
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Furuncular myiasis in a Saudi male: Case report
Remah Alzayyat1*; Ahrar Alsaihati1; Nouf Bin Rubaian2; Ayman El-Badry2; Inaam Aldamanhori2
1Department of Dermatology, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia.
2Department of Microbiology, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia.
*Corresponding Author : Remah Alzayyat
Department of Dermatology, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia.
Email: remah.business@gmail.com
Received : Jul 28, 2024
Accepted : Aug 14, 2024
Published : Aug 21, 2024
Archived : www.jcimcr.org
Copyright : © Alzayyat R (2024).
Abstract
Background: Furuncular myiasis is a well-known cutaneous parasite in tropical regions. Common risk factors include low socioeconomic status, an unhygienic environment, contact with animals, a weakened immune system (malignancy), and inadequate wound care.
Objective: To report a rare case of myasis of a 23-year-old Saudi male, a condition that is not commonly seen.
Case presentation: This is a 23-year-old healthy Saudi male who presented to our emergency department with multiple nodular lesions of 6 days duration. Lesions were associated with severe pruritis. Upon skin examination, multiple widespread erythematous furuncles had a central punctum over the legs, arms, and trunk. We noticed ten nodules. We instructed the patient to apply petroleum jelly over all the lesions and return two days later. We took a skin biopsy. We sent all the larvae to a parasitologist for analysis, and he identified them as Cordylobia anthropophaga (Tumbu fly). We referred the patient to the dressing clinic for proper wound care and instructed him to apply fusidic acid ointment three times daily for seven days. Two weeks later, the lesions resolved entirely.
Conclusion: Myiasis can occur in several parts of Saudi Arabia; however, it is uncommon. Understanding this condition, its epidemiologic trends, and its diagnostic traits can help avoid long wait times for diagnoses and pointless procedures.
Keywords: Myiasis; Furuncular myiasis; Skin infestation; Tumbu- fly; Saudi Arabia.
Citation: Alzayyat R, Alsaihati A, Rubaian NB, El-Badry A, Aldamanhori I. Furuncular myiasis in a Saudi male: Case report. J Clin Images Med Case Rep. 2024; 5(8): 3216.
Introduction/Background
Myiasis, coined from the Greek word ‘myia’ meaning fly, is the infestation of live or dead tissues of vertebrates (humans and animals) by immature stages (maggots) of dipteran flies [1]. Although it exsist around the world, reports of it are more common in tropical areas due to the presence and geographic spread of several fly species [2]. Three subtypes of cutaneous myiasis exists localized furuncular myiasis, migratory myiasis, and wound myiasis [1]. Low socioeconomic status, an unhygienic environment, tropical climate, animal contact, a weakened immune system (malignancy), and inadequate wound care are common risk factors [1-3].
Objective
Myiasis is an underestimated and unfamiliar problem for most healthcare providers in Saudi Arabia. We present a case of a 23-year-old Saudi male who presented to our clinic with multiple nodules and punctum and we took a biopsy and we reached a diagnosis of furuncular myiasis.
Case presentation
This case is a 23-year-old healthy Saudi male who presented to our emergency department with multiple nodular lesions of 6 days duration. The lesions started over his legs one day after returning from Abha, where he stayed in a chalet. After that, it progressed to involve the trunk both anteriorly and posteriorly. Lesions were associated with severe pruritis. The patient noticed something coming out of one of the lesions. Upon skin examination, multiple widespread erythematous furuncles had a central punctum over the legs, arms, and trunk. We noticed ten nodules. we appreciayed movements of the larvae hrough the punctum of some lesions with some frothy secretions. We instructed the patient to apply petroleum jelly over all the lesions and return two days later. We took a skin biopsy. Upon follow-up, two-thirds of dead larvae protruded from the punctum in most lesions.
We manually extracted using forceps after intra-lesional lidocaine, which pushed most larvae bodies out of the punctum. We sent all larvae to a parasitologist for analysis and identified them as Cordylobia Anthropophaga (Tumbu fly). We referred the patient to the dressing clinic for proper wound care and instruvted him to apply fusidic acid ointment three times a day for seven days. Two weeks later, the lesions resolved entirely, leaving post-inflammatory hyperpigmentation. We advised the patient to get the Tetanus vaccine as myiasis can be a portal entry for Clostridium Tetani.
Pathology report: Focal hyperkeratosis and parakeratosis with mild spongiosis and acanthosis. Superficial and deep lymphohistiocytic inflammation rich in neutrophils and eosinophils reaching subcutaneous tissue, and we detected parasiti organisms.
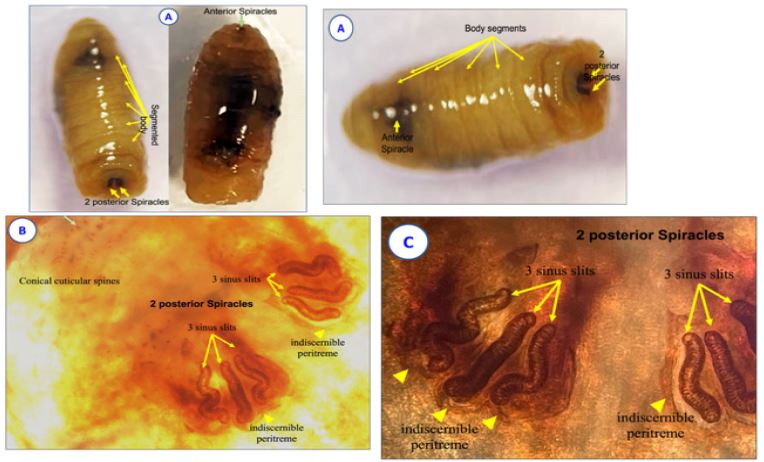
Parasitology report: The extracted larvae were sequentially preserved in alcohol 70%, then ethanol 90% and absolute ethanol (100%), and were microscopically examined. The larvae had characteristic morphological features of Cordylobia (C.) Anthropophaga fly larvae (maggots). Their body was covered with conical cuticular spines pointing posteriorly, as well as anterior respiratory spiracles and two posterior respiratory spiracles (Figure 1A). Each posterior respiratory spiracle had three golden-colored sinuous slits, indiscernible peritreme, and no button (Figure 1B,C]). The magnified slits showed low sinuosity, which differentiates C. anthropophagalarva from C. rodhaini larva (Figure 1B,C).
Discussion
Myiasis is a worldwide infection with seasonal variation correlated with latitude and the life cycle of the numerous fly species [4]. Myiasis is high in the tropics and subtropics of Africa America [5]. There has yet to be a thorough study on its incidence in Saudi Arabia. However, as compared to other reigons of saudi arabia the southern region is more prevalent [6]. Usually, myiasis is a disease that is unpleasant and disgusting to both patients and healthcare providers in most instances. Risk factors include open wounds, immunocompromised individuals, people in low socioeconomic levels, homeless, and drug addicts [1-3]. Patients with furuncular myiasis commonly present with pruritus, skin discomfort, redness, and a sensation of something under the skin crawling [1]. Among these symptoms, our patient had pruritus, pain, and a tingling sensation.
Moreover, the patient has witnessed one of the lesions protruding a material resembling a worm. In some cases, a cutaneous creeping eruption can occasionally exist. We observed that in our patient. If several body sites were involved, the pruritus would be intense so that myiasis would spread in the body. In myasis, physicans usually reach diagnosis clinically. However, a biopsy check can be helpful and supportive [7]. Furuncular myiasis is typically self-limiting [7]. The lesions can initially regress with suffocation with petroleum jelly, bee wax heavy oil, or other poisonous substances such as turpentine oil [4]. We instructed our patient to apply (petroleum gel) over all the nodules to ensure larva suffocation. Then we did larva extraction under local anesthesia with lidocaine injected into the base of the lesion in an attempt to create enough fluid pressure to extrude the larvae out of the punctum.
Conclusion
Myiasis can occur in several parts of Saudi Arabia; however, it is uncommon. Understanding this condition’s epidemiologic trends and diagnostic traits can help avoid long wait times for diagnoses and pointless procedures. To diagnose multiple furuncular myiasis, all types of skin lesions must be carefully examined and a high suspicion level must be maintained. Furthermore, Saudi Arabian medical practitioners must be knowledgeable of furuncular myiasis in order to spot and handle related diseases as quickly as possible.
Declarations
Patient consent: Written informed consent was obtained from the patient for publication and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Author’s contribution: All authors were involved in all steps of preparation of this article. Final proofreading was made by the first author.
Conflict of interest: None to declare.
Financial support and sponsorship: None.
References
- Devi R, Rao N, Sivakumar T, Kalpana G, Jacob E, et al. Case Report of Maggot Infestation on Diabetic Foot Ulcer. Journal of Pharmaceutical Research International. 2021; 194-7.
- Calvopina M, Ortiz-Prado E, Castañeda B, Cueva I, Rodriguez-Hidalgo R, et al. Human myiasis in Ecuador. PLoS Negl Trop Dis. 2020; 14(2): 0007858. Published 2020 Feb 21. doi:10.1371/journal.pntd.0007858.Calvopina M, Ortiz-Prado E, Castañeda B, Cueva I, Rodriguez-Hidalgo R, et al. Human myiasis in Ecuador. PLoS Negl Trop Dis. 2020; 14(2): 0007858. Published 2020 Feb 21. doi:10.1371/journal.pntd.0007858.
- Mutinda KN, Gichohi MP, Maina WR, Maina GS, Agosa KE. Prevalence, Etiology, and Risk Factors Associated with Occurrence of Canine Cutaneous Myiasis in Kitui County, Kenya. Vet Med Int. 2022; 2022: 5699060. doi:10.1155/2022/5699060.
- Francesconi F, Lupi O. Myiasis. Clin Microbiol Rev. 2012; 25(1): 79-105. doi:10.1128/CMR.00010-11.
- Jallow BJJ, Gassara G, Bajinka O, et al. Human myiasis in Sub-Saharan Africa: A systematic review. PLoS Negl Trop Dis. 2024; 18(3): 0012027. doi:10.1371/journal.pntd.0012027.
- Sundharam JA, Al-Gamal MN. Myiasis in Saudi arabia. Ann Saudi Med. 1994; 14(4): 352. doi: 10.5144/0256-4947.1994.352.
- Maxfield L, Crane JS. Cutaneous Larva Migrans. In: StatPearls. Treasure Island (FL): StatPearls Publishing. 2024. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507706/.