Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Lepidic adenocarcinoma of the lung in a female patient
Sarra Baziaa*; M Beaouiss; S El Fathi; H Souhi; Hel Ouazzani; I Rhorfi
Department of Medicine, Mohammed V University, Morocco.
*Corresponding Author : Sarra Baziaa
Department of Medicine, Mohammed V University, Morocco.
Email: sara.bazia@gmail.com
Received : Jul 14, 2024
Accepted : Aug 07, 2024
Published : Aug 14, 2024
Archived : www.jcimcr.org
Copyright : © Baziaa S (2024).
Abstract
We present the case of a 68-year-old female patient with a history of breast cancer in remission for 12 years and ischemic heart disease. She presented with bronchorrhea and dyspnea. Initial CT imaging revealed pneumopathy, and she was treated with antibiotics. However, her symptoms persisted, and follow-up CT scans showed no change. An echo-guided biopsy was performed, which revealed lepidic adenocarcinoma of the lung.
Keywords: Invasive lepidic adenocarcinoma; Female patient; Bronchorrhea.
Citation: Baziaa S, Beaouiss M, Fathi SE, Souhi H, Ouazzani H, et al. Lepidic adenocarcinoma of the lung in a female patient. J Clin Images Med Case Rep. 2024; 5(8): 3206.
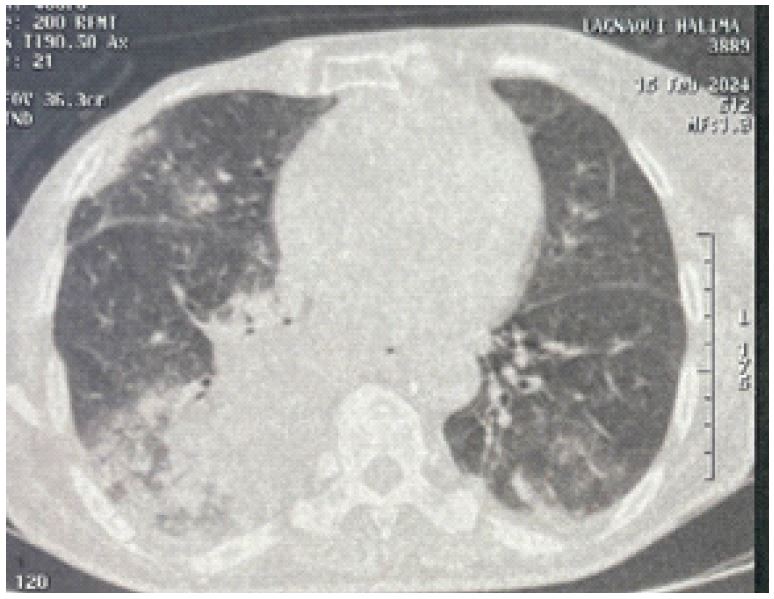
Description
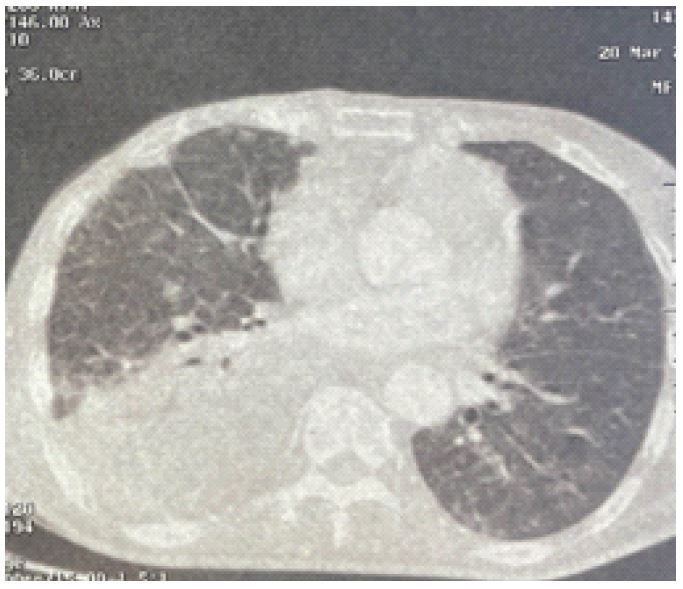
A 68-year-old female presented to emergency for 1 month progressively shortness of breath, dyspnea and weight loss. she reported important bronchorrhea. Medical history was notable for breast cancer operated and treated 12 years before, and ischemic heart disease. The patient underwent CT scan, it showed ground glass opacities located in the right upper lobe, posterior basal segmental consolidation in the right lung with air bronchogram ground-glass opacities with consolidation in the posterior basal segment of the left lung (Figure 1). Laboratory investigations revealed elevated C-reactive protein at 160; she was admitted to pulmonary service and placed on empiric antibiotic therapy with slight clinical improvement. She was readmitted after 1 month due to worsening dyspnea and persistent bronchorrhea. A follow-up chest CT scan showed persistent consolidation in the right middle and lower lobes containing air bronchograms, and a consolidation in the right upper lobe surrounded by a ground-glass opacity (Figure 2). Laboratory tests revealed a CRP of 40, a normal white blood cell count of 8400/mm3, no pathogens were identified in sputum culture. An ultrasound-guided biopsy of the consolidation was performed. Testing for Mycobacterium tuberculosis on the biopsy sample, including GeneXpert, was negative. The histopathological examination is consistent with a well-differentiated lepidic pulmonary adenocarcinoma.