
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
The puzzle of aphasia: An overall picture of a persian fluent aphasia patient
Narges Bayat1; Zahra Ghoreyshi2*; Mohanna Javanbakht3
1Faculty of Health Sciences, School of Rehabilitation Sciences, University of Ottawa, Ottawa, Canada.
2Assistant Professor, Speech Therapy Department, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
3Assistant Professor, Audiology Department, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
*Corresponding Author : Zahra Ghoreyshi
Assistant Professor, Speech Therapy Department, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
Tel: 00982122180043 & 00982122190043;
Email: za.ghoreyshi@uswr.ac.ir
Received : Jul 27, 2024
Accepted : Aug 13, 2024
Published : Aug 20, 2024
Archived : www.jcimcr.org
Copyright : © Ghoreyshi Z (2024).
Abstract
Aphasia, an acquired neurogenic language disorder, is a deficit in the expression and comprehension of language. This article presents a comprehensive assessment of a 59-year-old Persian-speaking individual, M.N., who experienced fluent aphasia as a result of an ischemic stroke in the left temporoparietal lobe. Persian Western Aphasia Battery, Persian Picture Naming test, Token test, Verbal Apraxia test, and Mini-Mental State Examination (MMSE) were used to evaluate language, speech, and cognition abilities respectively. After conventional hearing tests, central auditory processing tests were also performed to evaluate his auditory functioning. According to the results, he had moderate conduction aphasia (AQ=52%) with severe repetition problem, moderate naming disorder (54%), auditory comprehension impairment (15 out of 36 in the Token test), moderate to severe verbal apraxia (scored 41 out of 50), mild cognitive deficit (scored 21 out of 30 in MMSE), dichotic listening deficit (25% right ear and 55% left ear in Dichotic-Digit-Test), and temporal processing limitation (gap detection of 25 sec and more), and perceiving problems in the close set Word-In-Noise test (number of words identified correctly were 25 out of 35 in the right ear and 23 out of 35 in the left ear). This study highlighted the importance of having a comprehensive assessment in persons with aphasia.
Keywords: Aphasia; Language impairment; Cognitive deficit; Auditory processing; Auditory comprehension.
Citation: Bayat N, Ghoreyshi Z, Javanbakht M. The Puzzle of aphasia: An overall picture of a persian fluent aphasia patient. J Clin Images Med Case Rep. 2024; 5(8): 3215.
Introduction
Aphasia, an acquired neurogenic language disorder, is a deficit in the expression and comprehension of language [1]. Speech fluency is an important concept for understanding aphasia syndromes; therefore, the fluent and nonfluent aphasia classification system was devised. The prosodic or melodic characteristics of speech are the primary distinguishing factors for fluent and nonfluent aphasia types [2,3]. Fluent aphasia is often associated with lesions posterior to the fissure of Rolando (central sulcus), primarily in and around the language areas in the temporal lobe of the left hemisphere (perisylvian region). However, nonfluent aphasia is associated with lesions anterior to the fissure of Rolando, primarily around Broca’s area in the premotor strip of the speech areas of the left frontal lobe [3]. Although being fluent or nonfluent refer to expressive language characteristics, patients described with this classification system tend to have certain common receptive language characteristics as well [1]. In order to identify the type of aphasia and its severity, develop a personalized treatment plan tailored to the patient’s needs, and monitor progress, it is necessary to perform a comprehensive assessment [1]. Language and cognition are among the main functions of the brain; therefore, in persons with aphasia, we need to have an in-depth look into these functions [3]. Patients with aphasia may also experience disruptions in the motor aspects of speech which needs to be assessed [4]. Some aphasiologists, the most notable among them being Hildred Schuell (1964), have implied that auditory comprehension deficits form the underlying and unifying disorder in aphasia (possibly because of the auditory learning of language) [5-7]. According to Sarno (2017), auditory comprehension deficit is noticeable in patients with fluent aphasia [8]. Lesions in the right or left temporal lobes may affect auditory processing associated with Central Auditory Processing Disorder (CAPD) symptoms [9]. Bergemalm and Lyxell (2005) also reported that CAPD can be seen in more than 50% of adults with brain damage due to stroke [10]. Due to this high prevalence of CAPD in post-stroke patients, audiological evaluation is essential to detect CAPD in persons with aphasia, while there are no auditory processing tests in aphasia-related research [11]. The question is then, do we need a person with fluent aphasia’s auditory profile in addition to his language, cognition, and motor speech profile? In this study, we aimed to have a comprehensive assessment of a person with aphasia and discuss the hierarchy of a comprehensive assessment in these patients.
Case study
M.N. is a 59 years old right-handed man who has a bachelor’s degree in accounting and currently is retired. According to the patient’s report, all the family members (mother, father, brother, and grandparents) are right-handed. The patient was healthy and capable before the stroke and had no sensory, motor, or brain damage in childhood and adulthood. M.N. had an ischemic stroke in the left temporoparietal lobe in 2017 (2 years before assessment). Figure 1 demonstrates the site of the damage in his MRI result. According to the patient’s companion, he was not able to recognize people surrounding him during the first two to three days post-stroke. The patient received 8 months of speech therapy after the stroke. During the assessment, he had no motor problems but only had a mild sensory deficit on his right side of the body. As part of the research initiative approved by the University of Social Welfare and Rehabilitation Sciences with ethics code IR.USWR.REC.1395.401, the subject of this study initially referred to the speech therapy department. However, as the individual did not meet the inclusion criteria, he was not included in the sample of that study. Subsequently, with the consent of the patient, he referred for additional evaluations and the present article was written according to these evaluations. Language, speech, cognitive, and auditory assessments were performed after acquiring informed consent from the patient. Assessment sessions were done in a clinic related to the University of Social Welfare and Rehabilitation Sciences. There were multiple sessions to complete the assessments. During the sessions, if the patient felt tired, the assessment process was stopped for a few minutes. In order to comply with professional ethics, some treatment recommendations were given to the patient in each session. To assess the patient’s language abilities, the bedside version of the Persian Western Aphasia Battery (P-WAB-1) [12] and the Persian Picture Naming test [13] were implemented. P-WAB-1 has six sub-tests including spontaneous speech content, spontaneous speech fluency, auditory comprehension, sequential commands, repetition, and naming. Each subscale has 10 points and the maximum raw score of the test is 60. A percentile Aphasia Quotient (AQ) also can be formulated in order to determine the severity of aphasia [12].
The Persian Picture Naming test evaluates the severity of the naming deficit by evaluating the patient’s ability to name 50 pictures. According to the instructions of this test, semantic and phonetic cues can be given to the M.N., which in the end differentiates between aphasic and cognitive naming disorders [13].
Oral and verbal apraxia tests were implemented to evaluate motor-oral and verbal skills. The oral apraxia test includes two forms (verbal command form and imitation form). These two forms are scored and interpreted separately, and based on the results, the presence or absence of the disorder and its severity can be determined. This test has 22 questions, and with a correct answer, the patient gets a score of 0, a wrong answer gets a score of 1, and if the patient does not answer, a score of 2. The total score of this test is 44, which indicates the most severe level of apraxia. In this test, if a person scores 3 or less, he does not have oral apraxia, but if he scores 4 or more, he has oral apraxia. Repeating speech sounds and words, saying the sounds of letters, reading words, repeating sentences, memorizing automatic speech series, telling stories, and free speech are various sections of the verbal apraxia test. In this test, if the participant’s score is 12 or less, he does not have verbal apraxia. But if the participant’s score is 13 or more, it indicates the presence of verbal apraxia [14].
The Mini-Mental State Examination (MMSE) was used to evaluate the patient’s cognitive status. The maximum score of this test is 30 and the cut-off point is 22. This test includes questions about time and place orientation, repetition, attention and calculation, memory, language assessments, and copying [15]. Another test that was used for the cognitive evaluation of M.N. was the software version of the Wisconsin Card Sorting Test (WCST), which evaluates executive functioning. In this test, the participant must match the desired card with one of the 4 displayed cards in terms of color, shape, or number of symbols. Then the desired rule of the test suddenly changes and the patient must be able to discover the new rule and continue it. The 64-card version of this test was used to evaluate this patient [16]. Digit Span Forward Test (DSF) and Digit Span Backward Test (DSB) were also investigated to estimate working memory capacity [17]. To evaluate auditory comprehension skills, the Token test was used. This test has 36 commands that become more complex and the patient is asked to perform the commands [18]. Additionally, comprehensive examinations of peripheral hearing (otoscopy, audiometry, tympanometry, and acoustic reflex) and central auditory processing (Speech-in-Noise test, dichotic hearing test, and temporal processing test) were performed for the patient during three one-hour sessions.
In this study, Welch Allyn otoscope and tympanometer AT235, Intracoustics Co, Denmark were used to confirm the health of the eardrum and middle ear. Audiometric evaluations were performed using an AC40 audiometer, Intracoustics Co, Denmark, at conventional audiometric frequencies from 250 to 8000 Hz, and hearing thresholds were recorded in Air Conduction (AC) and Bone Conduction (BC) pathways. Since M.N. had working memory problems, the Persian version of the Wond in Noise (WIN) test was used instead of conventional sentence comprehension tests, such as the Persian version of the Quick- Speech-In-Noise (QSIN) test. The patient also had repetition problems; therefore, the closed pictural version of the WIN test was implemented. The WIN test was performed using a calibrated laptop and headphones. The test consists of a list of 35 words for each ear, and each five words is presented via headphones at one of the Signal-to-Noise Ratios (SNR) of 0, 4, 8, 12, 16, 20, and 24 decibels for each left and right ears. Scores below 30 for individuals over the age of 12 are considered abnormal. The test was conducted in an acoustic room at a comfortable hearing level (40dB SL).
To investigate dichotic auditory processing, the Persian version of the Dichotic Digit test was used. In this test, two pairs of monosyllabic numbers (between 1 and 10, except number 4 which has two syllables in Persian) are presented to the left and right ears at the same time via headphones. The subject is asked to repeat all 4 numbers heard in both ears. In adults over 12 years of age, a score of 90% and above in each ear is considered the norm and confirms the health of dichotic auditory processing and the communication pathway of the corpus callosum.
Auditory temporal processing in this study was investigated using the Random Gap Detection test for each ear at frequencies of 1 and 4 kHz and with silence intervals of 0 to 40 milliseconds. The ability to recognize time intervals of 20 milliseconds or less is required to recognize temporal changes in speech processing.
Results
Language, oro-motor, cognitive, and auditory assessments were performed. First, the results of the language assessment are reported. According to the P-WAB-1 [12], the patient demonstrated deficits in all the subtests (spontaneous speech content, fluency of spontaneous speech, auditory comprehension, sequential commands, repetition, and naming), but he had a significant repetition deficit. The results of this test are demonstrated in Figure 2. The patient’s AQ in the P-WAB-1 was 52%, indicating moderate conduction aphasia. The patient’s score in auditory comprehension of yes/no questions was 7 out of 10 and in understanding continuous commands was 6 out of 10. These results indicate the patient’s auditory comprehension deficit. The patient’s score in the naming subtest was 5 out of 10, which indicates his word-finding deficit. The patient’s score in repetition is 1 out of 10 and shows his severe deficiency in this skill. The patient’s rate of speech in describing the bird’s nest picture is 72 words per minute, which scores 7 out of 10 in the fluency of spontaneous speech; therefore, the patient’s speech is fluent. His content score is 5 out of 10, which indicates that at least half of the statements are meaningless and empty. In general, according to the results of the P-WAB-1 [12], M.N. has an auditory comprehension deficit, but he functions well at simple levels. He has word-finding deficits and difficulties in conveying meanings. His repetition deficit is evident and his speech is fluent. Analyzing the continuous speech of M.N. provided information on his quality of speech. Parts of the patient’s speech sample describing the events at the time of the stroke and picture description (the bird’s nest picture) and the results of the speech analysis are presented in the following. Table 1 demonstrates the quality of speech indexes such as the rate of speech and Mean Length Utterance (MLU).
Speech sample of the patient describing the events at the time of stroke (original version in Persian with English translation):
نیا زا رتهب / امش هب مضرع / مداسیاو هک یتقو نم نیمه / هگید هنیمه متسه هکنیا / منک تبحص منوتیمن دعب / مباوخب هدروخی هک ماوخیم / دش مامت مزامن زا دعب هک منودیمن / مباوخب هدروخی متساوخیم هک دعب / امش هب مضرع هی مدید / مدب مدید نوچ نم ونیا / مباوخب نم هک مراذب ونیا وت منزب نییاپ مرب / مدوب هداسیاو نم الثم / متسه یروج هشیمن هگید تفگ / مباوخب ماوخ یم / دش مامت هگید / الثم /دش مامت هگید هن تفگ / مباوخب متفگ /
When I stood up / I apologize to you / I can’t speak better than this / This is what I am / As soon as I finished my prayer / I want to go to sleep / Then my intend to you in that / After I wanted to get some sleep / I don’t know I put this to go to sleep / I gave this because I saw it / I saw that I was in a certain way / for example, I was standing / I’ll go down knock in, for example / it’s over / I want to sleep / he said it isn’t possible anymore / I said to sleep / he said no, it’s over /
In this speech sample, M.N. describes the events that happened at the time of the stroke and how he was not able to do anything during that time. The patient’s companion confirmed these explanations. These errors can be found in his speech sample:
Inability to form proper sentences and use suitable words in conveying the meaning, having a limited number of content words, and incoherent sentences.
The patient cannot find the proper lexicon and sentence structure in conveying his meaning. Therefore, circumlocution is evident in his speech sample while he could convey the same meaning in two or three sentences.
This patient is a patient with fluent aphasia since his rate of speech was 95.6 words per minute. Also, we can find a sentence with six words in his speech sample, while a patient with non-fluent aphasia often does not produce sentences with more than four words in a sentence [1].
There are some semantic-related deficits in this speech sample. For example, “I don’t know I put this” does not convey a specific meaning.
This is the patient’s speech sample describing the bird’s nest picture in the P-WAB-1 [12] (original version in Persian with English translation):
/نوشیا نوشیا / هدش یروجنیا / هنوشیا / هراد مناخ / نوشیا ورتکد / شوت / هدموا نوریب ینعی / نییاپ هدموا / الاب نیا زا دایب / نییاپ هتفیب راذب / نوسرب شهب / نوریب دیزادنب هراذب مش هچب / هنزیم دعب / امش هب مضرع / تفر / نییاپ مضرع و / نییاپ هسریم دعب / نییاپ هراذب / هرابود نییاپ /نییاپ داتفا هعفد کی / امش هب
She / She is / She is / This is what happened / He, He / From this top / He came down / I mean; he came out / Inside / Eject the doctor / Reach him / Let it fall down / Come down / Went / My intent to you is that / Then hits / Put its baby down again / Put down / Then reaches down / And my intent to you / Suddenly fell down
These errors are seen in this speech sample: The patient has limited access to the lexicon. For example, “She / She is / She is” is just a repetition of pronouns and there is no content lexicon.
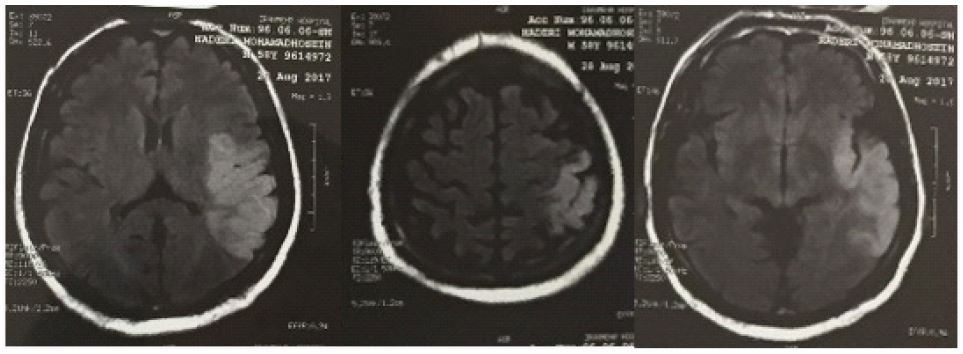
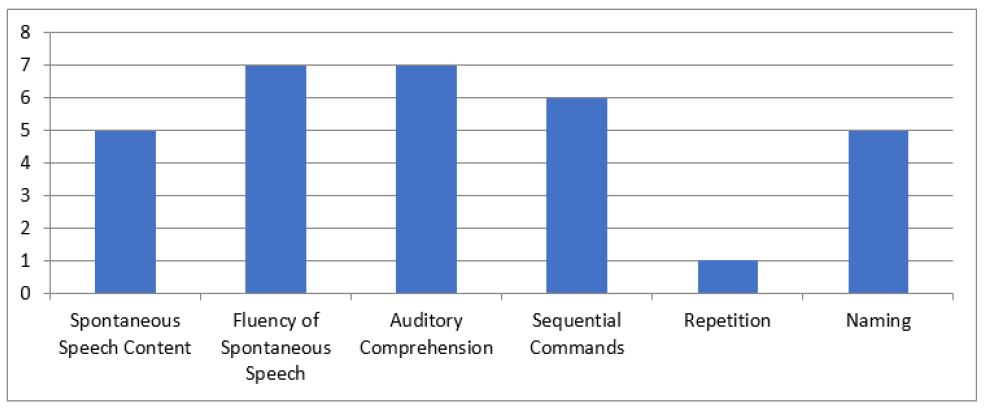
Table 1: Continuous speech analysis of the patient.
| Speech sample | Subject | Total number of the words | Duration(minutes) | Number ofutterances | Rate of speech (words per minute) | MLU |
|---|---|---|---|---|---|---|
| Free | Description of the eventsat the timeof stroke | 371 | 3.88 | 95 | 95.6 | 3.9 |
| Descriptive | The bird’snest picture | 93 | 0.88 | 37 | 112 | 2.5 |
Table 2: Examples of the patient’s paraphasias and fillers.
| Type | Intended word | Produced word |
|---|---|---|
Phonological paraphasias |
Fæsl (season) | Væsl |
| Dastan (story) | Bastan | |
| Kolah (hat) | Tolah | |
| Mix (nail) | Xix | |
| Sæg (dog) | Sæk | |
| Šæmʔ (candel) | Šæf | |
| Čængal (fork) | Gængal | |
| Æbr (cloud) | Æbs | |
| Hævij (carrot) | Hæsib | |
Semanticalparaphasias |
Khanom (woman) | Aqa (man) |
| Mi-istæm (I am standing) | Mi-nešinam (I am sitting) | |
| Čaqu (knife) | Qašoq (spoon) | |
| Sobh (morning) | Šæb (night) | |
| Dayere (circle) | Bošqab (plate) | |
| mi-bændim (we areclosing) | Češm (eye) | |
| Gorbe (cat) | Xærguš (rabbit) | |
| Fillers | Ærzæm be šoma (my intentto you is that…) | |
Table 3: The patient’s profile.
| Test | Score | Score (%) |
|---|---|---|
| P-WAB-1 | 52% | 52% |
| Persian picture naming test | 54% | 54% |
| Token test | 15 out of 36 | 41.66% |
| Verbal apraxiatest | 41 out of 50 | 82% |
| MMSE | 21 out of 30 | 70% |
| Speech-in-noise test | Right: 25 out of 35 Left: 23 out of 35 |
Right: 74.1% Left: 65.7% |
| Dichotic digittest | Right: 10 out of 40 Left: 22 out of 40 |
Right: 25% Left: 55% |
| Random gap detection test | minimum detectable gapin both ears was 25 milliseconds |
In the “Eject the doctor” section, the patient has seen the photo of the doctor in the picture and knows what he has to say, but cannot convey the right meaning, and produces an utterance which is not semantically correct according to the picture.
The patient produces many sentences for describing a picture that can be described with a short sentence, which demonstrates the semantic deficit.
The patient’s performance in answering open-ended and closed-ended questions was also examined. Due to severe word-finding difficulties, M.N. did not perform well in answering any of the open-ended or closed-ended questions. For example, to assess the patient’s skill in answering open-ended questions, he was asked to explain what happened to him at the time of the stroke. M.N. uttered 371 words in about 4 minutes, while he could explain the whole incident with two to three short sentences. To assess closed-ended questions, the patient was asked to answer questions such as “How many wheels does a car have?” or “Name the seasons.” While the patient could answer these questions with one or more words, he answered them with more than one sentence.
According to a study published in 2014, the normal rate of speech in Persian men is reported 119.38 (+28.32) words per minute [19]. Therefore, the patient’s rate of speech is normal. His rate of speech in the descriptive speech sample was more than the free speech sample. His MLU was lesser than normal people and he produced shorter sentences.
M.N. had self-corrections (mostly phonetic). He would stop during speech and try several times to pronounce the word correctly. For example, when saying the word “his hand” (/dæstæʃ/ in Persian), the patient said “/ dæstæs /” three times until he was able to produce it correctly the last time. Or to express the word “to go” (/berævæd/ in Persian), he produced “/berævæt/” three times, but he could not achieve the correct pronunciation of the word.
Many paraphasias and fillers were observed in the patient’s speech, and the number of phonological paraphasias was more than semantic paraphasias. In Table 2, you can see examples of these paraphasias and fillers.
In order to evaluate the patient’s naming skill, the Persian Picture Naming test was used [13]. Based on this test, 54% of the patient’s answers were correct, which indicates the severity of moderate disorder. The number of correct answers by M.N. was higher with phonetic cues than with semantic cues. Therefore, the use of phonetic cues over semantic cues was considered in the treatment process. The Token test was used to assess the patient’s auditory comprehension skills. The patient scored 15 out of 36(66.41%). According to this test, 90% of the normal population scored 36, and only 10% of them scored 29 to 36 [18]. In the oral apraxia test, M.N. scored 2 which indicates no oral apraxia. He was able to perform most of the commands without visual cues and with sufficient accuracy. In the verbal apraxia test, the patient scored 41 out of 50, which confirms moderate to severe verbal apraxia [14]. MMSE [15] and the WCST were used to assess the patient’s cognitive abilities. His score in the MMSE was 21 out of 30. M.N. functioned normally in the consciousness section, but he had severe deficits in attention and calculation, memory, three-step order, and repetition. In the WCST [16], the patient’s wrong answers were more than his correct answers. He could not follow the rule of matching the cards and this result shows the patient’s attention and executive function deficits. In the DSF and DSB tests, the patient’s working memory capacity was 4 and 2 units respectively, which was less than the norm of working memory capacity (7±2) [17].
The results of otoscopy and tympanometry in both ears were normal (type an), which indicated the health of the outer and middle ear. In AC and BC audiometry, mild to moderate bilateral symmetric sensorineural hearing loss was seen in frequencies above 2000 Hz, which seems to be appropriate to his age and history of exposure to noise. The patient’s speech comprehension score in silence using monosyllabic words and answering the closed set was 90% in the right ear and 85% in the left ear, which is considered close to the norm. But in the WIN speech comprehension test in noise, the number of words Correctly identified was 25 out of 35 in the right ear and 23 out of 35 in the left ear, which is abnormal in both ears and indicates a mod moderate speech perception disorder in noise. In the DDT test, the score of the right ear was 25% and the score of the left ear was 55%, which indicates a clear dichotic hearing disorder in M.N., and the left shows a clear superiority in the patient. The results of the Random Gap Detection test indicated a slight problem in time processing and the minimum detectable gap in both ears was 25 milliseconds. The profile of M.N. based on the language, oro-motor, cognition, and auditory processing assessments is demonstrated in Table 5.
Discussion
Aphasia is a language disorder that develops as a result of damage to specific regions of the brain. Individuals with aphasia often experience difficulties in both understanding and expressing language, which can impact their ability to communicate effectively [1]. Conducting a comprehensive assessment of aphasia holds significant importance. This process leads to determining the type and severity of language deficits, which facilitates diagnosis and treatment planning [1-20]. The presented article offers a detailed and comprehensive assessment of a Persian-speaking individual, M.N., who has experienced fluent aphasia following an ischemic stroke. Through this assessment process, we evaluated the patient’s language, oro-motor, cognitive, and auditory abilities. According to the P-WAB-1 [12] results, the patient diagnosed with a moderate conduction aphasia. A significant impairment in repetition was evident in the test outcome. Research confirms the presence of repetition deficit as one of the most common symptoms in conduction aphasia [21]. The patient’s speech was fluent and rhythmic, with only pauses attributed to lexical retrieval and self-correction. Additionally, the use of fillers was observed, a characteristic that Benson et al. (1973) identify as distinctive between conduction and Broca’s aphasia [22]. Furthermore, various paraphasias (mostly phonological and a few semantic) were evident, and the patient was aware of them and tried to do self-corrections. Studies comparing self-correction behaviors among individuals with conduction, Broca’s, and Wernicke’s aphasia have reported that individuals with conduction aphasia are more likely to recognize their errors, but are not more successful in correcting them compared to those with Broca’s or Wernicke’s aphasia [1]. In the case of patient M.N., it was also observed that these self-corrections often led to frustration and impeded his expressive capacities. Notably, refraining from self-correction and continuing with his speech allowed for clearer and more comprehensible expression of his intended meaning. Repetition was severely affected, and even during single-syllable word repetition, the patient experienced phonological paraphasias. Word retrieval difficulties were also present, which is considered a common impairment in conduction aphasia [21]. Furthermore, an assessment of speech fluency in the patient was conducted. By calculating the patient’s speech rate, it becomes evident that his speech is fluent. Additionally, word finding problems were identified, manifesting as a reduced number of content words within the patient’s speech, often accompanied by circumlocutions. These findings align with Buckingham and Kertesz’s (1974) study, which underscores conduction aphasia as a subtype characterized by fluent speech alongside deficits in word-finding [23]. As outlined by Benson et al. (1973), individuals afflicted with conduction aphasia tend to exhibit sound reading comprehension [22], yet their oral reading is characterized by paraphasic errors [1]. Similarly, in the case of M.N., oral reading also demonstrated a prevalence of paraphasic occurrences; however, the comprehension of written text exhibited comparatively higher proficiency. Notably, the patient displayed a greater inclination towards self-expression through written means rather than oral ways. Moreover, it is noteworthy that the frequency of phonological paraphasias has shown an increase in subsequent sessions as opposed to initial sessions. This increase is indicative of a rise in the usage of content words, given that paraphasias are less likely to occur in empty speech but are more prominent in speech with content [24]. In the Token test [18], the patient exhibited an increase in corresponding to the length of the instructions and their complexity. A similar pattern of performance was observed in the study by Strub et al. (1974) wherein a patient with conduction aphasia displayed diminished proficiency in the Token test [25]. As the instructions of this test become more complex, the role of auditory memory becomes more important. The patient’s decline in performance during these higher-level instructions could potentially be attributed to auditory memory problems. Evidently, the patient’s auditory memory capacity was limited to three items. Furthermore, the decrease in the patient’s performance in higher levels of the Token test might be attributed to underlying language deficits, specifically to syntax and semantics deficits. The auditory deficit is evident not only within the patient’s language profile but also in the outcomes derived from the Token test. The reasons for that could be rooted in a combination of linguistic and cognitive deficits, specifically memory deficits. The assessment findings indicated an absence of oral apraxia symptoms in the patient. However, according to the case presented by Ochipa et al. (1994), the patient exhibited verbal apraxia [26]. Similar to the observed instance, M.N. displayed an escalation of errors as the phonological chain increased during the verbal apraxia test. Notably, the patient engaged in apparent and audible search behaviors, accompanied by numerous off-target attempts. While the patient was aware of his unstable mistakes, he was unable to correct them. Non-linguistic cognitive impairments are evident in individuals who have experienced left hemisphere stroke [27], which was also evident in M.N. According to Erickson et al. (1996), deficits in attention and executive function are prevalent among individuals with conduction aphasia [28]. The cognitive assessments conducted on patient M.N., as evidenced by the MMSE and the WCST, further emphasize the presence of attention and executive function deficits. While Bell et al. (1997) attribute deficit in the WCST to frontal and prefrontal brain damage [29], it’s worth noting that the MRI report for patient M.N. does not indicate any damage in these areas; rather, the observed damage is reported to the temporoparietal region. A notable aspect of this study is the focus on auditory comprehension deficits in individuals with fluent aphasia. According to the results, M.N. demonstrated auditory processing disorder, highlighting its significance as a crucial element in the comprehensive assessment of aphasia. Kumar et al. (2016) suggested that patients with aphasia might exhibit intact peripheral hearing sensitivity up to cochlea, yet encounter difficulties in complex auditory tasks, potentially linked to symptoms of CAPD. Thus, including audiological assessments becomes imperative for the identification of CAPD in individuals with aphasia [30]. Intervention is the step that comes after assessment. Interventions targeting language, cognition, and auditory processing hold substantial potential for yielding favorable outcomes in the case of this patient, as well as those presenting similar conditions characterized by conduction aphasia. Future research can evaluate various treatment methods through the lens of single-subject studies, thus advancing our understanding of efficacious therapeutic approaches.
This study is valuable as it sheds light on the multifaceted nature of aphasia and the importance of conducting a thorough evaluation to understand its various dimensions, including language, cognitive, motor, and auditory aspects.
Conflicts of interest: The authors report no conflict of interest.
References
- LaPointe LL. Aphasia and related neurogenic language disorders: Thieme Medical Pub. 2005.
- Feyereisen P, Pillon A, Partz M. On the measures of fluency in the assessment of spontaneous speech production by aphasic subjects. Aphasiology. 1991; 5(1): 1-21.
- Goodglass H, Kaplan E. The assessment of aphasia and related disorders: Lea & Febiger. 1972.
- Pedersen PM, Jorgensen HS, Kammersgaard LP, Nakayama H, Raaschou HO, et al. Manual and oral apraxia in acute stroke, frequency and influence on functional outcome: The Copenhagen Stroke Study. American journal of physical medicine & rehabilitation. 2001; 80(9): 685-92.
- Schuell HM. Aphasia in adults: Diagnosis, prognosis, and treatment. Hoeber Medical Division. 1964.
- McNeil MR, Kimelman MD. Toward an integrative information-processing structure of auditory comprehension and processing in adult aphasia. Seminars in Speech and Language. 1986; 7(02): 123-46.
- Caplan D. Biological studies of mental processes: Mit Press. 1980.
- Sarno MT. Aphasia. Reference Module in Neuroscience and Biobehavioral Psychology: Elsevier; 2017.
- Kimura D. Cerebral dominance and the perception of verbal stimuli. Canadian Journal of Psychology/Revue canadienne de psychologie. 1961; 15(3): 166-71.
- Bergemalm PO, Lyxell B. Appearances are deceptive? Long-term cognitive and central auditory sequelae from closed head injury. International journal of audiology. 2005; 44(1): 39-49.
- Musiek FE, Chermak G. Testing and treating (C) APD in head injury patients. The Hearing Journal. 2008; 61(6): 36-8.
- Nilipour R, Pourshahbaz A, Ghoreyshi ZS. Reliability and Validity of Bedside Version of Persian WAB (P-WAB-1). Basic Clinical Neuroscience. 2014; 5(4): 253-8.
- Nilipour R, Bakhtiar M, Momenian M, Weekes BS. Object and action picture naming in brain-damaged Persian speakers with aphasia. Aphasiology. 2017; 31(4): 388-405.
- Yadegari F, Azimian M, Rahgozar M, Shekarchi B. Brain areas impaired in oral and verbal apraxic patients. Iran J Neurol. 2014; 13(2): 77-82.
- Ansari NN, Naghdi S, Hasson S, Valizadeh L, Jalaie S. Validation of a Mini-Mental State Examination (MMSE) for the Persian population: a pilot study. Applied neuropsychology. 2010; 17(3): 190-5.
- Heaton RK. Wisconsin card sorting test manual. Psychological assessment resources. 1981.
- Choi HJ, Lee DY, Seo EH, Jo MK, Sohn BK, et al. A normative study of the digit span in an educationally diverse elderly population. Psychiatry investigation. 2014; 11(1): 39-43.
- Aliniaye Asli P, Ghoreishi Z, Maroufizadeh S. Preparation of Persian auditory comprehension test and determining its psychometric properties. Shenakht Journal of Psychology and Psychiatry. 2021; 8(4): 24-37.
- Ghoreishi ZS, Azimian M, Khorrami banaraki A, Alaghband rad J, Rafiee SM, et al. Lexical Access in Persian Normal Speakers: Picture Naming, Verbal Fluency and Spontaneous Speech. Iranian-Rehabilitation-Journal. 2014; 12(2): 16-20.
- Spreen O, Risser AH. Assessment of aphasia: Oxford University Press.2003.
- Bernal B, Ardila A. The role of the arcuate fasciculus in conduction aphasia. Brain: A journal of neurology. 2009; 132(9): 2309-16.
- Benson DF, Sheremata WA, Bouchard R, Segarra JM, Price D, et al. Conduction Aphasia: A Clinicopathological Study. Archives of Neurology. 1973; 28(5): 339-46.
- Buckingham HW, Kertesz A. A linguistic analysis of fluent aphasia. Brain and Language. 1974; 1(1): 43-61.
- Caramazza A, Basili AG, Koller JJ, Berndt RS. An investigation of repetition and language processing in a case of conduction aphasia. Brain and Language. 1981; 14(2): 235-71.
- trub RL, Gardner H. The repetition defect in conduction aphasia: Mnestic or linguistic? Brain and Language. 1974; 1(3): 241-55.
- Ochipa C, Rothi L, Heilman K. Conduction apraxia. Journal of Neurology, Neurosurgery & Psychiatry. 1994; 57(10): 1241.
- Lee B, Pyun S. Characteristics of Cognitive Impairment in Patients With Post-stroke Aphasia. arm. 2014; 38(6): 759-65.
- Erickson RJ, Goldinger SD, LaPointe LL. Auditory Vigilance in Aphasic Individuals: Detecting Nonlinguistic Stimuli with Full or Divided Attention. Brain and Cognition. 1996; 30(2): 244-53.
- Bell MD, Greig TC, Kaplan E, Bryson G. Wisconsin card sorting test dimensions in schizophrenia: Factorial, predictive, and divergent validity. Journal of Clinical and Experimental Neuropsychology. 1997; 19(6): 933-41.
- Kumar P, Mohan BM, Pavithra K, Naveen CP. Exploring (central) auditory processing deficits in individuals with Broca’s aphasia: Based on case study. 2016; 22(2): 135-8.