
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
A rare case of c3, c4 bilateral cervical rib in pediatrics male patient: A case report
*Corresponding Author : Solomon Bishaw
Jugol Hospital, Harar, Harari Region, Ethiopia.
Email: bishawsolomon6@gmail.com
Received : Aug 02, 2024
Accepted : Aug 20, 2024
Published : Aug 27, 2024
Archived : www.jcimcr.org
Copyright : © Bishaw S (2024).
Abstract
Background: Cervical rib is an anomalous rib which arises from the seventh cervical vertebra. However, it may also arise from the fourth, fifth or sixth cervical vertebra.
Case presentation: A 13 years old male patient present with right side neck pain and unable to extend to left side after being stroked by stick on the right side. On physical examination he has right lateral neck tenderness, otherwise no pertinent finding.
Conclusion: Even though cervical rib is common at c7 they can be seen in the proximal vertebral body (c3, c4) and they can be multiple like our case.
Keywords: Cervical rib; C3; C4 rib.
Citation: Bishaw S. A rare case of c3, c4 bilateral cervical rib in pediatrics male patient: A case report. J Clin Images Med Case Rep. 2024; 5(8): 3224.
Introduction
The cervical rib is described as an anomalous, supernumerary, extra, or additional rib which commonly arises from the seventh cervical vertebra but it may arise from fourth, fifth or sixth cervical vertebra [1,2]. Its incidence is estimated to be 0.2% and 8%, and it is more common in women. It can be unilateral or bilateral with poor right predominance when they are unilateral. Majority of the cases tend to be asymptomatic, and usually diagnosed accidentally when a plain X-ray of the chest or cervical spine is performed for an unrelated different reason [3]. The diagnostic tools for identifying the cervical rib are chest X-ray and X-ray of cervical region (neck). Other imaging techniques like MRI scan or CT scan can also help [4]. Treatment is usually conservative with rehabilitation, except when symptoms occur caused by nerve (brachial plexus) or vascular (subclavian artery) compression, when the surgical option is taken [3].
Clinical case
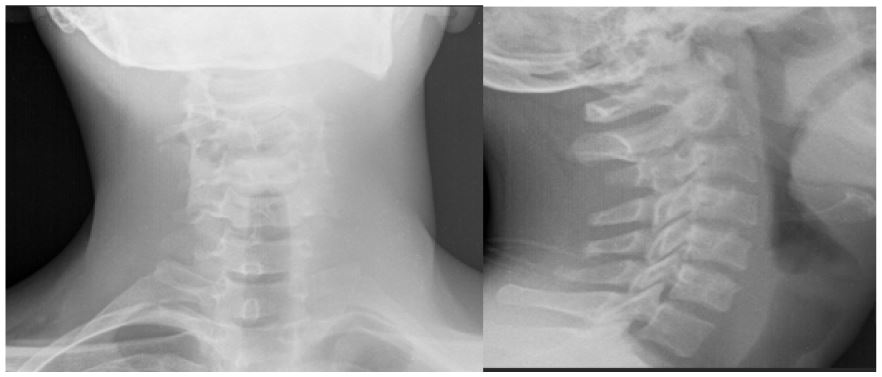
Informed consent was obtained from the patient for inclusion in this case report. A 13 years old male patient present with right side neck pain and unable to extend to left side after hit by stick on the right side. On physical examination he has tenderness on the right lateral neck otherwise no bruse, or swelling. Motor examination is unremarkable Laboratory examinations are all in normal range. PA and lateral neck X-ray was taken and showed bilateral cervical rib originating from the cervical vertebral body of C3 and C4 in lateral and caudal direction.
Discussion
The skeletal system arises from the paraxial mesoderm. The paraxial mesoderm located on either side of the neural tube forms somites. The mesenchymal cells of the somites differentiate into a ventral part, the sclerotome, and a dorsal part, the dermatome. At the end of the fourth week of embryogenesis, the cells of the sclerotome convert into mesenchymal cells and then into ribs [1]. It has been hypothesized Hox genes are responsible for patterning of the axial skeleton, and Mutations in hox genes mediate the abnormal development of cervical ribs [1,2]. The reported cervical rib prevalence is controversial and it varies depending on the population. Radiograph images indicate that the prevalence of cervical ribs is below 1% in the general population; however, studies have found its occurrence to vary significantly from 0.58% to 6.2% depending on the population are twice as common in females. It is present bilaterally in 47-73% of the cases but often the two sides are asymmetrical. When unilateral, it is generally on the right side. On postmortem studies, the incidence was 1% [2-6].
There are different type of classification of cervical rib based on their composition and articulation The cervical rib may be composed of bone completely (complete cervical rib) or may be incomplete with a short bony part and a fibrous or fibro muscular band extending from the bony part (incomplete cervical rib). There are two types of cervical ribs: those which are complete and articulate with the first rib and those which are incomplete and end freely in the soft tissues of the neck [6].
In 1869 [1], Gruber proposed a classification of cervical rib based on the amount of bone present and the thickness of the rib-like structure which was later modified by Blanchard [7]. This classification is divided into five types:
Type 1: Complete cervical rib attached to the sternum.
Type 2: Cartilage of the cervical rib is attached to cartilage of the first rib.
Type 3: The two extremities of the ribs are developed as bone structures, but the intermediate portion is a fibrous cord.
Type 4: The two extremities are developed but not united by a fibrous cord.
Type 5: The cervical rib is represented by a segment attached to the vertebrae, no anterior extremity exists.
Symptomatology and complications. The presence of cervical ribs is usually asymptomatic (90% of patients) and does not require their removal. Factors like trauma, overuse, poor posture, or the presence of large breasts predispose to symptoms. The symptoms are more prevalent in incomplete cervical ribs, compared to the complete ones. Pressure upon the brachial plexus and the subclavian artery and vein cause the symptoms. Only 5-10% of people with cervical ribs have symptoms. If they cause symptoms, this usually occurs after middle age [6,8]. If symptomatic, cervical ribs have numerous clinical implications, although they can be generally regarded as either neurological or vascular. It is commonly known that incomplete ribs only affect the brachial plexus, whereas complete ribs also have an impact on the subclavian artery [1].
Treatment is usually conservative with rehabilitation, except when symptoms occur caused by nerve (brachial plexus) or vascular (subclavian artery) compression, when the surgical option is taken [3,9].
Conclusion
Even though cervical rib is common at c7 they can be seen in the proximal vertebral body (c3, c4) and they can be multiple like our case.
Declarations
Ethics statement: Informed consent was obtained from the patient for inclusion in the case report.
Consent for publication: Written informed consent has been obtained from the patient to publish this manuscript and all of accompanying images.
Disclosure: The authors declare that there are no conflicts of interest in this work.
References
- Spadli AN, Cecot T, Majos A, N LS, Pietruszewska W, et al. The Epidemiological, Morphological, and Clinical Aspects of the Cervical Ribs in Humans. 2016.
- Agarwal S, Choudhury PR, Baro A. Cervical ribs: A study on radiographs in a tertiary care. 2018
- Aulestia NP, Montero SR, Luisa M, Feijoo V. Images in Clinical Rheumatology Double Cervical Rib : A Case Report Doble costilla cervical : a propósito de un caso. 2019; 15(6): 370-1.
- Iqbal K, Asif S. A Radiological Study on Cervical Rib and Associated Chest Wall Anomalies ORIGINAL ARTICLE A Radiological Study on Cervical Rib and Associated Chest Wall Anomalies. 2022.
- Subhi M Al, Aswami H Al. Prevalence of cervical ribs and elongated transverse processes in Omani population: A computed tomography-based study. 2022; 1-9.
- Different_Family_Functioning_Perceptions.pdf.
- Cu N, Ec I, Rt E, Cv O. Thoracic Outlet Syndrome from Bilateral Cervical Ribs -A Clinical Case Report. 2018; 8(2): 78-80.
- Urschel HC, Kourlis H. Thoracic Outlet Syndrome: A 50-Year Experience at Baylor University Medical Center. Baylor Univ Med Cent Proc. 2007; 20(2):125-35.
- Povlsen B, Hansson T, Povlsen SD. Treatment for thoracic outlet syndrome. Cochrane Database Syst Rev. 2014; 2014(11).