
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Management of acute onset stridor caused by thyroid lymphoma: A case report and review of literature
Arunabha Chakravarti1; Vishnudas TV2*; Oshin Guleria3; Akhil Bahuguna3; Shilpi Aggarwal4
1Director Professor & Head of Department, Department of ENT & Head and Neck surgery, Lady Hardinge Medical College, New Delhi, India.
2Senior Resident, Department of ENT & Head and Neck surgery, Lady Hardinge Medical College, New Delhi, India.
3Junior Resident, Department of ENT & Head and Neck surgery, Lady Hardinge Medical College, New Delhi, India.
4Director Professor, Department of Pathology, Lady Hardinge Medical College, New Delhi, India.
*Corresponding Author : Vishnudas TV
Senior Resident, Department of ENT & Head and
Neck surgery, Lady Hardinge Medical College, New
Delhi, India.
Email: vishnudas57@gmail.com
Received : Jul 22, 2024
Accepted : Aug 26, 2024
Published : Sep 02, 2024
Archived : www.jcimcr.org
Copyright : © Vishnudas TV (2024).
Citation: Chakravarti A, Vishnudas TV, Guleria O, Bahuguna A, Aggarwal A. Management of acute onset stridor caused by thyroid lymphoma: A case report and review of literature. J Clin Images Med Case Rep. 2024; 5(9): 3235.
Abstract
Thyroid lymphoma is a rare malignancy that can present with acute airway compromise, posing a diagnostic and therapeutic challenge. Though it usually presents as a rapidly enlarging neck mass, patients can also manifest with pressure symptoms like stridor, dysphagia or hoarseness. We present a case of a patient with thyroid lymphoma presenting as acute onset stridor, highlighting the importance of prompt recognition and management. This case report discusses the clinical presentation, diagnostic workup, and multidisciplinary approach to the management of thyroid lymphoma causing airway obstruction along with review of various literature.
Background
Thyroid lymphoma is an uncommon neoplasm, accounting for approximately 2-5% of all thyroid malignancies [1]. It most commonly occurs in the 7th decade of life [2]. Though it usually presents as a rapidly enlarging neck mass, patients can also manifest with pressure symptoms like stridor, dysphagia or hoarseness. Acute airway compromise due to thyroid lymphoma is a rare but potentially life-threatening presentation. 30-60% of patients present in euthyroid state [3]. Herein, we de- scribe a case of thyroid lymphoma presenting with acute onset stridor and discuss the diagnostic and therapeutic challenges associated with this condition.
Case Presentation
A 62-year-old female presented to the ENT emergency with acute onset stridor and dyspnea. Physical examination revealed a midline firm neck swelling with mild tenderness. Another firm and non-tender swelling of dimensions 3 x 4 cm was present in the right level posterior triangle (Figure 1). Trachea was not palpable. Urgent flexible laryngoscopy demonstrated adequate glottic chink but significant tracheal narrowing.
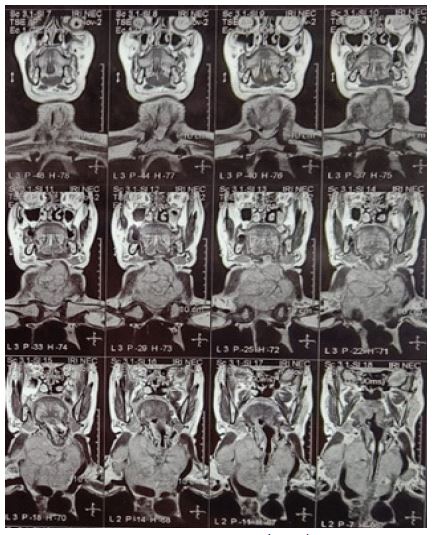
Magnetic Resonance Imaging (MRI) of the neck revealed a large lobulated high T2 signal intensity mass lesion in midline neck with ICA encasement with the thyroid gland inseparable from the mass with infiltration of the trachea (FIgure 2). Fine- Needle Aspiration Cytology (FNAC) of the thyroid mass gave the diagnosis of diffuse large B-cell lymphoma. FNAC of the right lateral neck swelling revealed it to be a metastatic lymph node.
An FDG PET scan was done following this which revealed, a large metabolically active lobulated heterogeneously enhancing soft tissue mass involving both lobes of the thyroid gland and isthmus and encasing the trachea. There was no other metabolically active areas anywhere in the body in the PET scan.
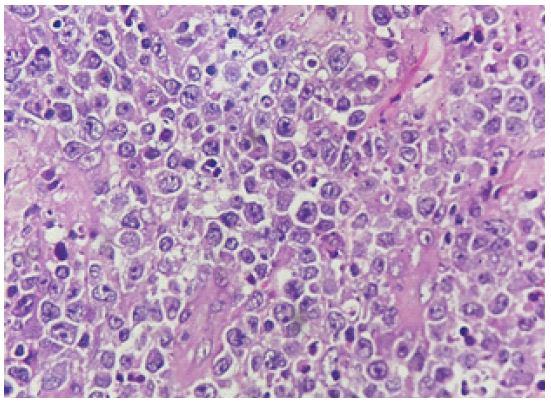
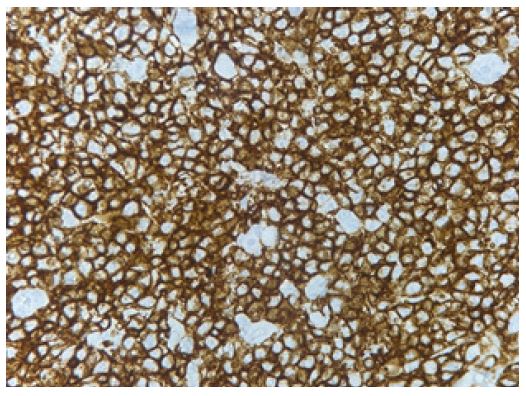
Hence the patient was provisionally diagnosed with thyroid lymphoma Ann Arbor stage IIE. The patient was promptly initiated on corticosteroids for airway management. A biopsy specimen was obtained under local anesthesia and sent for histopathological examination with immunohistochemistry which reported as Diffuse B-cell lymphoma (DLBCL) (Figures 3,4).
Multidisciplinary consultation with otolaryngology, hematology/oncology, and radiation oncology guided subsequent treatment decisions. The patient underwent 6 cycles of chemotherapy under the R-CHOP regimen (A regimen consisting of cyclophosphamide, doxorubicin, prednisone, rituximab and vincristine). Serial imaging and clinical follow-up demonstrated sustained remission.

Discussion and conclusion
The head and neck region is a favourable site for lymphomas owing to the vast amount of lymphoid tissues [4]. WHO classifies lymphomas based on genetic and immunohistochemical criteria into Hodgkin’s lymphoma (HL) and non-Hodgkin’s lymphoma (NHL). The occurrence of a primary thyroid lymphoma(PTL), a lymphoma occurring in the thyroid gland alone, is almost 5% [5] and it accounts for 3% for all the Non-Hodgkin lymphomas [1]. Females have a higher preponderance with a male: female ratio of 1:4 [2]. Though the risk factors associated with PTL have been attributed to various etiologies including auto-immune disorders, chronic antigen stimulation etc., the highest risk is associated with Hashimoto’s thyroiditis [6]. Our patient was an elderly female who presented with neck swelling and stridor.
PTL is again divided into diffuse B-cell lymphoma and mixed subtypes and pure MALT lymphomas. DLBCL accounts for 70% of all PTL and follows a more rapid course. They hold a 5-year survival rate of 90% with the use of multimodal therapies [7,8].
The definitive diagnosis of PTL is obtained by histological analysis of tissue. Ultrasonography is the imaging modality of choice and can typically show one of three patterns: nodular, diffuse, or mixed [9]. When presenting as a solitary mass, the radiological appearance can resemble that of anaplastic thyroid carcinoma but can be distinguished by its homogenous appearance as well as the lack of calcification, necrosis, and cystic degeneration within the nodule. Magnetic resonance imaging may be more sensitive than computed tomography in the detection of extrathyroidal involvement. Fluorine-18-fluorodeoxyglucose positron emission tomography (FDG-PET) can be useful in staging and restaging or in assessing response to treatment in PTL [10]. We performed an MRI scan together with PET scan to delineate the tumour and to cement the diagnosis.
Fine Needle Aspiration Cytology (FNAC) is the initial technique of choice for pathological assessment of a thyroid lesion. Generally for lymphoma, which may be extrapolated to PTL, Swart et al. found that the addition of flow cytometry to FNAC analysis produced sensitivity of 97% and specificity of 87% for the detection of B-cell lymphoma [11]. In our patient, the FNAC report suggested lymphoma but a histopathological examination was advised for further sub-typing through immunohistochemistry.
A definitive role remains for an open surgical biopsy to allow for definitive subtyping, especially in the diagnosis of MALT lymphomas.
The management of DLBCL is multimodal because of the typically aggressive clinical course and uses a combination of the monoclonal antibody rituximab, chemotherapy (a combination of cyclophosphamide, doxorubicin, vincristine, and prednisone [CHOP]), and radiotherapy. Our patient received 6 cycles of chemotherapy under the R-CHOP regimen and had shown good remission. Conversely, MALT lymphomas may be amenable to single-modality treatment because of the indolent nature of the disease. Surgery has a very limited role in the management of PTL but may be indicated in the urgent management of the airway. Multidisciplinary collaboration among various specialties is crucial for optimizing patient outcomes.
Thyroid lymphoma should be considered in the differential diagnosis of patients presenting with acute onset stridor and thyroid enlargement. A systematic approach to diagnosis and management, involving collaboration among multiple specialties, is essential for achieving favourable outcomes in these challenging cases.
References
- Walsh S, Lowery AJ, Evoy D, McDermott EW, Prichard RS. Thyroid Lymphoma: Recent Advances in Diagnosis and Optimal Management Strategies. The Oncologist. 2013; 18(9): 994-1003.
- Pedersen RK, Pedersen NT. Primary non-Hodgkin’s lymphoma of the thyroid gland: A population based study. Histopathology. 1996; 28(1): 25-32.
- Thieblemont C, Mayer A, Dumontet C, Barbier Y, Callet-Bauchu E, et al. Primary thyroid lymphoma is a heterogeneous disease. J Clin Endocrinol Metab. 2002; 87(1): 105-11.
- Etemad-Moghadam S, Tirgary F, Keshavarz S, Alaeddini M. Head and neck non-Hodgkin’s lymphoma: A 20-year demographic study of 381 cases. Int J Oral Maxillofac Surg. 2010; 39(9): 869-72.
- Ansell SM, Grant CS, Habermann TM. Primary thyroid lymphoma. Semin Oncol. 1999; 26(3): 316-23.
- Holm LE, Blomgren H, Löwhagen T. Cancer risks in patients with chronic lymphocytic thyroiditis. N Engl J Med. 1985; 312(10): 601-4.
- Graff-Baker A, Roman SA, Thomas DC, Udelsman R, Sosa JA. Prognosis of primary thyroid lymphoma: Demographic, clinical, and pathologic predictors of survival in 1,408 cases. Surgery. 2009; 146(6): 1105-15.
- Niitsu N, Okamoto M, Nakamura N, Nakamine H, Bessho M, et al. Clinicopathologic correlations of stage IE/IIE primary thyroid diffuse large B-cell lymphoma. Ann Oncol off J Eur Soc Med On- col. 2007; 18(7): 1203-8.
- Mounier N, Briere J, Gisselbrecht C, Emile JF, Lederlin P, et al. Rituximab plus CHOP (R-CHOP) overcomes bcl-2--associated re- sistance to chemotherapy in elderly patients with Diffuse Large B-Cell Lymphoma (DLBCL). Blood. 2003; 101(11): 4279-84.
- Karlin L, Coiffier B. Improving survival and preventing recurrence of diffuse large B-cell lymphoma in younger patients: Current strategies and future directions. OncoTargets Ther. 2013; 6: 289- 96.
- Swart GJ, Wright C, Brundyn K, Mansvelt E, du Plessis M, ten Oever D, et al. Fine needle aspiration biopsy and flow cytometry in the diagnosis of lymphoma. Transfus Apher Sci off J World Apher Assoc off J Eur Soc Haemapheresis. 2007; 37(1): 71-9.