
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
DIY meets WOPN: Spontaneous erosion of a peripancreatic fluid collection into the stomach
Madison Peregoy1*; Andrew Mertz2; Patrick E Young2
1Department of Internal Medicine, National Capital Consortium, Walter Reed National Military Medical Center, Bethesda, USA.
2Department of Gastroenterology, Walter Reed National Military Medical Center, Bethesda, MD, USA.
*Corresponding Author : Madison Peregoy
Department of Internal Medicine, National Capital Consortium, Walter Reed National Military Medical Center, Bethesda 20889, USA.
Tel: 9105409667;
Email: madisonperegoy1@gmail.com
Received : Aug 21, 2024
Accepted : Sep 12, 2024
Published : Sep 19, 2024
Archived : www.jcimcr.org
Copyright : © Peregoy M (2024).
Keywords: Walled off pancreatic necrosis; Pancreatic pseudocyst; Endoscopy; Gastric fistula.
Abbreviations: DIY: Do it Yourself; WOPN: Walled Off Pancreatic Necrosis.
Citation: Peregoy M, Mertz A, Young PE. DIY meets WOPN: Spontaneous erosion of a peripancreatic fluid collection into the stomach. J Clin Images Med Case Rep. 2024; 5(9): 3259.
Background
Pancreatic fluid collections are a common complication of both interstitial and necrotizing pancreatitis. Drainage is indicated if there is a concern for superinfection or symptoms secondary to size or location. The proximity of the pancreas to the stomach and duodenum makes stenting the top therapeutic choice for drainage in many cases. Uncommonly, fluid collections can enlarge and erode into nearby structures. Herein, we describe a case of spontaneous infected pancreatic fluid collection decompression via gastric fistula.
Case presentation
A 55-year-old female with a history of chronic alcohol-related pancreatitis presented with abdominal pain and anorexia. Cross-sectional imaging revealed a homogenous large fluid collection located in the pancreatic head consistent with pseudocyst, which was followed with repeat imaging studies. She subsequently underwent uncomplicated Endoscopic Ultrasound (EUS) guided cyst duodenostomy with placement of a lumen opposing metal stent along with common bile duct stent placement for biliary obstruction. One month later she represented with recurrent abdominal pain, anorexia, fever, and leukocytosis. Repeat imaging studies revealed a new complex peripancreatic fluid and gas collection concerning an infected acute pancreatic fluid collection. She was scheduled for EUS- guided drainage the following day and interestingly improved symptomatically overnight just prior to the procedure. Upper endoscopy the following day revealed a 4 cm defect in the posterior gastric wall filled with healthy-appearing granulation tissue and necrotic debris, indicative of spontaneous decompression of the infected pancreatic fluid collection. Acid suppression therapy was discontinued and interval endoscopy after 3 weeks showed resolution of the defect.
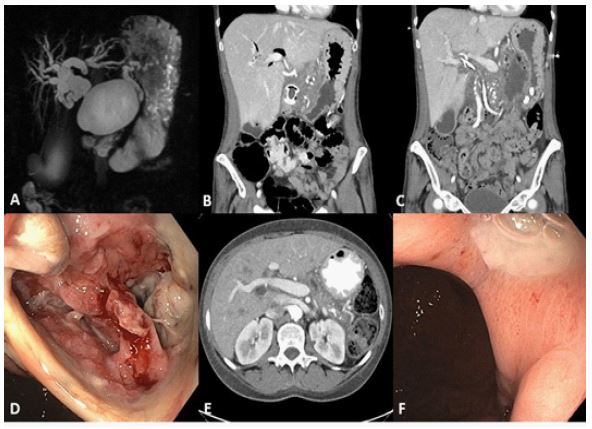
B: Imaging following LAMS placement with resolution of pseudo cyst.
C: CT reveaking large fluid collection near pancreatic tail with multiple air foci.
D: Endoscopic image of large gastric defect following erosion of pancreatic fluid collection into stomach.
E: CT revealing resolution of fluid collection following spontaneous decompression.
F: Healing ulcer at the site of prior gastric defect 1 month after decompression.
Discussion
Pancreatitis-associated fistulas are considered a rare complication of acute pancreatitis and management can vary from observation to surgical interventions. Conveniently in this case, a wide fistula formed with the exact organ to which drainage would be preferred. In such cases involving the stomach, acid suppression therapy can be held to promote gastric acid debridement of necrotic tissue, allowing the fistula to remain patent for adequate drainage. This case highlights a fortunate outcome for a patient with an infected pancreatic fluid collection, however it also reminds us to respect such fluid collections as they can hastily evolve.