
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Challenging differential diagnosis: Navigating the association of migraine, white matter lesions, and patent foramen ovale in a case of sudden visual impairment
PA Spanily1*; A Plesa2; F Antochi1
1Emergency University Hospital Bucharest, Romania.
2Emergency Military Hospital Bucharest, Romania.
*Corresponding Author : PA Spanily
Emergency University Hospital Bucharest, Romania.
Tel: +40747111305;
Email: ioan.patricia14@gmail.com
Received : Aug 12, 2024
Accepted : Aug 28, 2024
Published : Sep 04, 2024
Archived : www.jcimcr.org
Copyright : © Spanily PA (2024).
Abstract
Background: Visual impairments can be caused by various conditions affecting the visual pathway, including stroke, migraine, and multiple sclerosis. However, when diagnosing patients presenting with visual impairments, the presence of white matter lesions adds a layer of complexity, particularly in differentiating between Patent Foramen Ovale (PFO) related strokes and Multiple Sclerosis (MS). The increased presence of PFO, identified in patients suffering from migraine with aura, and the association between MS and migraines, further complicate the diagnostic process.
Case presentation: To illustrate the association of these conditions, we present the case of a 32-year-old male patient who was admitted to the Neurology Clinic with sudden binocular vision impairment. He experienced a visual field disturbance starting centrally and expanding outwards, resembling an oil stain pattern. Two similar previous incidents were reported, with the latter preceded by a headache syndrome. Additionally, the patient has been experiencing weekly headaches, suggestive of migraine headache for the past eight years. No other significant medical history was reported.
Conclusions: Given the overlap in clinical features and imaging findings between ischemic lesions due to the presence of either PFO or MS, in a patient with a history of migraines, establishing a certain etiology for the lesions described on the cerebral MRI can be extremely challenging. This differential diagnosis requires a comprehensive evaluation, including careful consideration of clinical features, neuroimaging findings, and potentially additional diagnostic tests as well as repeated imagistic studies, over the following years.
Keywords: Patent foramen ovale; Multiple sclerosis; Migraine; White matter lesions; MRI.
Citation: Spanily PA, Plesa A, Antochi F. Challenging differential diagnosis: Navigating the association of migraine, white matter lesions, and patent foramen ovale in a case of sudden visual impairment. J Clin Images Med Case Rep. 2024; 5(9): 3238.
Introduction
With the advancements in neuroimaging technologies, it is increasingly feasible to identify cerebral MRI irregularities, such as white matter lesions. However, the clinical significance and origins of these lesions continue to be investigated in various ongoing studies. They can arise from either vascular or non-vascular processes [1] (Table 1).
Vascular causes Non-vascular causes
It has been observed that the prevalence of PFO is significantly higher in individuals with migraine with aura compared to the general population. The prevalence of PFO in patients with migraine with aura is reported to be around 40-60%, whereas in the general population, it ranges from 20-30% [2].
The foramen ovale is a passage found in the interatrial septum during fetal development, which typically closes shortly after birth. When the foramen ovale remains open beyond the age of 3 years, it is referred to as a PFO [3]. When the pressure in the right atrium exceeds that in the left atrium, a right-to-left shunt can occur, potentially leading to paradoxical embolism under certain predisposing conditions. Studies are increasingly focused on investigating the role of PFO in the underlying mechanisms of migraine.
The diagnosis of PFO can be made using different diagnostic methods such as transthoracic and transesophageal ultrasound, transcranial Doppler with microbubble passage, or cardiac catheterization. Transcranial Doppler, specifically, has been shown to have a high sensitivity (97%) and specificity (93%) in detecting microemboli associated with PFO [4]. Depending on the number of microbubbles that are detected by transcranial doppler, the right-left shunt is classified using the Spencer Grading Scale [5].
Some patients with PFO and migraine have been observed to exhibit FLAIR hyperintensity in their cerebral MRI, particularly in the posterior circulation, including the occipital and juxtacortical regions [6].
Also, juxtacortical strokes, that are not caused by other identified vascular etiologies, have been attributed to the presence of a high risk PFO. The ROPE and PASCAL scores in this patients can establish an indication off percutaneous PFO closure, alongside a cardiological evaluation.
White matter lesions can also appear in MS and they are typically found in various locations such as periventricular, juxtacortical, infratentorial, and intramedullary. Additionally, it has been observed that more patients with MS experience migraine with or without aura, compared to the general population [7]. Still, is is uncertain if the migraines are triggered by the cerebral inflammatory process, or if there is any clear association at all between the two pathologies. More studies are needed in order to better understand the relationship between migraine and multiple sclerosis.
Considering all of these factors, diagnosing a patient who has a history of migraines, white matter lesions resembling those seen in MS, in the presence of a PFO can indeed be extremely challenging.
Table 1: Causes of white matter lesions.
| Vascular causes | Non-vascular causes |
|---|---|
| Microvascular ischemic disease | Inflammatory: Multiple sclerosis, neuromyelitis optica spectrum disorders, acute disseminated encephalomyelitis |
| Atherosclerosis | Infectious: HIV encephalopathy, neuroborreliosis, HSV and CMV encephalitis, neurosyphilis, Lyme encephalopathy |
| Migraine | Toxic |
| Amyloid angiopathy | Metabolic |
| Vasculitis | Neoplastic |
| Traumatic: radiotherapy, post-concussion | |
| Genetic |
Case presentation
A 32-year-old man, C.F., who does not have any notable medical history, including no history of smoking, was admitted to the Neurology Clinic for sudden binocular vision impairment. He described a visual field impairment, that initially appeared in the central region of his vision, and gradually expanded outward, resembling the pattern of an oil stain. Additionally, he experienced positive visual sensations, described as lights in different vision fields. The entire episode lasted for approximately 40 minutes, after which he fully regained his normal vision. Subsequently, he developed a headache. The results of the neurological clinical examination were found to be within the expected range.
He further reported experiencing two similar incidents of sudden visual field impairment. The initial episode occurred in 2014, following physical exertion and exposure to hot water, leading us to consider a potential Uhtoff phenomenon. The second episode took place in 2020 and was preceded by a headache syndrome.
Additionally, over the past eight years, the patient has been experiencing weekly episodes of right hemicrania, diffuse or retroocular headache. These headaches are described as non-throbbing, usually lasting eight hours, with a moderate intensity. They improve with Nonsteroidal Anti-Inflammatory Drugs (NSAIDs). Since two of these episodes were accompanied by visual disturbances, a preliminary diagnosis that aligns with the ICHD-3 criteria would be migraine with aura.
Following the patient’s symptoms, a gadolinium enhanced cerebral MRI was performed. The cerebral MRI revealed the presence of several white matter lesions (five) located in the juxtacortical and periventricular areas. These lesions appeared non-gadolinophilic.
These white matter lesions could have either vascular or non-vascular origins. Due to the fact that the lesions did not show gadolinium enhancement and the patient did not describe symptoms suggestive of an MS attack, we considered, at first, several vascular causes, including migraine attacks, microvascular ischemic disease, and vasculitis.
Migrainous infarction is diagnosed when the duration of the aura exceeds 60 minutes and a cerebral infarction is noted in a relevant brain area. However, neither of these characteristics were present in our patient’s case.
To investigate the possibility of vasculitis, we conducted specific laboratory tests such as an extended ANA (antinuclear antibody) profile, complement C3 and C4 levels, and immunoglobulin analysis, all of which yielded negative results. Furthermore, in consideration of a potential ischemic vascular cause, we pursued further etiological investigations (Table 2). These investigations ruled out other major causes of stroke but did reveal the presence of a PFO.
At the same time, we also investigated the possibility of a non-vascular etiology, including MS and Neuromyelitis Optica (NMO). We conducted tests for anti-AQP4 antibodies and anti-MOG, which yielded negative results. We also took into account infectious causes and conducted tests for anti-Borrelia burgdorferi antibodies, HIV, VDRL, and markers for viral hepatitis, all of which came back negative.
Furthermore, a lumbar puncture was performed to analyze the presence of oligoclonal bands, which were found to be positive. Optical Coherence Tomography (OCT) of the optic nerve and visual evoked potentials yielded normal results. A gadolinium enhanced cervical and thoracic spine MRI showed no spinal cord lesions.
Based on these findings, we were left with two potential hypotheses: microvascular ischemic disease in the context of a patent foramen ovale, and multiple sclerosis - Radiologically Isolated Syndrome (RIS).
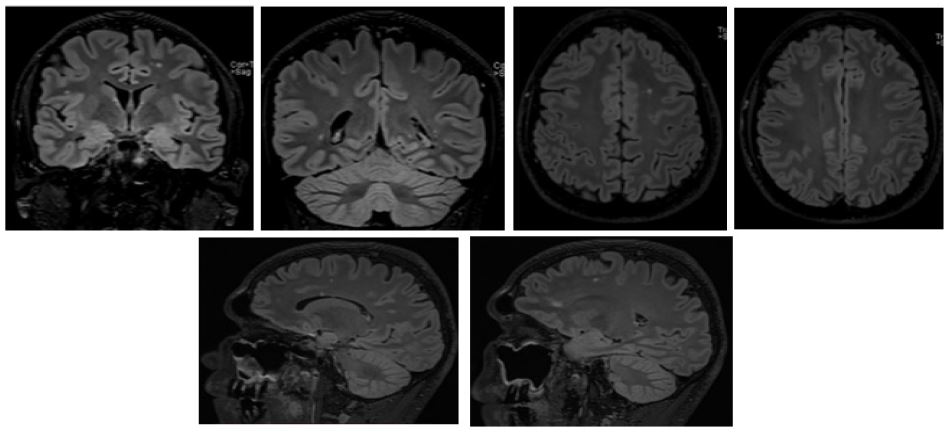
Table 2: Findings from etiological investigations.
| Investigation | Findings |
|---|---|
| AngioCT | Excludes atherosclerotic etiology, dissection, and vasculopathies. |
| Cervico-cerebral Doppler Ultrasound with Microbubble Passage | No atherosclerotic disease detected. Passage of approximately 20 microbubbles, indicating a PFO with right-left shunt. |
| Transesophageal Cardiac Ultrasound | 3 mm PFO (considered large), with passage of 20-30 bubbles; interatrial septum aneurysm and other cardioembolic causes excluded. |
| Hypercoagulability Tests | Coagulogram normal. Thrombophilia testing: negative. Anti-phospholipid antibodies absent. |
| 24-hour EKG Monitoring | No evidence of atrial fibrillation (AF). |
Discussion
The presence of juxtacortical lesions located superficially suggests a microembolic cause and provides support for the diagnosis of multiple PFO associated strokes. To assess the risk of paradoxical embolism, the ROPE score was used, which in this case yielded a score of 9 out of 10 points. Additionally, the PASCAL score was also calculated, indicating a high probability for the presence of PFO related strokes. Consequently, these scores were an indication that the patient should be refered to the Cardiology Clinic for percutaneous PFO closure.
The presence of nongadolinophilic juxtacortical and periventricular white matter lesions, along with the presence of oligoclonal bands and a possible Uhtoff phenomenon, but without clinical evidence of an MS attack, raised a suspicion that the patient might also have a RIS. Therefore, long-term follow-up using imagistic studies every 6-12 months (cerebral and cervical MRI with and without contrast) is necessary, to screen for new lesions and identify symptoms that might represent the first MS attack. Oligoclonal bands in patients with RIS suggest a higher risk of developing MS than in patients with RIS and no other associated findings.
Conclusion
The complex presentation of our patient makes it challenging to establish a definitive diagnosis. With the presence of multiple pathologies and overlapping clinical and imaging features, long-term follow-up is essential to track the progression of white matter lesions, even after a successful percutaneous closure of the PFO.
This case highlights the importance of proactive brain imaging in young patients experiencing headache syndromes. Despite the absence of clear guideline indications, such imaging can play a crucial role in establishing an accurate diagnosis or identifying associated conditions at an early stage.
It is important to recognize that not all white matter lesions in young patients signify a demyelinating disease such as MS, even if the imaging findings strongly suggest it. However, ongoing monitoring of these lesions can contribute to early detection and to an improved long-term prognosis due to early initiation of appropriate disease modifying therapy.
Furthermore, the presence of a PFO should be considered in young patients with localized, nongadolinophilic cortico-sub- cortical white matter lesions, without history of MS attacks.
Declarations
Conflict of interest statement: The authors declare that they have no conflict of interest in the publication of this case report.
Funding: This case report was not funded by a grant or public or non-profit sources.
IRB: IRB approval was not required for this case report. Data has been de-identified. Written consent was obtained from the patient for the use of health information including photographs.
Data availability:Data from this case report may be made available upon reasonable request.
References
- Sharma R, Sekhon S, Lui F, et al. White Matter Lesions. In: Stat-Pearls. Treasure Island (FL): StatPearls Publishing. 2024. https:// www.ncbi.nlm.nih.gov/books/NBK562167/.
- Kumar P, Kijima Y, West BH, Tobis JM. The connection between patent foramen ovale and migraine. Neuroimaging Clin N Am. 2019; 29(2): 261-270. doi: 10.1016/j.nic.2019.01.006.
- Romano V, Gallinoro CM, Mottola R, Serio A, Di Meglio F, et al. Patent foramen ovale-A not so innocuous septal atrial defect in adults. J Cardiovasc Dev Dis. 2021;8(60). doi:10.3390/ jcdd8060060.
- Mojadidi MK, et al. Accuracy of transcranial Doppler for the diagnosis of intracardiac right-to-left shunt: A bivariate meta-analysis of prospective studies. JACC Cardiovasc Imaging. 2014; 7(3): 236-250. doi:10.1016/j.jcmg.2013.12.011.
- D’Andrea A, Conte M, Riegler L, et al. Transcranial Doppler ultrasound: Incremental diagnostic role in cryptogenic stroke Part II. J Cardiovasc Echogr. 2016; 26(3): 71-77. doi:10.4103/2211-4122.187947.
- Signoriello E, et al. Migraine as possible red flag of PFO presence in suspected demyelinating disease. J Neurol Sci. 2018; 390: 222-226. doi:10.1016/j.jns.2018.04.042.
- Wang L, Zhang J, Deng ZR, Zu MD, Wang Y. The epidemiology of primary headaches in patients with multiple sclerosis. Brain Behav. 2021; 11(1). doi:10.1002/brb3.1830.