Sanpakit K, et al. Diencephalic syndrome due to astrocytoma in three infants with failure to thrive. Pediatrics International. 2011; 53(5): 784-787.
- Fleischman A, Brue C, Poussaint TY, Kieran M, Pomeroy SL, et al. Diencephalic syndrome: A cause of failure to thrive and a model of partial growth hormone resistance. Pediatrics. 2005; 115(6): 2004-2237.
- Kim A, Moon JS, Yang HR, Chang JY, Ko JS, et al. Diencephalic syndrome: A frequently neglected cause of failure to thrive in infants. Korean Journal of Pediatrics. 2015; 58(1): 28-32.
- Otten J, Hellwig JP, Meyers LD. Dietary References Intakes. The Essential Guide to Nutrient Requirements. Institute of Medicine of the National Academies. 1ª ed. National Academy of Sciences. 2006.
- Tosur M, Tomsa A, Paul DL. Diencephalic syndrome: A rare cause of failure to thrive. BMJ Case Reports. 2017; bcr-2017-220171.
- Trapani S, Bortone B, Bianconi M, Rubino C, Sardi I, et al. Diencephalic syndrome in childhood, a challenging cause of failure to thrive: miniseries and literature review. Ital J Pediatr. 2022; 48(1): 147.
- Wagner LM, Myseros JS, Lukins DE, Willen CM, Packeret RJ. Targeted therapy for infants with diencephalic syndrome: A case report and review of management strategies. Pediatric Blood & Cancer. 2018; 65(5): e26917.
- Yan J, Liu P, Li L, Zhou L, Liu X, et al. Diencephalic syndrome in a female child due to intracranial germinoma: a case report. Childs Nerv Syst. 2022; 38(10): 2033-2035.