
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Blood, sweat, smears
Brigid M Garrity, DO, MPH1*; Andrew Mittelman, MD2; Rebecca Levin, MD3
1Department of Emergency Medicine, Boston Medical Center, Boston, MA, USA.
2Boston University Chobanian & Avedisian School of Medicine, Boston, MA, USA; Department of Emergency Medicine, Boston Medical Center, Boston, MA, USA.
3Department of Pediatrics, Division of Pediatric Emergency Medicine, Boston University Chobanian & Avedisian School of Medicine, Boston, MA, USA.
*Corresponding Author : Brigid Garrity
Department of Emergency Medicine, Boston
Medical Center, Boston MA 02118, USA.
Email: bgarrit1@bu.edu
Received : Aug 15, 2024
Accepted : Sep 06, 2024
Published : Sep 13, 2024
Archived : www.jcimcr.org
Copyright : © Garrity BM (2024).
Citation: Garrity BM, Mittelman A, Levin R. Blood, sweat, smears. J Clin Images Med Case Rep. 2024; 5(9): 3252.
Introduction
A rare type of squamous cell cancer, known as sarcomatoid (spindle cell) carcinoma, is characterized by a biphasic tumor composition of carcinomatous and sarcomatous elements [1]. It is additionally referred to as collision tumour because epithelial and spindle cells originate from separate stem cells, pseudosarcomatous carcinoma, and pseudosarcoma [2]. Although the mean age at presentation is 58 years, it is crucial to keep in mind that a wide range of 14-87 years indicates significant variability in age at presentation [1]. It affects men more frequently than women. Even though the larynx may be a prevalent location for tumours, cancers of the oral cavity and oropharynx can still occur and should not be disregarded when making a diagnosis or developing a treatment strategy [2]. Seldom does it originate from the tongue. Smoking, consuming alcoholic beverages, and preceding head-neck radiation exposure are risk factors. A poorly differentiated form of squamous cell cancer is called sarcomatoid carcinoma and acts aggressively. Despite numerous studies utilizing immunohistochemistry, electron microscopy, and genetics, the exact histogenesis of sarcomatoid carcinoma remains a subject of debate. The motivation behind creating this case report stemmed from the patient in the index case, who had a rare history despite the presence of a highly aggressive tumor in an unusual location. It is essential to investigate a broad range of additional factors such as radiation therapy, pre-existing SCC, smoking, alcohol consumption, and tobacco use as common contributors to the development of this tumor. As a result, the case was explained to us in order to determine the many tumours causes and to raise awareness of this uncommon cancer.
Description
A 21-year-old male with no prior medical history presented to the emergency department for epistaxis and bleeding ulcers in his mouth. In addition to small ulcers with dried blood in the oropharynx, physical exam also revealed a petechial rash and bruising on his extremities that the patient noted were new and atraumatic. His white blood cell count (WBC) was 24.2 K/UL, lactate dehydrogenase was 1,193 U/L, and uric acid was 7.6. mg/dL. A peripheral blood smear was obtained (Figures 1 and 2).
Acute promyelocytic leukemia (APL) is a medical emergency that results from a translocation which causes fusion of the promyelocytic leukemia gene with the retinoic acid receptor alpha gene. APL often presents with hemorrhage including epistaxis, gingival bleeding, ecchymosis, and menorrhagia. Patients are at risk of disseminated intravascular coagulation (DIC) and hyperfibrinolysis which can result in life-threatening bleeding [1]. Approximately 30% of patients diagnosed with APL die within 30 days of diagnosis [2].
Emergent treatment with oral all-trans retinoic acid (ATRA) is recommended to stop cell differentiation and prevent death from hemorrhage, however about 35% of patients diagnosed never receive ATRA [3,4]. Patients with APL typically exhibit leukopenia. However, leukocytosis - as seen in this patient - is a poor prognostic marker. Patients with elevated WBC counts at diagnosis are at substantially increased risk of early mortality [2]. When a new diagnosis of APL is made in the emergency department, providers should consider emergent administration of ATRA in discussion with hematology and oncology.
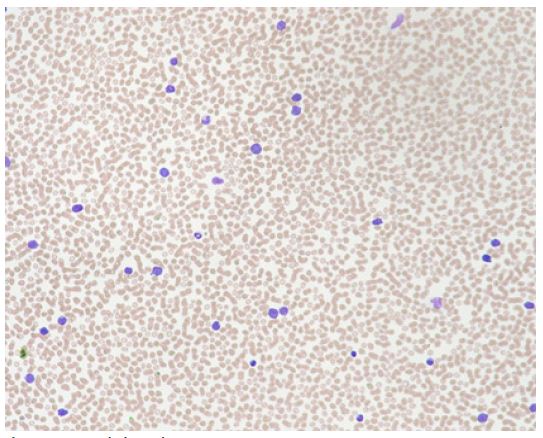
Peripheral smear showed poikilocytosis with occasional schistocytes.
References
- Cingam SR, Koshy NV. Acute Promyelocytic Leukemia. [Updated 2023 Jun 26]. In: StatPearls [Internet]. Treasure Island (FL): Stat-Pearls Publishing; 2024. Available from: https://www.ncbi.nlm. nih.gov/books/NBK459352/
- Lehmann S, Ravn A, Carlsson L, et al. Continuing high early death rate in acute promyelocytic leukemia: a population-based report from the Swedish Adult Acute Leukemia Registry. Leukemia 2011; 25: 1128–34.
- Mantha S, Goldman DA, Devlin SM, Lee JW, Zannino D, Collins M, Douer D, Iland HJ, Litzow MR, Stein EM, Appelbaum FR, Larson RA, Stone R, Powell BL, Geyer S, Laumann K, Rowe JM, Erba H, Coutre S, Othus M, Park JH, Wiernik PH, Tallman MS. Determinants of fatal bleeding during induction therapy for acute promyelocytic leukemia in the ATRA era. Blood. 2017; 129(13): 1763-1767. doi: 10.1182/blood-2016-10-747170. Epub 2017 Jan 12. PMID: 28082441; PMCID: PMC5374291
- Abedin S, Altman JK. Acute promyelocytic leukemia: preventing early complications and late toxicities. Hematol Am Soc Hematol Educ Program. 2016; 2: 10–15.