Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Endoscopy from the inside out
Tobias Schlosser1*; Jan Tünnemann2; Albrecht Hoffmeister2
1Department of Oncology, Gastroenterology, Hepatology, Pneumology & Infectious, University Medical Center, Leipzig, Germany.
2Division of Gastroenterology and Diseases, University Medical Center, Leipzig, Germany.
*Corresponding Author : Tobias Schlosser
Department of Oncology, Gastroenterology,
Hepatology, Pneumology & Infectious, University
Medical Center, Leipzig, Germany.
Email: as.schlosser@medizin.uni-leipzig.de
Received : Dec 15, 2020
Accepted : Dec 30, 2020
Published : Dec 31, 2020
Archived : www.jcimcr.org
Copyright : © Marinova (2024).
Citation: Schlosser T, Tünnemann J, Hoffmeister A. Endoscopy from the inside out. J Clin Images Med Case Rep. 2024; 5(8): 3225.
Introduction
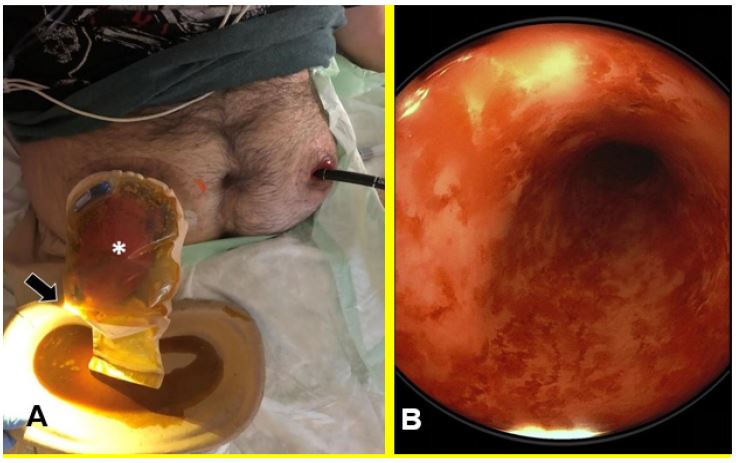
A 31-year-old patient with Crohn’s disease presented for endoscopy three years after surgical repair of an ileocecal conglomerate tumor and a left-sided enterocutaneous fistula with lower abdominal abscesses. In addition to ileocecal resection with necessity of an anastomotic stoma of the ileum (right upper abdomen) back then, a sigmoid resection was additionally needed, so that a descendostomy of the colon was also created as a mucous fistula (left middle abdomen). Before the planned repositioning of the now prolapsed ileostomy (Figure 1A,*), endoscopy was performed to evaluate the distal sections of the colon. For this purpose, retrograde endoscopy was performed via distal descendostomy. Due to the lack of luminal absorption of fatty acids, the mucosa showed inflammatory changes in the form of diversion colitis (Figure 1B). The tip of the standard colonoscope (Figure 1A,↑) reappears after retrograde passage of the bypassed transverse colon. The patient is currently awaiting full restoration of the intestinal tract’s continuity.
Conflict of interest: None of the authors has any potential conflict of interest related to this manuscript.