
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Black esophagus: A devastating consequence - A case report and comprehensive literature analysis
Agrawal Nirav1*; Sharma Akshay1; Louis-Jean Scarlet1; Singh Sanmeet1,2
1Department of Internal Medicine, Luminis Health, Anne Arundel Medical Center, Annapolis, MD, USA.
2Department of Gastroenterology, Luminis Health, Anne Arundel Medical Center, Annapolis, MD, USA.
*Corresponding Author : Agrawal Nirav
Department of Internal Medicine, Luminis Health, Anne Arundel Medical Center, Annapolis, MD, USA.
Email: nirav1191@gmail.com
Received : Aug 02, 2024
Accepted : Sep 02, 2024
Published : Sep 09, 2024
Archived : www.jcimcr.org
Copyright : © Nirav A (2024).
Abstract
Acute Esophageal Necrosis (AEN) is a rare condition characterized by circumferential black discoloration and necrosis of the esophageal mucosa. This report presents a case of a 79-year-old female with metastatic cancer diagnosed with black esophagus and literature reviews of 68 cases. Our literature search highlighted common presenting symptoms were hematemesis (55%), gastrointestinal symptoms (54%), and melena (19%). And comorbidities including, malignancy (~10%) being leading cause of AEN. Age, low hemoglobin, and hypotension are associated with increased mortality. Management typically involves supportive care, but in cases of advanced malignancy, treatment may focus on symptom control and palliation.
Keywords: Acute esophageal necrosis; Black Esophagus; Malignancy; Endoscopy.
Abbreviations: AEN: Acute Esophageal Necrosis; GERD: Gastroesophageal Reflux Disease; Hb: Hemoglobin; EGD: Esophagogastroduodenoscopy; ESRD: End-Stage Renal Disease; CKD: Chronic Kidney Disease; COPD: Chronic Obstructive Pulmonary Disease; HLD: Hyperlipidemia; MEN1: Multiple Endocrine Neoplasia Type 1.
Citation: Nirav A, Akshay S, Scarlet LJ, Sanmeet S. Black esophagus: A devastating consequence - A case report and comprehensive literature analysis. J Clin Images Med Case Rep. 2024; 5(9): 3244.
Introduction
Acute esophageal necrosis, commonly known as “black esophagus,” is a rare and potentially life-threatening condition characterized by the circumferential black discoloration and necrosis of the esophageal mucosa. This condition was first described by Goldenberg et al. in 1990, and since then, numerous case reports and small case series have been published in the literature [1]. The exact pathogenesis of the black esophagus remains unclear, but it is believed to result from a combination of factors leading to compromised blood supply to the esophagus, such as low-flow states, vasculopathy, and mucosal ischemia. Proposed risk factors and associated conditions include diabetes mellitus [2], alcohol abuse, malnutrition, Gastroesophageal Reflux Disease (GERD), vascular disease, hypoperfusion states (e.g., shock, cardiac disease), and certain medications or procedures that may impair esophageal perfusion [3,4]. The clinical presentation of black esophagus is often non-specific, with upper gastrointestinal bleeding (hematemesis, melena) being the most common symptom. Other associated symptoms may include epigastric pain [5], nausea, vomiting, dysphagia, and odynophagia. Diagnosis is typically made through endoscopic evaluation [6], revealing the characteristic circumferential black discoloration and necrosis of the esophageal mucosa, often involving the distal esophagus and abruptly stopping at the gastroesophageal junction [7]. Here, we present a case report of a black esophagus in a 79-year-old female with metastatic cancer.
Case report
A 79-year-old female with a past medical history of type 2 diabetes mellitus, hypertension, dementia, and hyperlipidemia, presented to the emergency department with worsening abdominal swelling, and dyspnea on exertion. Her initial vitals showed hypertension 172/92 mmHg, tachycardia 104 bpm, tachypnea 22 breaths/min, temperature 97.7°F, and oxygen saturation 98% on room air. Pertinent labs were Hemoglobin (Hb) 11.2 g/dL, platelets 373 x103/μL, AST 15 U/L, ALT 5 U/L, glucose 260 mg/dL, and creatinine 1.3 mg/dL. On exam, the lungs exhibited decreased breath sounds at the bases bilaterally. Imaging revealed peritoneal carcinomatosis with a large pelvic mass measuring 12.7 x 10.8 x 16.7 cm (Figure 1). Bilateral pleural effusions and ascites were also present. Paracentesis fluid analysis showed metastatic mucin-producing adenocarcinoma, tumor cells are positive for pan cytokeratin, CK20, and CDX2. The findings were suggestive of metastatic adenocarcinoma of colorectal origin. Oncology was consulted, but no treatment options were appropriate for the patient at this time as the prognosis was very poor. And recommended a palliative care consult. On hospital day 26, she developed coffee-ground emesis, her Hb dropped to 5.6 g/dL and was hypotensive to 82/64 mmHg, requiring 2 units of packed RBCs. On day 28, she underwent an Esophagogastroduodenoscopy (EGD) revealing circumferential black discoloration of the esophagus concerning for acute necrotic esophagus (Black esophagus) (Figure 2) with biopsy showing erosive esophagitis; she was treated with intravenous proton pump inhibitors, sucralfate, and hydration. Given the patient’s overall poor prognosis in the setting of malignancy, no follow-up EGD was recommended. Her course required 4 paracenteses removing ~10L of fluid, and 1 thoracentesis for symptomatic management. As she was not a candidate for further cancer treatment, detailed goals of care discussions with the family were done. The patient was transitioned to hospice care; unfortunately, the patient passed away in the hospital before being discharged.
Results
The study involved 68 patients diagnosed with the black esophagus, with a mean age of 60.37 (16.28) years. The majority of the patients were males (67%), while females accounted for 32%. The most common presenting symptom was hematemesis (55%), followed by other gastrointestinal symptoms (54%, nausea, vomiting, diarrhea, dysphagia, dysphonia, odynophagia), abdominal pain (22%), and melena (19%). Some patients experienced loss of consciousness (7%) or altered mental status (6%). Significant comorbidities included diabetes mellitus (42%), alcohol use disorder (25%), drug addiction (16%), and gastrointestinal conditions such as GERD, cirrhosis, and hepatitis (25%). Hypertension was present in 20% of the patients, while renal comorbidities (19%, including end-stage renal disease, chronic kidney disease, and renal transplant), cardiac conditions (12%), and lung disease (4% with COPD) were also reported. Malignancy was observed in 10% of the patients, and other comorbidities, such as hyperlipidemia and multiple endocrine neoplasia type 1, were present in 4% of the cases (as Table 1). Table 2 showing acute esophageal necrosis demographic and clinical data review. As per our literature review, Figure 3 shows the prognosis of black esophagus cases over the past 2 decades where the number of cases recorded in the literature has increased, likely from more awareness, early diagnosis, and resources like EGD availability across the health care system. Moreover, there is a clear increase in survival rate in patients diagnosed with black esophagus (Represented by the green line) with a downtrend of deceased patients (Represented by the red line).
Table 1: Demographics of all included patients with AEN.
| Variables | N=68 |
|---|---|
| Age | 60.37 (16.28) |
| Gender (%) | |
| Male | 67 |
| Female | 32 |
| Presenting symptoms (n) | |
| Hematemesis | 38 |
| Melena | 13 |
| Abdominal pain | 15 |
| Other GI symptoms* | 37 |
| Loss of consciousness | 5 |
| Altered mental status | 4 |
| Comorbidities (n) | |
| Hypertension | 14 |
| Diabetes Mellitus | 29 |
| Drug addiction | 11 |
| Alcohol use disorder | 17 |
| GI (GERD, cirrhosis, hepatitis) | 17 |
| Cardiac | 8 |
| Renal (ESRD, CKD, Renaltransplant) | 13 |
| Lung (COPD) | 3 |
| Malignancy | 7 |
| Others (HLD and MEN1) | 3 |
Table 2: Summary of literature review.
| Sr. No | Author | EGD findings | Biopsy | Cause | Treatment | Prognosis |
|---|---|---|---|---|---|---|
| 1 | Porcu et al [18] | N/A | N/A | Thoracic endoluminal aortic repair | Cholecystostomy, Tazocilline,amikacin | Deceased (non-BE related) |
| 2 | Akkinepally et al [19] | Lower half of esophagus showedsigns of necrosis (exudates and distal blackening), DU | N/A | Alcoholic cirrhosis | IVF, PPI, NPO | Deceased (non-BE related) |
| 3 | Lee et al [20] | Distal half blackening of theesophagus | Reactive glandular cells withacute inflammation and necrosis. | Alcohol-induced chemicalesophagitis with Achalasia and hypotensive episodes | PPI, broadspectrum abx, IVF | Survived |
| 4 | McLaughlin et al [21] | Ischemic changes starting 25 cmfrom the incisors and ending abruptly at the gastroesophageal junction,shortened esophagus | N/A | N/A | IVF, NG tube, broad-spectrum abx | Survived |
| 5 | Carrillo et al [22] | Typical blackish esophageallesions with exudates | N/A | Several hypotension episodes | N/A | N/A |
| 6 | Garas et al [23] | N/A | Features of ischaemia andassociated haemorrhagic necrosis | N/A | PPI, antiemetics, NPO | Deceased |
| 7 | Altenburger et al [24] | Esophagus was black with ischemicnecrosis of the mucosa, submucosa, and muscularis | Diffuse acute inflammatoryinfiltrate, brown pigmentation limited to the mucosa | N/A | N/A | Deceased |
| 8 | Singh D et al [25] | Blackened esophagus, necroticappearing pale esophageal mucosa, and normal GE junction | Necrotic debris, absence ofepithelium, granulation tissue, and heavy leukocytic infiltrates | DKA | NG tube, PPI, broad-spectrum abx,antifungal agent | Survived |
| 9 | Singh D et al [25] | Necrotic appearing friable areasof spontaneous bleeding | N/A | N/A | NPO, PPI,100 units of botulinimtoxin injected at LES | Survived |
| 10 | Singh D et al [25] | Dusky appearance in distal 10 cmof esophagus with areas of superficial ulceration suggestive of ischemia | N/A | N/A | NPO, PPI, TPN | Deceased |
| 11 | Singh D et al [25] | Diffuse blackened esophagealmucosa, friable mucosa | N/A | N/A | PPI, broad spectrum abx | Deceased |
| 12 | Singh D et al [25] | Middle to distal esophagusappeared necrotic | N/A | DKA | NPO, PPI | Survived |
| 13 | Lahbabi et al [26] | Lower third mucosa was black andcovered by an exudate of the same color associated with diffuse bleeding | Necrotic debris, mucosalsubmucosal necrosis with a local inflammatory response | N/A | PPI, TPN | Deceased |
| 14 | Pereira et al [27] | Extensive candidiasis and ablack-appearing oesophageal mucosa compatible with necrosis at the distal 2/3of the oesophagus | N/A | Esophageal candidiasis,hypotension episode, alcohol abuse | PPI, TPN, NPO, fluconazole | Survived |
| 15 | Singh S et al [28] | Extensive ulceration, sloughingand multiple areas of necrosis in the distal oesophagus and stomach | N/A | Dabigatran adverse effect | PPI, broad spectrum abx, NG tube | Survived |
| 16 | Kwon et al [29] | Black macerated mucosa in the midthird of the esophagus and circumferential mucosal necrosis with a hugeadherent blood clot in the distal third of the esophagus | N/A | Coronary angiography complicatedwith hypotension | PPI | Survived |
| 17 | Shimamura et al [30] | Thick black stripes involving thedistal esophagus, with a sharp demarcation at the squamocolumnar border | Leukocyte infiltration withhemosiderosis. | DKA | IVF, PPI, NPO | Survived |
| 18 | Lu et al [31] | N/A | N/A | Foreign body ingestion | Exploratory laparotomy (removedthe fish bone) | Deceased |
| 19 | Zaid et al [32] | Circumferential blackpigmentation, fragile esophageal necrotic mucosa, and multiple superficialulcerations in the middle and lower thirds of esophagus.The lower one-thirdof esophagus was covered with dark exudates, oozing fresh red-colored bloodwith minimal touch | Focal area of ulceration. Theulcerated area was replaced by local inflammatory changes comprising necroticdebris, neutrophil exudates, hemorrhage, and background fibrinous materialdeposition. | N/A | IVF, PPI, NPO, analgesia, TPN | Survived |
| 20 | koksal et al [33] | Circumferential, black colored,necrotic distal esophageal mucosa abruptly turning to normal at thegastroesophageal junction and a giant necrotic based ulcer covering theanterior aspect of the first portion of the duodenum. | N/A | DM | IVF, PPI, NPO,sulbactam-ampicillin | N/A |
| 21 | Galtes et al [34] | N/A | Severe necrosis of the mucosa andsubmucosa with absence of viable squamous epithelium and an abundance ofnecrotic debris. Marked acute inflammatory infiltrates and partialdestruction of muscle fibres | DKA | N/A | Deceased |
| 22 | Kim S et al [35] | Necrotic tissue on loweresophagus, necrotic tissue from bulb to distal area of duodenum | N/A | Likely from COVID-19 infection | NG tube, IVF, PPI, NPO, broadspectrum abx | Survived |
| 23 | Pineo et al [36] | N/A | N/A | cocaine abuse | PPI, IV opioids, NG tube, G-CSF,broad-spectrum abx, exploratory laparotomy | Deceased |
| 24 | Shafa et al [4] | black necrotic mucosacircumferentially throughout the entire esophagus. | N/A | Septic shock | supportive care | Deceased |
| 25 | Shafa et al [4] | diffuse esophageal necrosis aswell as a small segment of denuded mucosa that was actively oozing blood | N/A | alcohol abuse or heart failure | Bleeding esophageal segment wasinjected with epinephrine, PPI, NPO, TPN | Survived |
| 26 | Shafa et al [4] | acute esophageal necrosis from thecricopharyngeus to the gastroesophageal junction | Inflammatory exudate and necroticdebris | N/A | IV PPI, NPO | Survived |
| 27 | Shafa et al [4] | circumferential necrosisthroughout the esophagus and a mid-esophageal stricture 5 cm in length. | N/A | Alcohol, cocaine, cannabis abuse, DKA | Surgically placed gastrostomy tubeand supportive therapy | Survived |
| 28 | Shafa et al [4] | pan-esophageal necrosis withcircumferential involvement distally | N/A | N/A | Supportive care | Deceased |
| 29 | Shafa et al [4] | necrosis in the distal third ofhis esophagus | N/A | multiorgan dysfunction | N/A | Deceased |
| 30 | Alcaide et al [37] | Esophageal lumen diffuselydilated, with submucosal hemorrhages and confluent violet-blackish areas,hiatal hernia | Esophageal mucosa withmicro-hemorrhages and microscopic foci of necrosis | N/a | IVF, PPI | survived |
| 31 | Nunes et al [38] | black esophagus covered with darkfluid, hyperaemia and erosions. | N/A | Paraesophageal hernia and gastricvolvulus | Emergency surgery repaired thediaphragmatic hernia, achieved volvulus reduction and a Nissen fundoplication | survived |
| 32 | Osterman et al [39] | Severe diffuse ulcerationbeginning in the mid esophagus, with continued severe ulceration throughoutthe distal esophagus, stomach and duodenum | N/A | re-initiating clozapine andquetiapine | N/A | Deceased |
| 33 | Matsuo et al [40] | black esophagus with ulceratedlongitudinal necrosis in the lower esophagus | N/A | N/A | PPI, NPO | survived |
| 34 | Crescenzi et al [41] | diffuse, circumferential,blackappearing mucosa in the distal third of the esophagus | N/A | Septic shock | IVF, PPI, TPN and broad-spectrumabx | survived |
| 35 | Ullah et al [42] | circumferential necrotic, friableoesophagus that extended from 21 cm to 40 cm from the incisors. There wasassociated friable red mucosa | N/A | cocaine abuse | IVF, PPI, sucralfate suspension | Deceased |
| 36 | Sato et al [43] | black discoloration from theesophagus to the gastric junction, esophageal perforation and blackdiscoloration in the duodenem | N/A | N/A | thoracic cavity drain, esophagealstent (FSEMS), SBT gastric balloon, IVF | survived |
| 37 | Haghbayan et al [44] | circumferential black mucosa inthe distal esophagus, immediately proximal to the gastroesophageal junction | N/A | DKA | PPI, NPO, insulin, IVF | survived |
| 38 | Kondo et al [45] | diffuse black discoloration of theesophageal mucosa that affected the distal esophagus and stopped abruptly atthe gastroesophageal junction | Necrosis of the esophageal mucosa | DKA | PPI, NPO, insulin, IVF | survived |
| 39 | Ullah et al [46] | circumferential necrotic, friableoesophagus extending from 21 to 38 cm from the incisors | N/A | Dialysis-induced hypotension | NG tube, IVF, PPI, IV sucralfate | Deceased |
| 40 | Tomori et al [47] | necrotic esophagitis in the middleand lower parts of the esophagus and duodenal erosions | No findings suggestive ofesophageal necrosis | Strongyloides stercoralishyperinfection and dissemination | NG tube, ivermectin, broadspectrum abxkim s | survived |
| 41 | Dias et al [48] | friable, diffuse black-appearingdistal esophageal mucosa with an abrupt transition at the gastroesophagealjunction | N/A | Septic shock | Percutaneous cholecystostomy, IVF,PPI, NPO, broad-spectrum abx | survived |
| 42 | Uyar et al [49] | diffusecircumferential black appearance throughout the entire esophagus mucosa | Histologicalappearance of Candida hyphaes and necrosis in esophagus tissue | N/A | PPI, IVF, anti-fungal for candidain the bx | N/A |
| 43 | Tanaka S et al [50] | diffuse erosiveesophagitis with black discoloration predominantly affecting the loweresophagus and abruptly interrupted at the gastroesophageal junction | N/A | N/A | PPI, IVF, abx | N/A |
| 44 | Siddiqi A [51] | inflammation of theepiglottis, arytenoid cartilages, and dark mucosal pigmentation of the distaltwo-thirds of the esophagus with associated hiatus hernia | Fragments offibrinopurulent exudate, and necrotic tissue with predominant neutrophilinfiltration indicating severe inflammation | N/A | PPI, IVF, abx | N/A |
| 45 | Deliwala Ss et al [52] | Blacknecrotic-appearing mucosa encompassing the entire esophagus and endingabruptly at the GEJ with associated gastric erosions and proximal duodenalulcerations | Acute esophagealsterile gangrenous necrosis | N/A | PPI, IVF, abx | N/A |
| 46 | Bhattacharya et al [53] | Circumferential black oesophagealmucosa extending proximally from the gastro-oesophageal junction. | The duodenumcontained microscopic foci of neuroendocrine tumour consistent withgastrinoma. | MEN related | PPI, IVF, abx | Survived |
| 47 | Kim NY et al [54] | Circumferentialblack pigmentation, and edematous mucosa covered by exudates was noted at themid-lower esophagus | An ulcer, andimmunohistochemistry showed negative cytomegalovirus (CMV), herpes simplexvirus (HSV-1), and HSV-2 polymerase chain reaction findings. | post renal transplantation | PPI, abx | Survived |
| 48 | Kroner et al [55] | Diffuse severemucosal changes of the middle and lower third of the esophagus characterizedby black-discoloration, erythema, and friable tissue with ulceration,sloughing and contact bleeding | Biopsies wereconsistent with acute esophageal necrosis, also known as “black esophagus”. | post renal transplantation | PPI, and TPN | Survived |
| 49 | Riascos et al [56] | Extensive esophagealnecrosis from the cricopharyngeal muscle to the esophageal-gastric junctiontransmurally at 30 cm, with a perforation of approximately 15 mm at 35 cm. | N/A | N/A | PPI, abx, fluconazole | Survived |
| 50 | Laverick et al [57] | A blackdiscolouration of the distal oesophagus with deep black ulcers and diffuseoozing of blood. | N/A | N/A | PPI, abx | Survived |
| 51 | Mustafa et al [58] | Two large 1.5–2 cmwide-based ulcers in the distal oesophagus without active bleeding | An ulceratedsquamous mucosa with extensive necrosis extending to the muscularis propria.Coccoid bacterial colonies and rare fungal forms suggestive of Candidaspecies were seen in the necrotic areas. | N/A | PPI, fluconazole | Survived |
| 52 | Iwamoto et al [59] | Entire circumferenceof the whole esophagus was shown to have turned black | N/A | HHS | treated the HHS | Survived |
| 53 | okamoto et al [60] | N/A | N/A | N/A | Survived | |
| 54 | okamoto et al [60] | N/A | N/A | N/A | Survived | |
| 55 | okamoto et al [60] | N/A | N/A | N/A | Survived | |
| 56 | okamoto et al [60] | N/A | N/A | N/A | Survived | |
| 57 | okamoto et al [60] | N/A | N/A | N/A | Survived | |
| 58 | okamoto et al [60] | N/A | N/A | N/A | Survived | |
| 59 | okamoto et al [60] | N/A | N/A | N/A | Survived | |
| 60 | okamoto et al [60] | N/A | N/A | N/A | Survived | |
| 61 | okamoto et al [60] | N/A | N/A | N/A | Survived | |
| 62 | Kitawaki [61] | circumferentialnecrosis of the middle and distal esophagus, immediately proximal to thegastroesophageal junction | N/A | N/A | PPI | |
| 63 | alsakarneh et al [62] | severe inflammationwith black discoloration consistent with acute esophageal necrosis in themiddle and lower esophagus, and erythematous duodenitis | N/A | N/A | PPI, sucralfate, NPO | Survived |
| 64 | Jeican et al [63] | N/A | N/A | N/A | N/A | Deceased |
| 65 | Ifuku [64] | circumferential mucosal injury andpartial necrosis from the middle esophagus to the gastroe- sophageal junctionwith a sudden transition to normal mu- cosa at the distal portion | N/A | cynotic spells from co-morb | PPI and NPO for 2 days | Survived |
| 66 | Greco S et al [65] | circumferentialblack appearance of the esophageal mucosa, as in concentric necrosis of thedistal esophagus with possible fungal superinfection. | Fungal hyphae by Candida spp. | N/A | IV fluconazole | Survived |
| 67 | Patil et al [66] | Diffuse ischemic andnecrotic mucosa beginning approximately 20 cm from the teeth and extendingdistally, and a large distal esophageal perforation extending into thestomach. | Gross surgicalspecimen analysis and immunohistochemistry were consistent with diffusenecrosis. | N/A | surgical esophagectomy andcervical esophagostomy | Survived |
| 68 | Gonzalez diaz et al [67] | diffuse circumferential blackmucosa covered by fibrin, affecting the middle third and distal esophagus.These changes progressively worsened from the proximal to distal esophagus,until reaching the eso- phagogastric junction | N/A | N/A | N/A | N/A |

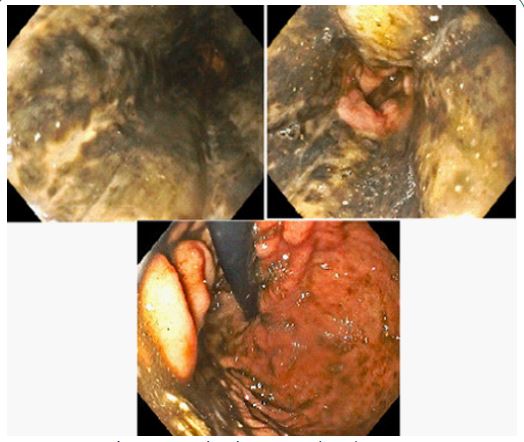
Endoscopic features of black esophagus showing diffuse esophageal necrosing in all the three images.
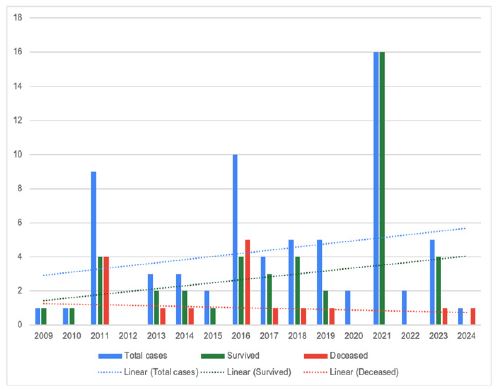
Demonstrates the prognosis of black esophagus cases over the past 2 decades where the number of cases recorded in the literature. Additionally, showing linear trends, blue line representing increase in total number of cases, red line indicating decrease in mortality and green line indicating improved survival.
Discussion
The findings from our literature review are consistent with the existing knowledge of black esophagus. The mean age of the patients in our study (60.37 years) aligns with the reported predominance of this condition in older adults, likely due to the presence of comorbidities and compromised vascular supply.[8] The male predominance (67%) observed in our study is also consistent with previous reports, although the underlying reason for this gender difference remains unclear [9]. The presenting symptoms and comorbidities identified in our study are in line with the established literature. Hematemesis (55%) and other gastrointestinal symptoms (54%) were the most common presenting complaints, reflecting the underlying mucosal injury and bleeding associated with black esophagus.[10] Comorbidities such as diabetes mellitus (42%), alcohol use disorder (25%), and gastrointestinal conditions (25%) are well-recognized risk factors for the development of black esophagus, as they can contribute to vascular compromise, mucosal ischemia, and esophageal injury [11,12]. In the current case report, the patient was an elderly female with multiple comorbidities, including diabetes mellitus, hypertension, and hyperlipidemia. While she did not have any known history of alcohol or drug abuse, her advanced metastatic cancer and overall poor prognosis likely contributed to a compromised vascular supply and increased susceptibility to esophageal necrosis. Similarly, a study by [13], providing a broader perspective on prognostic factors for mortality, showed that age, low hemoglobin, and hypotension were factors associated with increased mortality. Notably, my patient had all three of these risk factors, which increased her mortality risk. Interestingly, our analysis found a relatively high prevalence of malignancy (10%) among patients with black esophagus. While malignancy itself may not directly cause black esophagus, the associated treatments or complications (e.g., chemotherapy-induced mucositis, malnutrition, immunosuppression) could potentially predispose patients to this condition. This finding is particularly relevant in the context of our case report [14], where the patient’s underlying malignancy and poor prognosis likely played a significant role in the development of black esophagus. It is noteworthy that Day et al. published a case report with a review of the literature in 2009, which included most of the cases reported until 2008. In our review, we excluded those studies and focused on more recent cases [15], incorporating literature from 2009 to 2023, making our case report one of the most up-to-date compilations of black esophagus cases. The management of black esophagus typically involves supportive care, including intravenous fluid resuscitation, proton pump inhibitors, antibiotics, and nutritional support. In our case report, the patient received appropriate management with intravenous proton pump inhibitors [16], sucralfate, and hydration. However, given the patient’s overall poor prognosis due to advanced metastatic disease, no further interventions or follow-up endoscopy were pursued, aligning with the palliative care approach. It is important to recognize that black esophagus can be a manifestation of underlying systemic illness or compromised vascular supply, and prompt diagnosis and management are crucial to prevent potential complications, such as esophageal perforation, mediastinitis, or sepsis. In cases of advanced malignancy or poor prognosis [17], as in our case report, the management may be tailored toward symptom control and palliation, with careful consideration of the risks and benefits of invasive interventions.
Conclusion
Acute esophageal necrosis is an uncommon but severe condition typically affecting older individuals with underlying medical conditions that compromise blood flow to the esophagus. Rapid diagnosis through endoscopy and prompt supportive treatment, such as intravenous fluids, proton pump inhibitors, and antibiotics, are essential. However, in cases where patients have advanced malignancy or a poor overall prognosis, the management approach may focus more on palliative care and symptom relief, carefully weighing the potential risks and benefits of invasive procedures.
Acknowledgement: None.
Conflict of interest: None.
References
- Goldenberg SP, Wain SL, Marignani P. Acute necrotizing esophagitis. Gastroenterology. 1990; 98(2): 493-496.
- Gurvits GE. Black esophagus: acute esophageal necrosis, anecdotal experience of 2 cases. 2010; 44(4): 273-275. doi:10.1097/MCG.0b013e3181c39406
- Gurvits GE, Cherian K, Shami MN, et al. Black esophagus: new insights and a systematic review of the literature. 2021; 66(6): 1805-1819. doi:10.1007/s10620-020-06548-7.
- Shafa S, Sharma N, Keshishian J, Dellon ES. The black esophagus. Clin Gastroenterol Hepatol. 2016; 14(10): 1420-1424. doi: 10.1016/j.cgh.2016.05.021.
- Gurvits GE, Shapsis A, Lau N, Gualtieri N, Robilotti JG. Acute esophageal necrosis: a rare syndrome. 2007; 42(1): 29-38. doi:10.1007/s00535-006-1974-z.
- Senese G, Barrenechea E, Gonzalez A, et al. Acute necrotic esophagus: a case series and systematic review. 2022; 28(7): 790-803. doi:10.3748/wjg.v28.i7.790.
- Augusto F, Fernandes V, Cremers MI, et al. Acute necrotizing esophagitis (black esophagus): descriptive analysis of 43 cases. 2004; 36(3): 227-230. doi:10.1055/s-2004-814193.
- Sako A, Yoshimura K, Hori Y, et al. Acute esophageal necrosis: reports of 29 cases. 2018; 43(1): 8-14.
- Dutta R, Jamieson C. Acute necrotizing esophagitis: a case report. 2020; 89(1): 50-53.
- Lacy BE, Toor A, Bensen SP, Rothstein RI, Maheshwari Y. Acute esophageal necrosis: report of two cases and a review of the literature. 1999; 49(4 Pt 1): 527-532. doi:10.1016/s0016-5107(99)70052-5.
- Tsokos M, Reinhold R, Sachse N, Kleereman N, König M, et al. Black esophagus induced by chemotherapy combined with impaired blood supply. 2021; 82: 102233. doi: 10.1016/j.jflm.2021.102233.
- Wang AY, Khoury T, Bellizzi AM. Acute esophageal necrosis: a case report and review of literature. 2018; 55(2): 134-139. doi: 10.1016/j.jemermed.2018.04.037.
- Kim SM, Song KH, Kang SH, et al. Evaluation of prognostic factor and nature of acute esophageal necrosis: Restropective multicenter study. 2019; 98(41): 17511. doi:10.1097/MD.0000000000017511.
- Singh D, Amin R, El Chibane I, Jessel M, Barker S. Acute necrosis of the esophagus: case report and review of the literature. 2013; 19(4): 185-187. doi:10.4103/1319-3767.114516.
- Cho SY, Lee YM, Han JH, Lee YH, Cho TS, et al. Clinical presentation and management of acute esophageal necrosis. 2021; 11(1): 14753. doi:10.1038/s41598-021-94212-2.
- Riascos RF, Leon M, Quinteros R, Guerrero J, Franco J, et al. A multifactorial approach for an accurate diagnosis and appropriate treatment of acute esophageal necrosis. 2014; 79(3): 480-487.
- Porcu A, Cavallo P, Guemando RV, et al. Black esophagus after thoracic endoluminal aortic repair. Ann 2015; 100(5): 87-88. doi:10.1016/j.athoracsur.2015.04.111.