
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 5
Acquired reactive perforating collagenase’s with dermatomyositis: A rare case report
Qian Dong; Hongjun Lu; Yue Xi; Rui Zheng*
Shanxi Medical University, Taiyuan, Shanxi, China.
*Corresponding Author : Rui Zheng
Shanxi Medical University, No 56, Xinjian South
Road, Yingze District, Taiyuan, Shanxi, China.
Tel: +86-1382174197;
Email: zhengr2002@163.com
Received : Aug 15, 2024
Accepted : Sep 05, 2024
Published : Sep 12, 2024
Archived : www.jcimcr.org
Copyright : © Zheng R (2024).
Citation: Dong Q, Lu H, Xi Y, Zheng R. Acquired reactive perforating collagenase’s with dermatomyositis: A rare case report. J Clin Images Med Case Rep. 2024; 5(9): 3249.
Short report
65-year-old male who presented with recurrent erythema and pruritic papules for one year, Initially, he developed numerous keratotic red papules, featuring central umbilication and necrosis with scab formation. He was previously diagnosed with “nodular prurigo and eczema” and treated with oral ebastine, cetirizine, prednisone, and topical steroid cream. While the rash initially subsided, it recurred intermittently.
On March 5, 2024, he presented to our department. The patient denied any history of hypertension, diabetes, thyroid disease, rheumatic diseases, or HIV. There was no history of chronic ulcers, surgeries, trauma, or family history of similar diseases. Vital signs were normal. Dermatological examination revealed heliotrope rash on the eyelids and Gottron’s papules on the extensor surfaces of the metacarpophalangeal and interphalangeal joints, which were purple-red and covered with scales (Figure 1A). The trunk, limbs, and neck exhibited keratotic red papules with central umbilication, slightly raised crater-like edges, and some with necrosis and scab formation, without significant bleeding upon scab removal (Figure 1B). Muscle strength in the limbs was normal.
Laboratory tests showed no significant abnormalities in complete blood count, urinalysis, liver function, kidney function, coagulation profile. Antinuclear antibody was 1:80, C-reactive protein was 9.3 mg/L, and anti-Scl-70 antibody was strongly positive. Skin biopsy revealed hyperkeratosis with parakeratosis, thickened granular and spinous layers, focal epidermal necrosis, surface pus scabs, and perivascular lymphocytic infiltration in the superficial dermis (Figure 1C). Combining clinical and pathological findings, the diagnosis was confirmed as “1. Acquired reactive perforating collagenosis, 2. Dermatomyositis.”
Treatment included oral acitretin (20 mg/day), ebastine (8.8 mg/day), cetirizine (10 mg/day), and hydroxychloroquine (200 mg/day), topical steroid cream (twice daily) and Narrow-Band Ultraviolet B (NB-UVB) therapy (every other day). Four weeks after treatment, the patient’s pruritus completely resolved, and most skin lesions had subsided, indicating effective disease control. The patient is currently under routine follow-up in the rheumatology department with ongoing medication adjustments.
Acquired Reactive Perforating Collagenosis (ARPC) is a type of perforating dermatosis characterized by the extrusion of altered collagen through the epidermis. Its typical pathological features include cup-shaped epidermal invaginations containing parakeratotic debris and basophilic collagen fibers, with collagen bundles observed perforating vertically through the epidermis [1]. ARPC is rare, and its pathogenesis remains unclear [2]. In adults, it is associated with various systemic diseases such as diabetes, chronic renal failure, hyperlipidemia, hyperthyroidism (or hypothyroidism), liver disease, pulmonary fibrosis, HIV, pulmonary aspergillosis, scabies infection, lymphoma, leprosy, cancer, hemodialysis, and internal malignancies [1,2]. ARPC combined with rheumatic diseases is rare, studies have shown its association with vasculitis, systemic lupus erythematosus, and idiopathic myositis [3]. This association may be due to the inflammatory response originating from dermal connective tissue, which activates collagenase, leading to the penetration of collagen into the epidermis [4].
Currently, there is no cure for ARPC, and treatment mainly focuses on managing the associated systemic diseases. Dermatomyositis, as an immune-mediated inflammatory myopathy, involves multiple systemic pathological changes due to varying degrees of inflammation, autoimmunity, and vasculopathy [5]. In our patient, ARPC appeared to be closely related to the activity of dermatomyositis. The use of hydroxychloroquine significantly improved the patient’s skin symptoms. Cases of ARPC combined with dermatomyositis are extremely rare. Further research is needed to determine the potential association between dermatomyositis and ARPC.
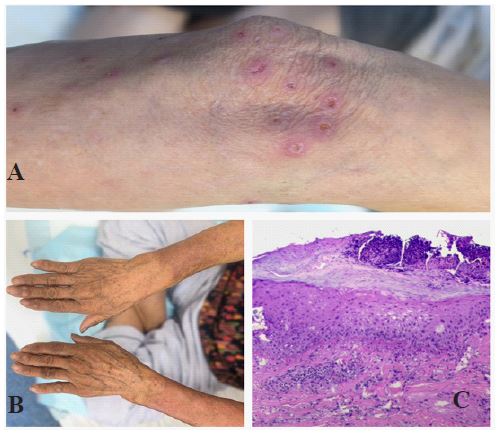
B: Symmetrically distributed purple-red papules on the extensor surfaces of the metacarpophalangeal and interphalangeal joints of both hands, known as Gottron’s papules. C: Pathological examination: hyperkeratosis with parakeratosis, thickened granular and spinous layers, focal epidermal necrosis, surface pus scabs, and perivascular lymphocytic infiltration in the superficial dermis.
Declarations
Conflict of interest statement: There are no conflicts of interest to declare.
Funding statement: None.
References
- Prados-Carmona A, De la Torre Gomar FJ. Acquired Reactive Perforating Collagenosis. The New England journal of medicine. 2023; 389(18): 37.
- Zhang X, Yang Y, Shao S. Acquired reactive perforating collagenosis: A case report and review of the literature. 2020; 99(22): 20391.
- Alenzi F. Reactive perforating collagenosis and systemic lupus erythematosus: A rare case report. Medicine. 2022; 101(48): 32138.
- Lee SJ, Jang JW, Lee WC, Kim DW, Jun JB, et al. Perforating disorder caused by salt-water application and its experimental induction. International journal of dermatology. 2005; 44(3): 210-4.
- Lundberg IE, Fujimoto M, Vencovsky J, Aggarwal R, Holmqvist M, et al. Idiopathic inflammatory myopathies. Nature reviews Disease primers. 2021; 7(1): 86.