
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Behind the red curtain: The real face of panscleritis
Diksha1; Priyanka Arora2*; Ritesh Verma2; Gurvinder Kaur3
1Junior Resident, Department of Ophthalmology, Dayanand Medical College and Hospital, Ludhiana, Punjab, India.
2Associate Professor, Department of Ophthalmology, Dayanand Medical College and Hospital, Ludhiana, Punjab, India.
3Professor and Head, Department of Ophthalmology, Dayanand Medical College and Hospital, Ludhiana, Punjab, India.
*Corresponding Author : Priyanka Arora
Associate Professor, Department of Ophthalmology,
Dayanand Medical College and Hospital, Ludhiana,
Punjab, India.
Tel: 9781162639;
Email: priyankagalhotra@gmail.com
Received : Aug 01, 2024
Accepted : Aug 27, 2024
Published : Sep 03, 2024
Archived : www.jcimcr.org
Copyright : © Arora P (2024).
Abstract
Scleritis is a painful, sight-threatening, inflammatory condition of the sclera often presenting with an acute red and painful eye and potential decreased visual acuity. Inflammation of the periorbital soft tissues and ophthalmoplegia are not typically associated with posterior scleritis. We present a comprehensive visual documentation of a diagnostically challenging case of panscleritis.
Keywords: Panscleritis; B-Scan; CT Scan; Choroidal folds.
Citation: Diksha, Arora P, Verma R, Kaur G. Behind the red curtain: The real face of panscleritis. J Clin Images Med Case Rep. 2024; 5(9): 3236.
Introduction
Scleritis is a rare, vision-threatening inflammation of the sclera that is often associated with life-threatening systemic illnesses. Posterior scleritis is often not diagnosed or missed due to its subtle clinical signs and protean manifestations [1].
Case
55-year-old female presented with acute left eye pain, left-sided headache, and sudden vision loss. Best-corrected visual acuity was 6/9 in the right eye and 3/60 in the left eye. Intraocular pressure was 30 mmHg in the left eye. Anterior chamber showed 1+ reactions and extraocular movements were restricted in all gazes.
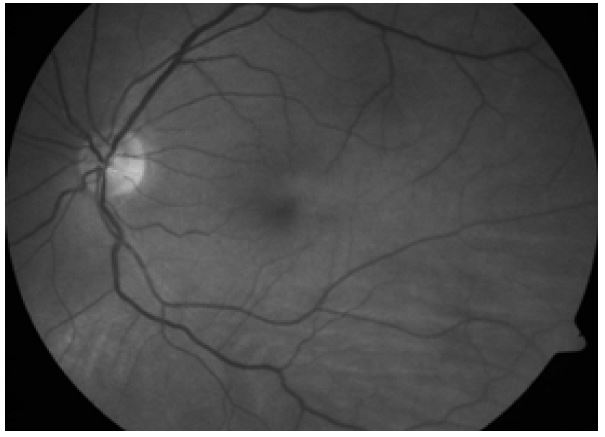
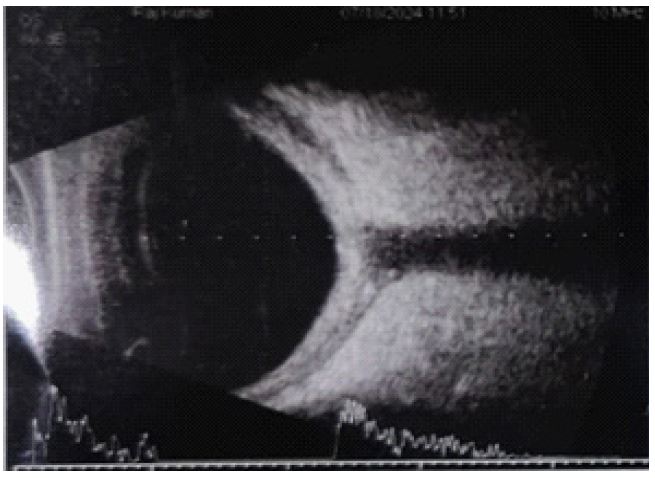
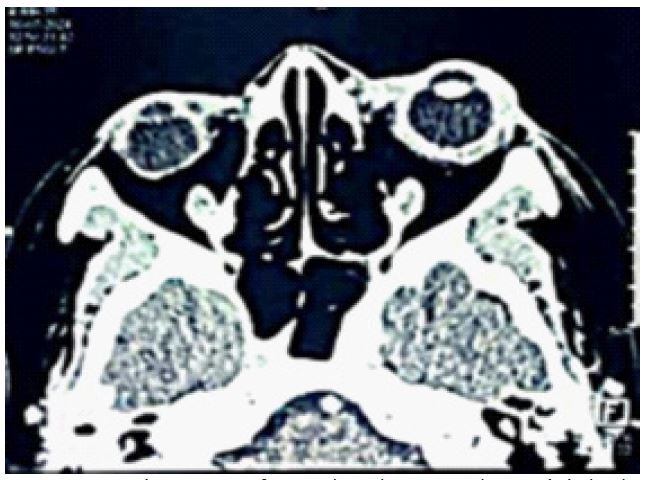
We provide a comprehensive visual documentation, including slit lamp images demonstrating diffuse conjunctival congestion and chemosis (Figure 1), fundus photographs showing choroidal folds (Figure 2). B-scan ultrasound revealing the characteristic T sign (Figure 3) and CT scan indicating increased choroidal thickness (Figure 4).
Discussion
These diagnostic images underscore the complexity and severity of panscleritis, highlighting the need for thorough ocular examination and imaging in ambiguous cases. This case emphasizes the diagnostic challenges posed by panscleritis and the critical importance of accurate differentiation from other periorbital inflammatory conditions. Effective management, often requiring systemic therapy in the form of Oral non-steroidals can be effective with various appropriate regimens, such as ibuprofen 600 to 800 mg q.i.d.,. In cases unresponsive to oral NSAIDs, high-dose systemic corticosteroids are often used, with typical doses of 1 mg/kg/day or approximately 60 mg of prednisone daily, is crucial to prevent irreversible vision loss [2].

Conflict of interest: Nil.
Acknowledgement: None.
Funding: Nil.
References
- Dutta Majumder, Parthopratim, Agrawal, Rupesh, McCluskey, et al. Current Approach for the Diagnosis and Management of Noninfective Scleritis. Asia-Pacific Journal of Ophthalmology. 2021; 10(2): 212-223. DOI: 10.1097/APO.0000000000000341.
- Boston LMR MD. Posterior Scleritis: A Diagnostic Challenge. www.reviewofophthalmology.com. https://www.reviewofophthalmology.com/article/posterior-scleritis-a-diagnostic-challenge.