
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Mystery unveiled: The dilemma of stone vs. foreign body in a 65-year-old male with intriguing urinary symptoms
Zaara Khan; Sachin Khanduri; Rohit; Ashok Gupta; Akshay Aggarwal*; Nisha; Mohammad Shahbaz; Namra Mahmood; Shaista Ejaz; Abhishek Singh
Department of Radiodiagnosis, Era’s Lucknow Medical College and Hospital, Lucknow, U.P., India.
*Corresponding Author : Akshay Aggarwal
Department of Radiodiagnosis, Era’s Lucknow Medical College and Hospital, Lucknow, U.P., India.
Tel: +91-750-790-9832;
Email: akshayaggarwal1996@live.com
Received : Jul 19, 2024
Accepted : Aug 08, 2024
Published : Aug 15, 2024
Archived : www.jcimcr.org
Copyright : © Aggarwal A (2024).
Abstract
The intriguing case report delves into the medical mystery surrounding a 65-year-old male presenting with complex urinary symptoms. Despite a history of noncompliance with hypertension and diabetes medications, the patient’s symptoms of burning micturition and incomplete bladder emptying led to a diagnostic conundrum. Through a series of investigations including Retrograde Urethrography and Micturating Cystourethrography, the presence of multiple calculi in the posterior urethra was revealed, alongside features of chronic cystitis. The successful treatment involved urethroscopy lithotripsy to remove the stones, shedding light on the importance of tailored management strategies and thorough evaluation in cases of chronic urinary issues. This case underscores the complexity of diagnosis in urological conditions and emphasizes the pivotal role of imaging studies and confirmatory tests in guiding treatment decisions.
Keywords: Calculi; Urethra; Urethroscopy, Retrograde cystourethrogram; Urinary bladder.
Citation: Khan Z, Khanduri S, Rohit, Gupta A, Aggarwal A, et al. Mystery unveiled: The dilemma of stone vs. foreign body in a 65-year-old male with intriguing urinary symptoms. J Clin Images Med Case Rep. 2024; 5(8): 3208.
Introduction
Urethral calculi are rare, accounting for approximately 2% of urinary tract calculi [1]. The most common location for these calculi is typically in the proximal urethra, frequently impacted behind the external urinary meatus or in the prostate urethra, specifically behind the narrow membranous portion [2].
These calculi usually originate from the upper urinary tract or the bladder but can also form within the urethra itself. Primary urethral calculi tend to develop within the urethra, often in conjunction with a stricture or urethral diverticulum. On the other hand, secondary calculi are more prevalent than primary ones [3].
Risk factors for stone formation comprise various dietary and medical conditions. Adequate hydration, aiming for approximately 2.5 liters of urine production daily, is recommended. Contrary to popular belief, low calcium intake can heighten stone risk by fostering increased oxalate absorption and excretion [4].
Several medical conditions, such as chronic kidney disease, hypertension, gout, diabetes mellitus, hyperlipidemia, obesity, and endocrine disorders, elevate the risk of stone formation [5]. Obesity and type 2 diabetes mellitus are notably associated with calcium oxalate and uric acid stones due to dietary patterns and metabolic shifts [6].
Struvite stones, which are produced by urease-producing bacteria like Proteus or Klebsiella, are less common and can lead to significant renal complications. Uric acid stones correspond with low urinary pH and high dietary purine consumption, while cystine stones are rare and linked to genetic conditions affecting cystine metabolism.
Case presentation
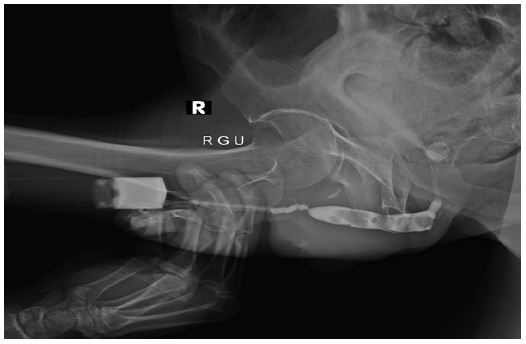
Embark on a journey into the intriguing case of a 65-year-old male who brought forth a conundrum that puzzled even seasoned medical practitioners when he presented to the psychiatric outpatient department with complaints of burning micturition and incomplete bladder emptying persisting for two years. The patient had a history of noncompliance with hypertension and diabetes medications for 15 years and occasionally took clonazepam for anxiety and insomnia. The patient appeared in good general condition with stable vitals. The patient underwent investigations including Retrograde Urethrography (RGU) and Micturating Cystourethrography (MCU), which revealed multiple round filling defects in the posterior urethra with an irregular mucosal lining, creating a visual puzzle of sorts. Is it a stone or a foreign body causing this enigmatic presentation? The plot thickens when Computed Tomography (CECT) of the abdomen shows the presence of multiple hyperdense lesions, arranged in a chain form in the posterior urethra, suggestive of calculi. Additionally, the CECT showed diffusely irregularly thickened wall of the bladder with the maximum thickness measuring 12 mm, indicating features of chronic cystitis. Further Evaluation: Urine culture and microscopy confirmed pus cells and the growth of gram-negative bacteria confirming the presence of chronic cystitis. However, the patient’s Complete Blood Count (CBC), Kidney Function Tests (KFT), and Liver Function Tests (LFT) were within normal limits, indicating no systemic complications related to the urinary condition.
Treatment and outcome: Urethroscopy lithotripsy was performed to fragment and remove the stones. Successful stone removal was achieved, with the largest stone measuring 4 x 6 mm. During the procedure, a pouch-like thickened lining was noted, suggestive of a diverticula.


Discussion
Urethral calculi are an extremely uncommon medical condition, representing less than 0.3% of all urinary calculi. They are most often seen in children because of the high frequency of bladder stones, and rarely observed in women due to the anatomic peculiarities of the female urethra [7]. These calculi are typically secondary to urethral pathologies such as urethral stenosis, diverticulum, hypospadias, urethral tumors, or meatal stenosis in young adults, and they rarely develop in a normal urethra. They are usually located in the posterior urethra and very rarely in the anterior urethra. The calculi can be solitary or multiple.
The chemical composition of stones varies. Calcium oxalate and cystine stones originate mainly from the kidneys, while struvite and uric acid stones originate from the bladder [8]. The diagnosis is often clear, involving a patient history that looks for previous urinary stone disease, episodes of passing stones, or penile pain. A clinical examination can reveal a mobile, hard urethral mass, particularly if it is not impacted and is located in the anterior urethra [9].
The treatment is not well standardized and varies based on the size, number, and location of the calculi, as well as the presence of any underlying urethral pathology or complications that could affect the surgical approach. For small proximal calculi, a minimally invasive endoscopic approach via urethroscopy is preferred. This method allows for the removal or fragmentation of the calculi in situ or the option to push them into the bladder for fragmentation by laser or lithotripsy. For larger, multiple, distal stones, or those encrusted in the urethra, conventional open surgery, such as meatotomy or sometimes urethrotomy with or without urethroplasty, is an effective therapeutic option [10].
Our case demonstrated that while multiple urethral calculi are rare, they can be a significant cause of acute urinary retention in men. The patient presented with acute urinary retention and could not undergo urethral catheterization due to the size and distal location of the calculus. Urethroscopy lithotripsy was performed to fragment and remove the stones. During the procedure, removal of calculi was achieved and a pouch-like thickened lining was noted, suggestive of a diverticula.
This case aims to highlight for practitioners, especially emergency department physicians, that multiple urethral calculi should be considered as a potential cause of catheterization failure. A straightforward clinical examination and standard imaging can often lead to a diagnosis.
Conclusion
This case underscores the importance of thorough evaluation and tailored management approach in patients with chronic urinary symptoms. The dilemma between foreign body and calculi, as well as the presence of chronic cystitis, highlights the complexity of diagnosis in such cases. Comprehensive imaging studies and confirmatory tests play a crucial role in determining the appropriate treatment strategies for patients with urological conditions.
References
- Prabhuswamy V, et al. Urethral calculi are extremely rare and constitute about 2% of the calculi in the urinary tract. 2014. doi:10.4103/0974-7796.127015.
- Danfulani, Mohammed, Saidu SA, Musa, Margery. Multiple urethral calculus misdiagnosed as urethral stricture: The role of imaging in unknotting the confusion. Asian Journal of Medical Sciences. 2016; 7: 118. 10.3126/ajms.v7i3.13874.
- Patel U. Intraluminal Abnormalities and Filling Defects of the Urethra. In Imaging and Urodynamics of the Lower Urinary Tract. Springer, London. 2010. https://doi.org/10.1007/978-1-84882-836-0_11.
- Curhan GC, Willett WC, Rimm EB, Stampfer MJ. A prospective study of dietary calcium and other nutrients and the risk of symptomatic kidney stones. N Engl J Med. 1993; 328(12): 833-8. doi: 10.1056/NEJM199303253281203.
- Bickel C, Rupprecht HJ, Blankenberg S, et al. Serum uric acid as an independent predictor of mortality in patients with angiographically proven coronary artery disease. Am J Cardiol. 2002; 89(1): 12-7. DOI: 10.1016/S0002-9149(01)02161-3 (SpringerLink).
- Antonelli JA, Maalouf NM, Pearle MS, Lotan Y. Use of the national health and nutrition examination survey to calculate the impact of obesity and diabetes on cost and prevalence of urolithiasis in 2030. European Urology. 2014; 66(4): 724-729. https://doi.org/10.1016/j.eururo.2014.06.036.
- Kamal BA, Anikwe RM, Darawani H, Hashish M, Taha SA. Urethral Calculi: Presentation and Management. BJU International. 2004; 93: 549-552. https://doi.org/10.1111/j.1464-410X.2003.04660.x.
- Wein AJ, Kavoussi LR, Novick AC, et al. Campbell-Walsh Urology (Campbell’s Urology (4 Vols.)). Saunders. ISBN:B0069S9RB0.
- Mbouché LO, Andzé GO, Makon ASN, Bob DN, Tamufor EN, et al. Acute Urinary Retention in the Male Child from Urethral Calculi: A Report of Three Cases. Case Reports in Urology. 2019. Article ID: 5762139. https://doi.org/10.1155/2019/5762139.
- Agwu NP, Abdulwahab-Ahmed A, Sadiq AM, Oyibo EU, Mungadi IA. Management of Impacted Urethral Calculi: An Uncommon Cause of Acute Urine Retention in North-Western Nigeria. International Journal of Clinical Urology. 2020; 4: 1.