
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Incidental vestibular schwannoma, personality change and LGI-1 antibody related autoimmune encephalitis - A coincidence which delayed diagnosis
Naveen Kumar*; Neeraj Kumar; Beerbhan Singh; Surekha Dabla
Department of Neurology, Pt BDS, PGIMS, Rohtak, India.
*Corresponding Author : Naveen Kumar
Department of Neurology, Pt BDS, PGIMS, Rohtak,
India.
Email: nvnranga744@gmail.com
Received : Aug 12, 2024
Accepted : Sep 03, 2024
Published : Sep 10, 2024
Archived : www.jcimcr.org
Copyright : © Kumar N (2024).
Citation: Kumar N, Kumar N, Singh B, Dabla S. Incidental vestibular schwannoma, personality change and LGI-1 antibody related autoimmune encephalitis - A coincidence which delayed diagnosis. J Clin Images Med Case Rep. 2024; 5(9): 3247.
Introduction
Autoimmune Encephalitis (AE) is an emerging autoimmune inflammatory neurological disorder in which antibodies are directed against intracellular or cell surface neuronal antigens in Central Nervous System (CNS). Autoimmune Encephalitis (AE) can be subcategorized on the basis of presence of specific autoantibody. Among these Anti-leucine-rich glioma-inactivated 1 limbic encephalitis (anti-LGI1 LE) is a rare entity which presents with rapidly progressive dementia, Faciobrachial Dystonic Seizures (FBDS), refractory hyponatremia and mental disorders [1]. Less than 10 % of cases are associated with various tumors but none is reported with a vestibular schwannoma which is a benign tumor and does not spread to other brain area. Presentation in vestibular schwannoma is usually due to cranial nerve involvements however trigeminal acoustic schwannomas are strongly associated with psychiatric symptoms affecting limbic pathways [2,3]. Here we report an adult patient who presented with abnormal behavior with incidentally detected large left cerebellopontine angle tumor without any involvement of limbic system or trigeminal area on brain imaging. Later when patient developed acute psychosis a possibility of Paraneoplastic vs autoimmune encephalitis was kept and patient was extensively worked up for the same. His Autoimmune panel reports strongly positive for LGI-1 antibody (Leucin rich glioma -inactivated protein 1) and PET Brain was also supportive of Limbic encephalitis. Patient was managed with both IVIG and methylprednisolone and he improved markedly.
Case presentation
A 63-year-old male, presented with a 15 days history of cognitive impairments and psychiatric disturbances. The patient had recent rapid memory decline, difficulty in comprehending simple commands, disorientation of time and place, confusion in activity of daily routine. He also had history of auditory hallucinations, agitation, and irritability. He was admitted under neurology ward after several episodes of agitation.
On examination: Patient was conscious but confused and smiling inappropriately. All the vitals were normal, Chest/ Abdomen /CVS- Normal; Neurological Examination- MMSE-21/30; Detailed mental status examination could not do as patient was not cooperative with examination. Cranial Nerves, Motor and Cerebellar examination was normal. No signs of meningeal irritation were present.
Investigations: His complete blood count, Renal function Test, Serum Electrolytes, Liver function tests and Lipid profile were normal. Thyroid functions showed T3-1.02 ng/ml (0.8-2.0), T4-7.02 ug/dl (5.10-14.10), TSH–1.41 uIU/ml (0.27-4.20) and anti TPO antibodies were Negative. Patient was tested negative for Anti-HIV, HBsAg and Anti HCV. Cerebrospinal fluid study revealed clear, transparent fluid, no coagulum, sugar-79 mg/dl (RBS:123 mg/dl), Protein 28 mg/dl, TLC-<05/cumm (100% L), Indian ink & cryptococcal antigen negative, AFB and Gram stain-negative, CBNAAT for MTB-negative. CSF Neuro-viral Panel (including herpes simplex virus 1, 2, and herpes zoster virus)-Negative, S.B12 levels -325 pg/ml (180-914), VDRL – Negative, Urine for Toxicology screening also negative. His CXR was normal and Ultrasound abdomen was normal. Brain magnetic resonance imaging (MRI) showed left Cerebello Pontine (CP) angle space occupying lesion and Possibility of left vestibular schwannoma was kept (Figure 1).
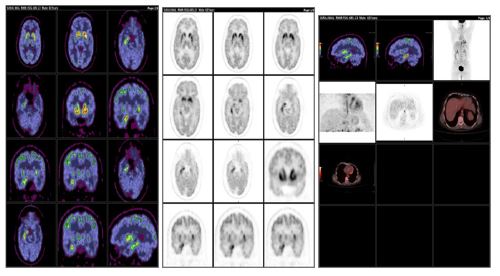
Symptoms were initially attributed to be associated with vestibular schwannoma However, his symptoms worsened rapidly. Hence a possibility of autoimmune vs paraneoplastic encephalitis was kept. Chest computed tomography and the whole-body positron emission tomography (Figure 3) examination didn’t reveal any neoplastic etiology.
18F-FDG PET-CT Whole Body (Figure 3): B/L symmetrically increased metabolic avidity in caudate and putamen and asym- metrically increased metabolic avidity in right mesial temporal lobe-likely encephalitis (consistent with Limbic encephalitis) pattern. No definite scan evidence of any abnormal hyper metabolic disease focuses elsewhere in the body to suggest any malignancy.
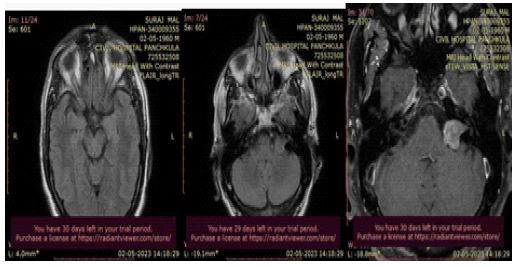
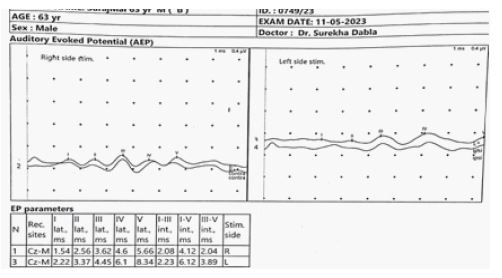
The study shows intracranial extra axial space occupying mass lesion in left CP angle cistern extending into the porous acousticus of internal auditory canal. The lesion is showing a definite intracanalicular component which is extending up to its entire length. The lesion shows ice cream appearance. It is showing hyperintense mildly hyper intense signal on T2W images and homogeneous post contrast enhancement abutting the left MCP and cerebellar hemisphere without any mass effect Possibilityofleftvestibularschwannomais likely. Electroencephalogram was normal. Brainstem auditory responses showed-peak latencies of wave I and V and interpeak latencies of wave I-V prolonged on left side and normal on right side (Figure 2).
LGI-1 antibodies in both CSF and serum were strongly positive by cell-based transfection immunofluorescence assay. This satisfies the diagnostic criteria of anti-LGI1 LE. The other immune indexes, such as glutamic acid receptor antibodies (NMDA/transfection cells, AMPA1/transfection cell, and AMPA2/transfection cell), voltage-gated potassium channels/ contact protein-related protein 2 antibodies/transfection cells, were all negative.
Course in hospital: Considering the possibility of LGI LE we managed the patient with immunoglobulin (0.4 g/kg/d, continued for 5 days), Injection Methylprednisolone 1000mg for 5 days and followed by prednisone (50 mg/d, reducing 10 mg/ month for 3 months). He improved markedly on the 10th day of the treatment, the patients’ cognitive function almost returned to normal, with Mini-Mental State Examination score 29/30 and Montreal Cognitive Assessment score 25/30. Moreover, psychiatric symptoms were significantly improved with Neuropsychiatric Inventory score 2/144 and discharged in very stable condition.
Discussion and conclusions
Autoimmune encephalitis has antibodies directed against neuroglial cell surface antigen or intracellular antigen. In comparison to the AE associated with intracellular antigens, Neuroglial Surface-Directed Antibodies (NGS Abs) related spectrum have a subacute onset of symptoms, association with symptom course and antibody levels, good response to immunotherapies and are less frequently associated with malignancies4. Frequently detected Neuroglial surface-directed antibodies are identified are the N-Methyl-D-Aspartate Receptor (NMDAR) and components of the Voltage-Gated Potassium Channel (VGKC) complex, which includes Leucine Rich Gliomainactivated 1 (LGI1), Contactin-Associated Protein 2 (CASPR2), and contactin-2. LGI1 antibodies associated limbic encephalitis is characterized by cognitive impairment, seizures-classically Faciobrachial Dystonic Seizure (FBDS), psychiatric disorders, and refractory hyponatremia [4,5]. Here we report a case of anti-LGI1 Limbic encephalitis who presented with neuropsychiatric symptoms of subacute onset. Metabolic workup was normal and on MRI brain he had vestibular schwannoma. In view of its association with neuropsychiatric symptoms in some cases, patient was managed symptomatically. However, his symptoms worsened rapidly with cognitive decline and then further work-up was done to look for autoimmune encephalitis and then he was diagnosed as a case of anti LGI1 limbic encephalitis. LGI 1 is a secretory synaptic glycoprotein predominantly located in the temporal cortex and cornuammonis6. Interaction of antigen antibody at hippocampus leads to inflammatory process and later sclerosis if not treated leading to characteristic symptoms. Owing to its varied presentation and a subacute onset it is easily misdiagnosed. Delayed treatment is associated with residual deficit with persistent cognitive impairments in form of worse verbal and visuospatial memory performance, while early immunotherapy was associated with better memory outcomes [7]. Co-presence of tumor is rare, and most such cases are thymomas [8] but till now none has reported association with vestibular Schwannoma. In our case it might be a coincidence but it definitely delayed the diagnosis and management because psychosis and other mental illness are reported with vestibular Schwannomas as well. In summary, we show that anti-LGI1 LE is reversible and treatable. As treatment of rapidly progressive dementia, new onset seizures and neuropsychiatric symptoms is entirely dependent on the diagnosis, a comprehensive, structured, but pragmatic approach to diagnosis, including key clinical, laboratory, and radiologic features is critical for better outcomes and patient’s quality of life. Furthermore, we should follow up with the patient for a long time to monitor the possibility of recurrence.
References
- Irani SR, Michell AW, Lang B, et al. Faciobrachial dystonic seizures precede Lgi1 antibody limbic encephalitis. 2011; 69: 892.
- Takeda M. 100 Years of the Japanese Journal of Psychiatry and Neurology the year of 1911-cerebellopontine angle tumor. 2011; 113: 930-932.
- Huang WL, Hsieh MH, Liao SC. Acoustic neuroma identified after electroconvulsive therapy in a patient with recurrent major depression and undifferentiated somatoform disorder. 2010; 26: 330-331.
- Irani SR, Vincent A. The expanding spectrum of clinically-distinctive, immunotherapy responsive autoimmune encephalopathies. 2012; 70: 300-304.
- Zuliani L, Graus F, Giometto B, et al. Central nervous system neuronal surface antibody associated syndromes: review and guidelines for recognition. 2012; 83: 638-645.
- Herranz-Pérez V, Olucha-Bordonau FE, Morante-Redolat JM, Pérez-Tur J. Regional distribution of the Leucine-Rich Glioma Inactivated (LGI) gene family transcripts in the adult mouse brain. 2010; 1307: 177-94.
- Jang Y, Lee ST, Lim JA, et al. Psychiatric symptoms delay the diagnosis of anti-LGI1 encephalitis. 2018; 317: 08-14.
- Ohkawa T, Fukata Y, Yamasaki M, et al. Autoantibodies to epilepsy-related LGI11 in limbic encephalitis neutralize LGI1-ADAM22 interaction and reduce synaptic AMPA receptors. 2013; 33: 18161-74.