
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 5
Neuritis ossificans of the sciatic nerve
Michael Wilson1*; Anna Panagiotidou2; Christopher Wilson1; William Aston2; Michael Fox2
1Trauma & Orthopaedics, Dorset County Hospital, Wessex Deanery, UK.
2Royal National Orthopaedic Hospital, Stanmore, UK.
*Corresponding Author : Michael Wilson
Trauma & Orthopaedics, Dorset County Hospital,
Wessex Deanery, UK.
Email: wilsmd1@gmail.com
Received : Jul 17, 2024
Accepted : Aug 29, 2024
Published : Sep 05, 2024
Archived : www.jcimcr.org
Copyright : © Wilson M (2024).
Keywords: Neuritis; Ossificans; Sciatic Nerve.
Citation: Wilson M, Panagiotidou A, Wilson C, Aston W, Fox M. Neuritis ossificans of the sciatic nerve. J Clin Images Med Case Rep. 2024; 5(9): 3240.
Introduction
Neuritis Ossificans, known as intraneural heterotopic ossification, is a rare condition impacting peripheral nerves. Symptoms typically include pain and paraesthesia along the affected nerve’s distribution. The cause of this condition remains unknown. This unusual case managed in a tertiary referral centre for peripheral nerve injury, highlights the successful conservative management of a patient with neuritis ossificans affecting the sciatic nerve, showing both clinical and radiological resolution within 12 months.
Case presentation
A 43 year old female patient presented to a district general hospital with a 4 week history of right sided thigh pain and reduced sensation over the lateral aspect of her right leg. The pain was insidious in onset, constant in nature, and resistant to simple analgesia. There was no history of trauma. The patient suffered from hypothyroidism for which she took levothyroxine, but otherwise was medically fit and well.
On initial examination there was a distinct 20 mm x 30 mm lump in the posterior aspect of the right thigh, which was tender on palpation. Lower Limb motor function throughout all myotomes was intact, MRC (Medical Research Council) grade 5. Sensation was reduced in superficial and deep peroneal nerve distribution to the right leg. There was a negative Tinel’s test along the sciatic nerve at the point of the lesion.
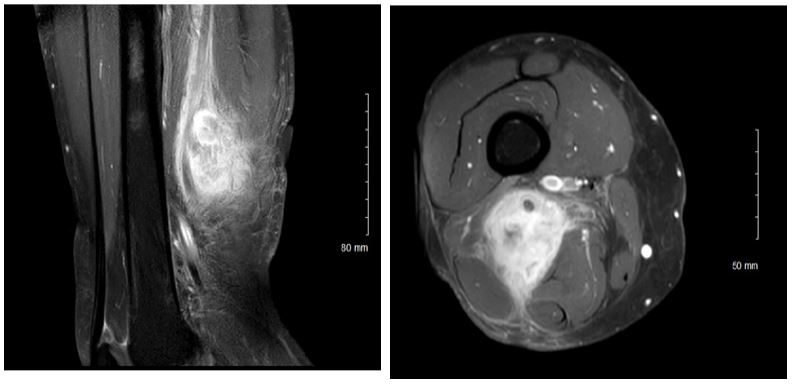
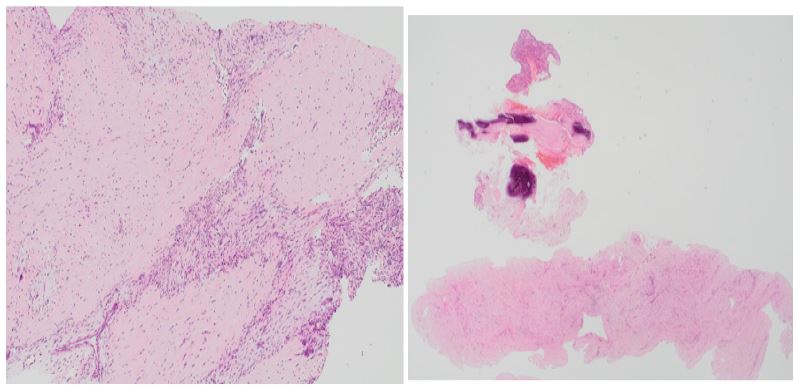
Initial radiographs were unremarkable. Magnetic Resonance Imaging (MRI) showed a well-defined 45 mm x 46 mm x 51 mm lesion (Figure 1), closely related to the sciatic nerve, with surrounding soft tissue oedema. Ultra-sound guided needle core biopsy was performed under general anaesthesia. Histological examination (Figure 2) revealed a USP6-rearranged ossifying tumour, and given the anatomical location the features were consistent with neuritis ossificans.
Following confirmation of the diagnosis, the patient was referred to the Peripheral Nerve Injury Unit at the Royal National Orthopaedic Hospital (RNOH) and was seen at 6 months post diagnosis. The significant delay to the outpatient clinic appointment was likely secondary to the Covid-19 pandemic effect on clinic waiting lists at the time of this clinical case. During this period of 6 months of unintentional conservative management, the clinical situation changed. The patient described the character of her pain had improved, it was no longer sharp in nature, with no radiation down the leg. The pain had improved on simple analgesia alone. On clinical examination, the numbness in the distribution of the common peroneal nerve had almost completely resolved. Due to the significant improvement in the patient’s symptoms, the decision was made in clinic to continue conservative management for the lesion.
At 11 months post diagnosis, a repeat MRI scan was performed (Figure 3) - showing a remarkable recovery of the neuritis ossificans affecting the sciatic nerve. The patient was successfully discharged from outpatient clinic, with no further re-presentations.

Discussion
Intraneural heterotopic ossification (neuritis ossificans) is an extremely rare condition, providing a challenge to the clinician with regards to both diagnosis and management [1].
Cross sectional imaging - specifically Magnetic Resonance Imaging (MRI), remains the gold standard imaging modality for detecting inflammatory changes within these lesions. Histopathology studies [2] display a classical appearance of neuritis ossificans. This is a characteristic zonal pattern: A fibroblastic core primarily of fibroblasts, an intervening zone of osteoid - an unmineralized organic component of the bone matrix, and a peripheral layer of ossification - in which new bone is formed [2].
In the current literature to date, there have been only 10 reported cases of this condition affecting distal peripheral nerves. Of these, 70% of the cases (7 cases) were managed surgically with excision of the lesions [3-5]. Surgical removal has associated risks with the sacrifice of some fascicles or the complete nerve, and thus has the potentially devastating clinical consequences of nerve resection. However, since 2009 there are no reports of surgical removal being utilised as a treatment modality, with the 3 most recent reported cases of neuritis ossificans all being managed conservatively [3].
In all three conservatively managed cases, a full clinical resolution was achieved. The medical management has included the use of Non-Steroidal Anti-Inflammatory Drugs (NSAID) and Gamma-Aminobutyric Acid (GABA) analogues for neuropathic pain [3]. Unfortunately, two of the cases managed conservatively, did not have any follow up imaging as it was not felt to be required clinically [1,6]. The one case reported in 2011 which has a post -treatment MRI scan, shows ongoing residual involvement of the affected nerve, but without any active inflammation [7]. None of the ten previously reported cases of neuritis ossificans has resulted in a recurrence of the disease process [1].
This report remains the only case of neuritis ossificans affecting the sciatic nerve to show both clinical and radiological resolution within a 12-month period, following conservative management. In our opinion, this unusual case adds weight to the modern literature of successfully treating these lesions conservatively, and thus avoiding the potentially life-changing complications associated with resection of a nerve.
Acknowledgements: The authors thank the research team at its institution for collecting and managing the patient data, and for the patient themselves for their time and effort contributing to the data used in this case report.
References
- Murthy NK, Fritchie KJ, Amrami KK, Rose PS, Spinner RJ. Diffuse Neuritis Ossificans of the Brachial Plexus: Case Report and review of the literature. World Neurosurg. 2020; 141: 363-366.
- George DH, Scheithauer BW, Spinner RJ, Buchler U, Cronin TE, et al. Heterotopic ossification of peripheral nerve (“neuritis ossificans”): report of two cases. Neurosurgery. 2002; 51: 244-6.
- Trigkilidas D, Lidder S, Delaney D, Pollock RC, Saifuddin A. Neuritis ossificans of the common peroneal nerve: a case report. Skeletal Radiol. 2009; 38: 1115-1118.
- Muzaffar N, Ahmad N, Bhat A, Shah N. Neuritis ossificans of the radial nerve. Orthopedics. 2012; 35: e589-e591.
- Yoshida S, Taira H, Kataoka M, Takita C, Tsumura H. Idiopathic heterotopic ossification within the tibial nerve. A case report. J Bone Joint Surg Am. 2002; 84: 1442-1444.
- Wasman JK, Willis J, Makley J, Abdul-Karim FW. Myositis ossificans-like lesion of nerve. Histopathology. 1997; 30: 75-8.
- Katz LD, Lindskog D, Eisen R. Neuritis ossificans of the tibial, common peroneal and lateral sural cutaneous nerves. J Bone Joint Surg Br. 2011; 93: 992-994.