
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
A case of granulomatosis with polyangiitis misdiagnosed as severe asthma: The key role of spirometry
Cecilia Calabrese1*; Alessio Sola1; Marco Balestrino1; Federica Massaro1; Laura Ferrentino2; Stefano Badolato1; Valentina Morgillo1; Serena Vettori3; Gaetano Rea4; Carmine Guarino5
1Department of Translational Medical Sciences, University of Campania “Luigi Vanvitelli”, Naples, Italy.
2Department of Translational Medicine, Federico II University, Via Sergio Pansini 5, 80131, Naples, Italy.
3Department of Medicine, Monaldi Hospital, Napoli, Italy.
4Department of Radiology, Monaldi Hospital, Naples, Italy.
5Unit of Bronchology, Monaldi Hospital, Naples, Italy.
*Corresponding Author : Cecilia Calabrese
Department of Translational Medical Sciences,
University of Campania “Luigi Vanvitelli”, Naples,
Italy.
Email: cecilia.calabrese@unicampania.it
Received : Aug 13, 2024
Accepted : Sep 04, 2024
Published : Sep 11, 2024
Archived : www.jcimcr.org
Copyright : © Calabrese C (2024).
Citation: Calabrese C, Sola A, Balestrino M, Massaro F, Ferrentino L, et al. A case of granulomatosis as polyangiitis misdiagnosed as severe asthma: The key role of spirometry. J Clin Images Med Case Rep. 2024; 5(9): 3248.
Introduction
Granulomatosis with Polyangiitis (GPA) is a granulomatous, necrotizing small-vessel vasculitis associated with the presence of Antineutrophil Cytoplasmic Antibodies (ANCA). In more than eighty percent of GPA patients ANCA have a Cytoplasmatic Pattern at the indirect immunofluorescence (c-ANCA) and recognize the autoantigen Proteinase 3 (PR3), while in few cases they have a perinuclear pattern (p-ANCA) and are directed toward the autoantigen Myeloperoxidase (MPO) [1]. However, in patients with limited disease or at early stages ANCA status can be negative. Although diagnostic criteria have not been established, the diagnosis usually relies on clinical, radiological and serological findings usually supported by the histological examination and/or by the presence of ANCA positivity. When a diagnosis of small or medium vessel vasculitis has already been made, recently updated classification criteria can be adopted to differentiate GPA form the other ANCA associated-vasculitis; the diagnosis of GPA can be made when the score is ≥ 5 (Table 1) [2].
GPA usually starts involving the upper respiratory tract with crusting rhinitis, nasal obstruction, nasal septum perforation, oral or nasal ulcerations, saddle-nose deformities, sinusitis, and otitis. From the ear–nose–throat tract, GPA can progress with lung, kidney, ocular, gastrointestinal and peripheral nerve involvement, but any organ may be affected.
Three main kind of lung involvement in GPA patients have been described: 1) necrotizing granulomatous inflammation manifesting as single or multiple nodules or mass sometimes with central cavities; 2) tracheobronchial inflammation, with the development of masses and polyps, subglottic and/or tracheobronchial stenosis and pulmonary capillaritis, and, 3) inter- stitial lung disease in rare cases [3].
The frequency of the tracheobronchial involvement varies from 13.6–55% and is more frequent in women and younger GPA patients. Subglottic stenosis is the most common manifestation occurring in about 10–20% of cases; it may be the first manifestation of GPA, but, more frequently, appears during the course of the disease frequently associated with a severe sinonasal disease, usually without other organ involvement [3]. Clinical symptoms of subglottic stenosis depend on the degree of the obstruction: at the beginning, symptoms as cough or dyspnea can be mild or even absent, while in the most advanced cases they can become severe and life-threatening even requiring tracheostomy. The wheezing of patients with subglottic stenosis may often led to a misdiagnosis of asthma, especially when there is no other organ involvement. The presence of subglottic stenosis in patients with GPA can be suspected by spirometry. In fact, the flow-volume curve shows a typical plateau in both inspiratory and expiratory phases, consistent with a central fixed airway obstruction. Dynamic expiratory chest computed tomography (CT) allows to evaluate the stenosis and its degree [4]. Finally, fiberoptic broncoscopy is the gold standard for the diagnosis of subglottic stenosis consenting not only the direct visualization of the tracheobronchial tree but also to obtain biopsies for the histologic exam, to plan therapeutic interventions and to monitor tracheobronchial lesions [5]. Whether the diagnosis of SGS in patients with known GPA is quite easy, on the contrary, suspecting GPA when other clinical manifestations are not present is quite difficult.
Table 1: Criteria and their score for the diagnosis of GPA if the cumulative score is ≥5 points [2]
| Bloody nasal discharge, nasal crusting or sino-nasal congestion | +3 |
| Cartilaginous involvement | +2 |
| Conductive or sensorineural hearing loss | +1 |
| Cytoplasmic antineutrophil cytoplasmic antibody (ANCA) or anti-proteinase 3 ANCA positivity | +5 |
| Pulmonary nodules, mass or cavitation on chest imaging | +2 |
| Granuloma or giant cells on biopsy | +2 |
| Inflammation or consolidation of the nasal/paranasal sinuses on imaging | +1 |
| Pauci-immune glomerulonephritis | +1 |
| Perinuclear ANCA or antimyeloperoxidase ANCA positivity | -1 |
| Eosinophil count ≥1×109 /L | -4 |
Case presentation
A 47 years old woman, never smoking, not allergic, affected by type 1 diabetes, was admitted to our outpatient clinic for suspected severe asthma. The patient referred the onset of respiratory symptoms four years ago with a progressive exertional dyspnea and dry cough attacks. The patient showed previous spirometries judged “not evaluable” by doctors due to a poor patient’s cooperation. At the clinical examination, stridor was audible during inspiration. She had stable vital signs, 98% oxygen saturation on room air and a negative 6 MWT.
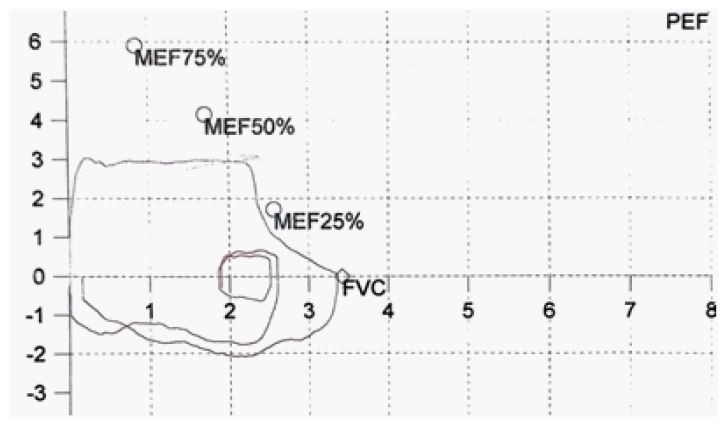
The patient performed a spirometry, and the flow volume curve showed a plateau in both forced inspiratory and expiratory phases with a box-like appearance suggesting a fixed central or upper airway obstruction, according to ERS/ATS guidelines [4]. Peak Expiratory Flow (PEF) was severely reduced (182,3 l/ min, 44% of predicted value) more than the Forced Expiratory Volume in the first second (FEV1) (2,61 L, 89% of the predicted value), with FEV1/PEF >8 ml/L/min suggestive of a fixed central airway obstruction (Figure 1).
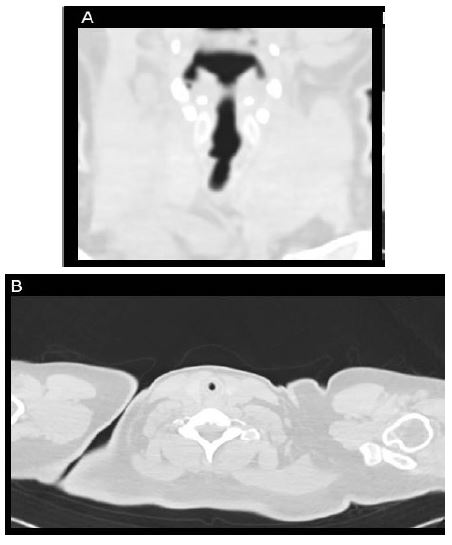
In order to detect the aetiology of the upper airway obstruction, a neck and chest inspiratory and dynamic expiratory High-Resolution CT was performed that showed a reduction of the transverse diameter of the trachea in the region between a plane below the glottis and the first two tracheal rings (Figure 2).
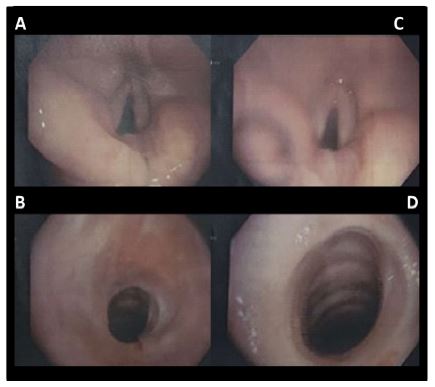
A Flexible Bronchoscopy (FB) was performed that detected a subglottic stenosis of about 7 mm diameter (Figure 3A and 3B). A FB mechanical dilatation of the stenosis from 7 mm to 10 mm was performed. The histological examination of biopsy samples showed fibrosis and chronic inflammation of the corion with squamous metaplasia and mild dysplasia of the epithelium.
Laboratory tests revealed positive p-ANCA (7,4 U/ml; range 3,5-5), negative c-ANCA, Anti-Nuclear Antibodies (ANA) 1:320 (nucleolar pattern), C-Reactive Protein (CRP) <0,4 mg/dl. Investigating more carrefully the anamnesis, the patient referred persistent nasal obstruction and crusting. A rhinoscopy demonstrated a bilateral atrophic rhinitis.
A diagnosis of ANCA-associated vasculitis was made and a further endoscopic management of the tracheal stenosis was programmed. In addition, low dose systemic corticosteroids and azathioprine were prescribed. An Yttrium-Aluminium-Garnet (YAG) laser via FB was performed with an enlargement of the tracheal stenosis that reached the transverse diameter of 11 mm (Figure 3C and 3D).
Six months after the FB procedure, the patient reported an improvement of dyspnea and dry cough and stridor was no longer audible. An improvement of both PEF (383,7 l/min, 94%) and FEV1 (3,12 L, 101%) with a change of the morphology of the flow-volume curve were observed at the spirometry (Figure 4).
Yag: A yttrium-aluminium-garnet; FB: Flexible bronchoscopy.

Conclusion
Spirometry is a non-invasive test that can play a key role in the diagnosis of upper airway diseases and should be performed in all patients with persistent respiratory symptoms as cough, dyspnea, hoarseness, and stridor, even when the clinical manifestations are not suggestive of the most common respiratory diseases as bronchial asthma or chronic obstructive respiratory disease. In fact, the flattening of the expiratory and/or inspiratory limb of the flow-.volume curve may consent an early diagnosis of pharynx, laryngeal, tracheal and mainstem bronchial stenosis [6]. Of note, it is very important a good patient’s cooperation during spirometry because a poor initial effort can affect the FEV1/PEF ratio; however the morphology of the flow–volume loop showing a repeatable pattern of a plateau in both forced inspiratory and expiratory flows suggests a fixed central or upper airway obstruction, while a plateau of the only forced inspiratory flow suggests a variable extra-thoracic upper airway obstruction and a plateau of the only forced expiratory flow suggests a variable intra-thoracic central airway obstruction [6]. As shown by our case report the plateau of the expiratory and inspiratory limb of the flow-volume curve allowed us to suspect a disease involving the central airways and to exclude bronchial asthma.
In our patient the suspicion of GPA was confirmed by the serological test with ANCA showing a perinuclear pattern and MPO positivity. Several studies have shown that GPA patients with MPO-pANCA positivity, in comparison with those with PR3-cANCA positivity have, more frequently, a limited disease with a high prevalence of subglottic stenosis and, as our patient, are predominantly young females, with fewer constitutional symptoms, milder renal lesions and lower relapse rates [7,8]. However, in a recent study, GPA patients with MPO-ANCA phenotype have been described older, with less prevalent upper airway involvement and neurological manifestations, increased end-stage renal disease and mortality [9]. Although biopsy is the gold standard for the diagnosis of GPA showing necrosis, granulomatous inflammation, and vasculitis, it may display atypical or not complete histological features, as in our patient [3].
Only one case report is present in literature showing the key role played by spirometry in the diagnosis of GPA. In this case, the presence of a biphasic pattern in both the expiratory and inspiratory limbs of the flow-volume curve, allowed to suspect a unilateral main- stem bronchial obstruction further confirmed by chest CT scan and bronchoscopy [10].
A recent study investigating pulmonary function in patients with ANCA associated vasculitis showed the presence of upper airway obstruction, diagnosed by a FEV1/PEF > 10, in 22% GPA patients, although only 5 among the 81 GPA patients received a definite diagnosis of tracheal or subglottic stenosis made by endoscopy [11]. For this reasons, the authors concluded that subclinical upper airway lesions may have been overlooked by spirometry. However, we can suppose that the forced expiratory maneuver can allow to detect the laryngeal/tracheal involvement in GPA at earlier stages not clearly evident at FB, and a strict follow-up can prevent life-threatening complications. In addition, the authors in their work utilized a FEV1/PEF ratio higher than that suggested by the current ERS guidelines and so some cases of upper airway involvement in GPA patients may be underdiagnosed [6].
A recent study showed a good correlation between the degree of subglottic stenosis measured by CT-based virtual bronchoscopy with conventional bronchoscopy and pulmonary function test [12]. Dynamic expiratory chest CT demonstrating a decrease more than 50% of the area of the tracheal lumen during exhalation (area during full inspiration - area during exhalation)/area during full inspiration) was proposed as screening diagnostic tool of central airways involvement in GPA [4]. Although being a noninvasive procedure, it is associated with the exposure to ionizing radiation, limiting its utility in the monitoring of subglottic stenosis in patients with GPA. In contrast, spirometry may be used in the follow-up of patients with tracheobronchial stenosis reducing the frequency of invasive procedure as bronchoscopy.
In GPA patients, previous studies have demonstrated that systemic treatments are frequently ineffective and recurrent bronchoscopic procedures are required in half cases [13]. The management of central airway stenosis is still a clinical challenge considering that it can be caused either by an ongoing active inflammatory process either by a cicatritial stenosis without inflammation. The activity of the underlying autoimmune systemic disease can be evaluated monitoring ANCA status and C-reactive protein levels. However, the optimal systemic treatments and endoscopic interventions and their best timing are not defined and subglottic and bronchial stenosis remain a life-threatening condition and a therapeutic challenge in the management of GPA patients.
References
- Lyons PA, Rayner TF, Trivedi S, et al. Genetically distinct subsets within ANCA-associated vasculitis. N Engl J Med. 2012; 367(3): 214-23. doi: 10.1056/NEJMoa1108735. PMID: 22808956; PMCID: PMC3773907
- Robson JC, Grayson PC, Ponte C, et al. 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology classification criteria for granulomatosis with polyangiitis. Ann Rheum Dis. 2022; 81(3): 315-320. doi: 10.1136/annrheumdis-2021-221795. Epub 2022 Feb 2. PMID: 35110333.
- Potentas-Policewicz M, Fijolek J. Granulomatosis with polyangiitis: clinical characteristics and updates in diagnosis. Front Med (Lausanne). 2024; 11: 1369233. doi: 10.3389/ fmed.2024.1369233. PMID: 39257888; PMCID: PMC11385631.
- Quinn KA, Gelbard A, Sibley C, et al. Subglottic stenosis and endobronchial disease in granulomatosis with polyangiitis. Rheumatology (Oxford). 2019; 58(12): 2203-2211. doi: 10.1093/ rheumatology/kez217. PMID: 31199488; PMCID: PMC7967893
- Villeneuve T, Prevot G, Pugnet G, Heluain V, Faguer S, Guibert N. Role of bronchoscopy for respiratory involvement in granulomatosis with polyangiitis and microscopic polyangiitis. Eur Respir J Open Res. 2023: 9; 00141–2023. doi: 10.1183/23120541-00141-2023
- Stanojevic S, Kaminsky DA, Miller MR, et al. ERS/ATS technical standard on interpretive strategies for routine lung function tests. Eur Respir J. 2022; 60(1): 2101499. doi: 10.1183/13993003.01499-2021. PMID: 34949706.
- Schirmer JH, Wright MN, Herrmann K, et al. Myeloperoxidase-Antineutrophil Cytoplasmic Antibody (ANCA)-Positive Granulomatosis With Polyangiitis (Wegener’s) Is a Clinically Distinct Subset of ANCA-Associated Vasculitis: A Retrospective Analysis of 315 Patients From a German Vasculitis Referral Center. Arthritis Rheumatol. 2016; 68(12): 2953-2963. doi: 10.1002/art.39786. PMID: 27333332.
- Chang DY, Li ZY, Chen M, Zhao MH. Myeloperoxidase-ANCA- positive granulomatosis with polyangiitis is a distinct subset of ANCA-associated vasculitis: A retrospective analysis of 455 patients from a single center in China. Semin Arthritis Rheum. 2019; 48(4): 701-706. doi: 10.1016/j.semarthrit.2018.05.003. Epub 2018 May 9. PMID: 29887327.
- Alba MA, Jennette JC, Hu Y, et al. Relevance of Combined Clinicopathologic Phenotype and Antineutrophil Cytoplasmic Autoantibody Serotype in the Diagnosis of Antineutrophil Cytoplasmic Autoantibody Vasculitis. Kidney Int Rep. 2022; 7(12): 2676-2690. doi: 10.1016/j.ekir.2022.09.011. PMID: 36506241; PMCID: PMC9727534.
- Agrawal A, Sahni S, Marder G, Shah R, Talwar A. Biphasic flow-volume loop in granulomatosis with polyangiitis related unilateral bronchus obstruction. Respir Investig. 2016; 54(4): 280-3. doi: 10.1016/j.resinv.2016.01.002. Epub 2016 Mar 17. PMID: 27424828.
- Dieterich J, Hellmich B, Mahrhold J, et al. Pulmonary function in patients with ANCA-associated vasculitis. Sarcoidosis Vasc Diffuse Lung Dis. 2024; 41(2): e2024025. doi: 10.36141/svdld. v41i2.15577. PMID: 38940708; PMCID: PMC11275547.
- Shitrit D, Valdsislav P, Grubstein A, Bendayan D, Cohen M, Kramer MR. Accuracy of virtual bronchoscopy for grading tracheobronchial stenosis: correlation with pulmonary function test and fiberoptic bronchoscopy. Chest. 2005; 128(5): 3545-50. doi: 10.1378/chest.128.5.3545. PMID: 16304311
- Girard C, Charles P, Terrier B, et al. Tracheobronchial Stenoses in Granulomatosis With Polyangiitis (Wegener’s): A Report on 26 Cases. Medicine (Baltimore). 2015; 94(32): e1088. doi: 10.1097/MD.0000000000001088. PMID: 26266344; PMCID: PMC4616693.