
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Epidermoid cyst of base of the tongue in an infant: A rare entity
Arunabha Chakravarti*; Oshin Guleria; Vishnudas TV; Akhil Bahuguna; Pooja Abbey
Department of Otorhinolaryngology - Head and Neck surgery, Lady Hardinge Medical College, New Delhi, India.
*Corresponding Author : Arunabha Chakravarti
Department of Otorhinolaryngology - Head and Neck surgery, Lady Hardinge Medical College, New Delhi, India.
Tel: 9868093035;
Email: drachakravarti@yahoo.co.in
Received : Aug 02, 2024
Accepted : Aug 16, 2024
Published : Aug 23, 2024
Archived : www.jcimcr.org
Copyright : © Chakravarti A (2024).
Abstract
Introduction: Stridor is often a symptom exhibited by pediatric age group patients which signifies an underlying pathology of the airway. The major causes of stridor in an infant include laryngomalacia, laryngotracheobronchitis subglottic stenosis, and vocal cord palsy. However, relatively less common causes include epidermoid cyst, laryngeal papillomatosis, and bacterial tracheitis.
Case presentation: Here we report a case of epidermoid cyst of the base of the tongue in a 6 month old female child which went undiagnosed till 6 month after birth. Simple examination methods like depressing the tongue with a tongue depressor and finger palpation of the base of the tongue could have led to an early diagnosis and avoided morbidity for the child and anxiety for the caregiver. Elective tracheostomy with transoral excision of the cyst with powered instruments was performed and after significant multidisciplinary postoperative efforts, the child was discharged in a stable condition.
Conclusion: There should be a high index of suspicion of oropharyngeal masses as a possible cause of persistent stridor and failure to thrive, like epidermoid cyst, vallecular cyst, lingual thyroid.
Keywords: Pediatric stridor; Epidermoid cyst; Epidermoid cyst of oral cavity; Microdebrider.
Abbreviations: USG: Ultrasound; MRI: Magnetic Resonance Imaging.
Citation: Chakravarti A, Guleria O, Vishnudas TV, Bahuguna A, Abbey P. Epidermoid cyst of base of the tongue in an infant: A rare entity. J Clin Images Med Case Rep. 2024; 5(8): 3221.
Background
Stridor is defined as a high pitch noise that arises from compromised airway at the level of the larynx and trachea [1]. In the pediatric age group, it is a distressing scenario for the caregivers. The spectrum of conditions causing stridor can range from benign pathologies like laryngomalacia to potentially fatal conditions like foreign body aspiration and subglottic stenosis. The major causes of stridor in an infant include laryngomalacia, laryngotracheobronchitis subglottic stenosis, and vocal cord palsy [1,2]. Epidermoid cyst of the oral cavity is a relatively rare cause of stridor. Epidermoid cyst is a type of teratoma and it constitutes 15-35% of all teratomas [3]. Tongue is a rare location, as only 13 cases of epidermoid cyst of the body of the tongue have been reported in English literature [4]. They present with inspiratory stridor, and often intermittent attacks of complete respiratory obstruction with cyanosis. Feeding problems, including regurgitation, dysphagia, and inability to suck accompany. Weight loss or failure to gain at a normal rate is usually seen. Obstructive sleep apnoea has been reported to occur due to these cysts [5].
Immediate diagnosis and prompt measures need to be taken as such lesions may be life threatening in infants. In this particular case, the child was undiagnosed till 6 months of age causing severe failure to thrive.
Case presentation
ChA six month old female child presented to hospital with chief complaints of noisy breathing and cough since 5 months. The difficulty in breathing was progressive, aggravated on sleeping and feeding, and not relieved on proning, associated with breath holding spells, poor oral acceptance and regurgitation of feeds. The child was not gaining weight and had failure to thrive.
The child was previously admitted twice in other hospitals and was treated as a case of pneumonia, but the child did not attain any relief in symptoms.
On examination, the child had inspiratory stridor. Subcostal and intercostal retractions were present. Weight of the child was 3 kg and looked emaciated (Figure 1). Respiratory rate was 38 min, with use of accessory muscles and peripheral cyanosis. SpO2 on room air was 86%, On depressing the tongue, a cystic swelling approximately 3 x 3 cm seemed to be arising from the base of tongue obliterating whole of the oral cavity. Distal extent of the tumor could not be visualised.
Laryngeal USG revealed round to oval 28 mm x 32 mm well defined iso-hypoechoic lesion arising from the base of the tongue. Thyroid gland was normal in position (Figure 2).
An MRI scan, although ideal for evaluation of the mass, could not be performed as it was very risky in this case because it could precipitate apnoea upon sedating the child.
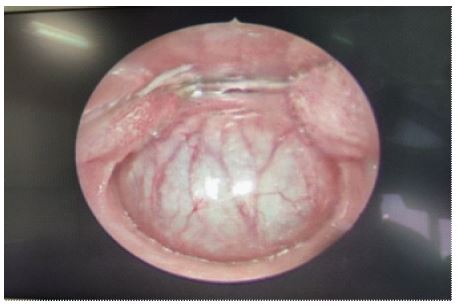
Endotracheal intubation was not possible hence an elective tracheostomy followed by transoral microdebrider assisted excision of the cyst was performed under general anesthesia using direct laryngoscopic visualisation. Figure 3 shows the intraoperative endoscopic picture of the lesion. Part of the cyst wall sent for histopathology, which was suggestive of epidermoid cyst. Figure 4 shows the laryngoscopic view post-excision of the cyst.
Postoperatively, the patient was shifted to pediatric intensive care unit in view of need of mechanical ventilation due to underlying poor chest condition. Finally, the child could be weaned off the ventilatory support after 15 days and was shifted back to ENT ward.
The child was successfully decannulated after 6 days. Oral feeds were started which were well tolerated by the child. She was maintaining O2 saturation on room air. The child was discharged in stable condition and is on regular follow up with no fresh complaints (Figure 5).




Discussion
Epidermoid cyst of the oropharyngeal region is an extremely rare cause of stridor. An oral epidermoid cyst can be congenital or acquired [5]. The congenital type arises due to failure of surface ectoderm to separate from underlying neural tube, or from invagination of the surface ectoderm along the embryonic fusion sites during embryonic stage [3]. The acquired type is a result of trauma causing implantation of surface epithelial element into deeper tissue [3]. Both the varieties are similar histologically and clinically [6]. Histologically, epidermoid cysts are lined by keratinized squamous epithelium, whereas dermoid cyst has additional skin appendages [5]. They are mostly found in the submental and sublingual region along the midline and have a predilection for the floor of the mouth [5,6].
Clinically the differential diagnoses to be considered in a lesion at the base of the tongue in the pediatric age group are dermoid cyst, vallecular cyst, lingual thyroid and thyroglossal duct cyst. Lingual thyroid may present as a mass at the base of tongue, and imaging is required to confirm a normally situated thyroid gland. Thyroid scan carries a risk of radiation exposure which can have long term side effects in the pediatric population, and. In this case, the presence of a normally placed thyroid gland was a reassuring feature from surgeon’s point of view. All of the above lesions have similar presentations, which depends on the size of the lesion and the extent of obstruction caused by it.
The condition can usually be diagnosed by visual examination with the aid of a tongue depressor, or by palpation of the cyst with the finger. Direct laryngoscopy may be used to confirm the diagnosis. Ultrasonography is non invasive and easy to perform and both otolaryngologists and pediatricians are well versed with it. It provides a distinction between solid and cystic masses and can also confirm the presence of a normal thyroid gland [8,9]. Although MRI is the modality of choice for complete evaluation of the lesion,it requires sedation and careful airway management in infants. Histopathology remains the cornerstone for definitive diagnosis. Definitive management includes excision or marsupialisation of the cyst, which relieves the symptoms due to obstruction. Simple aspiration of the cyst carries a high risk of recurrence [10].
There should be a high index of suspicion of oropharyngeal masses as a possible cause of persistent stridor and failure to thrive, like epidermoid cyst, vallecular cyst, lingual thyroid. A otolaryngological referral should always be sought for early diagnosis and management.
Declarations
Ethics approval and consent to participate: Ethics approval is not applicable for the case report.
Consent for publication: Written informed consent was obtained from the patient’s parents for publication of this case report and accompanying images.
Source of support: Not applicable.
Acknowledgments: We would like to thanks the PICU team who managed the child in post operative period. We would also like to thank the OT staff for their support in managing the case.
Conflict of interests: The authors declare that they have no conflict of interests.
Authors contribution: The manuscript has been read and approved by all the authors, that the requirements for authorship as stated earlier in this document have been met, and that each author believes that the manuscript represents honest work.
References
- Patnaik S, Zacharias G, Jain MK, Samantaray KK, Surapaneni SP. Etiology, Clinical Profile, Evaluation, and Management of Stridor in Children. Indian J Pediatr. 2021; 88(11): 1115-1120. doi:10.1007/s12098-021-03722-8.
- Gilbert EG, Russell KE, Deskin RW. Stridor in the infant and child. Assessment, treatment. AORN J. 1993; 58(1).
- Shaari CM, Ho BT, Shah K, Biller HF. Lingual dermoid cyst. Otolaryngol Head Neck Surg. 1995; 112(3): 476-478. doi:10.1016/S0194-59989570289-X.
- Corrêa MS, Fonoff Rde N, Ruschel HC, Parizotto SP, Corrêa FN. Lingual epidermoid cyst: Case report in an infant. Pediatr Dent. 2003; 25(6): 591-593.
- Smirniotopoulos JG, Chiechi MV. Teratomas, dermoids, and epidermoids of the head and neck. Radiographics. 1995; 15(6): 1437-1455. doi:10.1148/radiographics.15.6.8577967.
- Chaurasia A, Goel D. Epidermal Inclusion Cyst of Tongue-A Case Report. J Oral Med Oral Surg Oral Pathol Oral Radiol 2015; 1(4): 171-175. doi: 10.5958/2395-6194.2015.00004.1.
- Ueno T, Takayama R, Osada SI, Saeki H. Epidermoid Cyst Arising on the Body of the Tongue: Case Report and Literature Review. J Nippon Med Sch. 2018; 85(6): 343-346. doi:10.1272/jnms.JNMS.2018_85-56.
- Ahrens B, Lammert I, Schmitt M, Wahn U, Paul K, et al. Life-threatening vallecular cyst in a 3-month-old infant: Case report and literature review. Clin Pediatr (Phila). 2004; 43(3): 287-290. doi:10.1177/000992280404300312.
- Breysem L, Goosens V, Vander Poorten V, Vanhole C, Proesmans M, et al. Vallecular cyst as a cause of congenital stridor: report of five patients. Pediatr Radiol. 2009; 39(8): 828-831. doi:10.1007/s00247-009-1299-1.
- Tibesar RJ, Thompson DM. Apnea spells in an infant with vallecular cyst. Ann Otol Rhinol Laryngol. 2003; 112(9 Pt 1): 821-824. doi:10.1177/000348940311200914.