
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Papular epidermal nevus with “skyline” basal cell layer: Case report and brief literature review
Isabel Gainza Apraiz1*; Laura Blanch Rius1; Irene Arévalo Ortega1; Jurvist Stee Rodríguez Blandon1; Iria Fernández de la Prieta2; Rosa María Izu Belloso1
1Department of Dermatology, Basurto University Hospital, Bilbao, Spain.
2Department of Anatomic Pathology, Basurto University Hospital, Bilbao, Spain.
*Corresponding Author : Isabel Gainza Apraiz
Department of Dermatology, Basurto University Hospital, Bilbao, Spain.
Email: isabel.gainzaapraiz@osakidetza.eus
Received : Jul 25, 2024
Accepted : Aug 14, 2024
Published : Aug 21, 2024
Archived : www.jcimcr.org
Copyright : © Apraiz IG (2024).
Abstract
Background: Papular Epidermal Nevus with “Skyline” Basal Cell Layer (PENS) is a newly described epidermal nevus characterized by unique clinical and histologic features. While typically sporadic, familial cases and extracutaneous manifestations have been reported.
Case report: We present a case of an infant with small, slightly keratotic, hypopigmented, flat papules distributed across the trunk and lower extremities, which increased in quantity over a 4-year follow-up. The diagnosis was initially uncertain, but a skin biopsy showed histopathological characteristics of PENS, confirming the diagnosis. Additionally, the patient exhibited mild developmental delay.
Discussion: We discuss clinical and histopathological features of PENS, the risk of associated extracutaneous manifestations, and a possible inheritance mechanism for familial cases.
Conclusion: PENS may often go undiagnosed. Therefore, recognizing its presentation and potential associated anomalies is crucial for accurate diagnosis.
Keywords: Epidermal nevus; keratinocytic nevus; Cutaneous mosaicism; Neurocutaneous syndrome.
Citation: Apraiz IG, Rius LB, Ortega IA, Blandon JSR, de La Prieta IF, et al. Papular epidermal nevus with “skyline” basal cell layer: Case report and brief literature review. J Clin Images Med Case Rep. 2024; 5(8): 3217.
Introduction/background
Epidermal nevi are mosaic hamartomatous lesions arising from the epidermis and/or adnexal structures of the skin. There are various types of epidermal nevi, each distinguished by unique clinical and histopathological characteristics. Papular Epidermal Nevus with “Skyline” basal cell layer (PENS) is a recently identified form of keratinocytic nevus [1]. It typically manifests as single or multiple, small, flat papules with a rough, scaly surface that are widely distributed. Lesiones are present at birth and usually do not follow Blaschko’s lines [1-3]. Histologically, PENS exhibits characteristics such as orthokeratotic hyperkeratosis, acanthosis with broad rete ridges, and a basal cell layer featuring a distinct palisaded arrangement of basal cell nuclei resembling the “skyline” pattern seen in Bowen’s disease [1]. Even though it is usually a sporadic condition in otherwise healthy individuals, familial cases [4,5] and association with extracutaneous manifestations have also been documented [2-6].
Case presentation
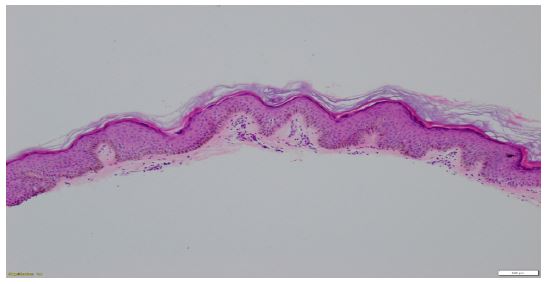
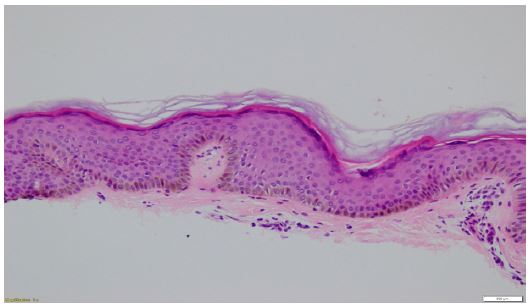
A one-year-old patient was referred to our institution due to small, mildly keratotic, hypopigmented, flat papules scattered in the trunk and lower extremities of unknown duration. Initially, flat warts were suspected, but human papillomavirus polymerase chain reaction testing was repeatedly negative and treatment with topical tea tree oil and 0.05% tretinoin was ineffective. During follow-up, similar lesions appeared, and by the age of four at least 9 papules with similar characteristics were found in various areas including the chest, upper back, lower limbs, buttock, and cheek (Figures 1 and 2). Papular Epidermal Nevus with “Skyline” basal cell layer (PENS) was considered as a possible diagnosis, leading to a skin biopsy that confirmed the condition (Figures 3 and 4). The patient had mild developmental delay including language difficulties and delayed social skills, but was otherwise healthy.


Discussion
In 2011, Torrelo et al. coined the term PENS to describe a specific form of epidermal keratinocytic nevus characterized by small, round to oval, coma-shaped or polygonal, hyperkeratotic flat discrete papules ranging from 1 to 7 mm in size. These papules exhibit unique histopathologic features such as compact orthokeratotic hyperkeratosis, regular acanthosis with broad and rectangular rete ridges, and a basal cell layer displaying a distinctive palisaded arrangement of basal cell nuclei reminiscent of the skyline sign observed in Bowen’s disease [1]. Lesions can range in number from 1 to 18 and do not exhibit a regional predisposition. Typically, they display a random distribution and do not follow any of the known patterns of mosaicism [1], although although a few cases have been reported showing the Blaschkoid distribution commonly seen in keratinocytic nevi [7]. Differential diagnosis comprises common keratinocytic nevi, viral warts, flat warts, and mosaicism of waxy keratoses of childhood (kerinokeratosis papulosa) [2]. Different types of epidermal nevi may appear isolated or in conjunction with different extracutaneous manifestations, primarily neurological, leading to their classification as epidermal nevi syndromes [6]. PENS was initially thought to be an isolated skin defect without dysmorphic features [1]. Nevertheless, in 2012 Tadini et al observed 5 patients with mild neurologic anomalies, including psychomotor delay or epilepsy [4]. This led to the term “PENS syndrome” for cases of PENS associated with extracutaneous features. A review in 2016 highlighted that 42% of reported PENS cases had extracutaneous findings, mainly mild developmental or psychomotor delay. Other described manifestations include epilepsy, dyslexia, attention-deficit/hyperactivity disorder, unique facial features, Achilles tendon shortening, hypospadias, and curved penis. The high prevalence of these extracutaneous features was suggested to be influenced by referral bias [2]. The same literature review evidenced that all individuals with PENS syndrome had more than one lesion, yet not all patients with multiple lesions exhibited extracutaneous manifestations. The study suggests that individuals with four or more lesions have a 6.3 times higher likelihood of developing extracutaneous features, and therefore recommends that patients with more than four PENS lesions should be referred to a neuropediatrician to exclude mild neurologic delay [2]. In the literature, most described cases of PENS have been sporadic, but a few familial cases have been documented [4,5]. In these instances, paradominant inheritance has been suggested to explain how traits that typically appear sporadically can occasionally be transmitted. In paradominant inheritance, heterozygous individuals for a mutation may be asymptomatic but can transmit the mutation to their offspring. If an early postzygotic somatic mutation affects the corresponding wild-type allele, leading to a loss of heterozygosity, the trait can become manifest. Affected tissues then result from cell clones that are either homozygous or hemizygous for the mutation in a mosaic pattern. In rare cases where postzygotic loss of heterozygosity occurs in several family members, familial aggregation of the condition may be observed [5].
Conclusion
PENS is a newly described entity that might be underdiagnosed. It is essential to be familiar with its clinical and histopathologic features to accurately diagnose and differentiate it from other conditions. It is also crucial to bear in mind and rule out associated extracutaneous anomalies, mainly neurological.
Competing interests: The authors declare that they have no competing interests.
References
- Torrelo A, Colmenero I, Kristal L, Navarro L, Hafner C, et al. Papular epidermal nevus with skyline basal cell layer (PENS). J Am Acad Dermatol. 2011; 64 (5): 888-92.
- Luna PC, Pannizardi AA, Martin CI, Vigovich F, Casas JG, et al. Papular Epidermal Nevus with Skyline Basal Cell Layer (PENS): Three New Cases and Review of the Literature. Pediatr Dermatol. 2016; 33(3): 296-300.
- Pardo Domínguez C, Del Boz González J, Fúnez Liébana R. Papular epidermal nevus with skyline: 3 nuevos casos. Actas Dermosifiliogr. 2020; 111 (2): 185-7.
- Tadini G, Restano L, Happle R, Itin P. PENS Syndrome: A New Neurocutaneous Phenotype. Dermatology. 2012; 224(1): 24-30.
- Brena M, Besagni F, Boneschi V, Tadini G. Familial Papular Epidermal Nevus with Skyline Basal Cell Layer. Pediatr Dermatol. 2014; 31(1): 33-5.
- Rodríguez-Díaz E, Gonzalvo P, Colmenero I, Requena L, Hernández-Martín A, et al. Papular Epidermal Nevus with Skyline Basal Cell Layer (PENS) with Extracutaneous Findings. Pediatr Dermatol. 2013; 30(4): 54-6.
- Faure E, Tadini G, Brena M, Cassulini LR. Papular epidermal nevus with skyline basal cell layer (PENS) following a blaschko linear pattern. Pediatr Dermatol. 2013; 30(6): 270-271.