
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 5
Multisystem inflammatory syndrome in Romanian children - A multicentric national retrospective study: Are there any differences between our cohort and published data?
Doina Anca Plesca1,2; Anca Draganescu1,3; Oana Cristina Patran4*; Vlad Monescu6; Maria Mitrica4,5; Laura Larisa Dracea4,5; Luciana Petrescu4; Oana Gabriela Falup-Pecurariu4,5
1University of Medicine and Pharmacy Carol Davila, Bucharest, Romania.
2Clinical Hospital for Children Victor Gomoiu, Bucharest, Romania.
3The National Institute of Infectious Diseases, Prof. Dr. Matei Bals, Bucharest, Romania.
4Emergency Clinical Hospital for Children, Brasov, Romania.
5Faculty of Medicine, Transylvania University, Brasov, Romania.
6Faculty of Mathematics and Informatics, Transylvania University, Brasov, Romania.
*Corresponding Author : Oana Cristina Patran
Emergency Clinical Hospital for Children, Brasov, Romania.
Email: oanapatran@yahoo.com
Received : Aug 19, 2024
Accepted : Sep 12, 2024
Published : Sep 19, 2024
Archived : www.jcimcr.org
Copyright : © Patran OC (2024).
Abstract
Multisystem Inflammatory Syndrome in Children (MIS-C) is a complication that occurs 4 to 6 weeks after an infection with SARS-CoV2. The aim of the study was to compare our data to the published literature and secondly to see if there are any prediction markers of the severity of the disease. We conducted a multicenter national retrospective study based on a cohort of 80 patients diagnosed with MIS-C from 3 centers in Romania. Patients were divided into 4 groups according to age: under 1 year, 1-5 years, 5-10 years and above 10 years. We compared demographic characteristics, clinical symptoms, lab results and treatment. Most common symptoms were fever (97.5%), pharyngeal hyperemia (76.2%) and rash (47.5%). We demonstrated the multisystem involvment of the disease based on clinical examination and lab results. High mean CRP values were found: 53.78 mg/dl in the first group, 52.24 mg/dl in the second, 88.24 mg/dl in the third and 112.79 mg/dl in the last one. Same pattern of increased values for increasing age groups were found for ferritin levels, both of them being correlated with more days of hospitalization. Nearly all patients received IV corticotherapy and antibiotics and only half of them received IV immunoglobulin. To the best of our knowledge this is the first multicenter study regarding MIS-C in our country regarding similarities and differences between our pacients and published data. We highlighted the importance of knowing possible evolution of the disease in order to choose the best treatment plan.
Keywords: Pediatric health; COVID19; MIS-C.
Citation: Plesca DA, Draganescu A, Patran OC, Monescu V, Mitrica M, et al. Multisystem inflammatory syndrome in Romanian children - A multicentric national retrospective study: Are there any differences between our cohort and published data?. J Clin Images Med Case Rep. 2024; 5(9): 3260.
Introduction
More than 290 million people have been infected with the novel coronavirus, called severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and more than 5.4 million deaths occurred. A total of 3,308,480 cases of Covid 19 were reported in Romania until December 2022 [1]. Children under the age of 9 represented 5% and under the age of 19 represented 7.5% according to the National Surveillance Data [2]. Since March 2020, when pandemic was declared, COVID-19 disease in children had mild or asymptomatic forms in nearly all cases. Most interesting feature of the disease was the particular complication that occurs 4 to 6 weeks after the infection with SARS-CoV2 [3]. This particular syndrome was named Pediatric Multisystem Inflammatory Syndrome temporally associated with COVID-19 (PIMS-TS) in Europe and Multisystem Inflammatory Syndrome in Children (MIS-C) in the USA. United Kingdom NHS was first to notice cases of a severe multisystem inflammatory syndrome in children previously affected by Covid 19. In USA, on April 7th 2020, the first 6 month old child with MIS-C was described. He was initially diagnosed with Kawasaki Disease (KD) [3]. There are several hypotheses regarding the pathophysiology of this syndrome, most incriminating an autoimmune reaction of the body to the viral infection. MIS-C is considered to be either an exacerbated immune system response or a maladaptive response characterized by hyperinflammation and a cytokine storm. The link between COVID-19 disease and this syndrome was demonstrated by Yonker et al [4]. that found prolonged presence of SARS-CoV2 virus in the gastrointestinal tract of children suffering of MIS-C [5]. Kawasaki disease was one of the first diseases with which the syndrome was being confused. Shana Godfred-Cato and co. elaborate a score to distinguish MIS-C from KD. They attribute 1 point to abdominal pain, headache, pericardial effusion and CRP>10 mg/dl, 2 points to platelets < 150x100/ uL, -1 point to rash and -2 points to mucocutaneous lesions. The likelihood of positive diagnosis of MIS-C increased as the score raises. Thrombocytosis is a characteristic of KD, while lymphopenia, increased d-dimer and ferritin value and cardiac findings like myocarditis with ventricular dysfunction are found more often in MIS-C [6].
Matrieal and methods
We conducted a multicentric national based study comprising of a cohort of patients hospitalized between 1st of August, 2020 and 31st of December, 2022 in 3 centers in Romania: Clinical Hospital for Children Victor Gomoiu Bucharest, The National Institute of Infectious Diseases Prof. Dr. Matei Bals Bucharest and Emergency Clinical Hospital for Children Brasov. Bucharest, the capital of Romania, has a population of 2,142,300. Clinical Hospital for Children Victor Gomoiu is responsible for consultations and treatment for children in Bucharest and oversees arounnd 30,000 emergency cases every year. The National Institute of Infectious Diseases Prof. Dr. Matei Bals has over 40.000 emergency presentation during an year and it is the referal institute for Romania. Brasov county is located in the central area of Romania and has a population of more than 300.000 inhabitants, according to the latest national survey. The Children’s Clinical Hospital of Brasov is the largest pediatric hospital from this region (more than 200 beds) and serves as a tertiary hospital for 3 neighbor counties. The statistical results were obtain using Microsoft Excel, from the Office 365 package and Matlab R2023b. The statistical analysis was performed with predefined tools, functions and package. The statistical correlation with a p value of less that 0.05 was considered. The Ethical Committee from each of the three hospitals has approved the study. There are 3 definitions for this disease formulated by the Royal College of Paediatrics and Child Health (RCPCH), World Health Organization (WHO) and Centers For Disease Control And Prevention (CDC). We included in our study 80 patients according to World Health Organisation case definition who met all 6 criteria of the following: 1. Children between 0 and 19 years; 2. Fever more than 3 days; 3. Clinical signs of multisystem involvment (at least 2 of the following): rash, bilateral nonpurulent conjunctivitis, mucocutaneous inflammation signs (oral, hands or feet), hypotension or shock, cardiac dysfunction, pericarditis, valvulitis, coronary abnormalities (including echocardiographic findings or elevated troponin/BNP), evidence of coagulopathy (prolonged PT or PTT, elevated D-dimer), acute gastrointestinal symptoms (diarrhea, vomiting or abdominal pain); 4. Elevated inflammation markers, including any of the following: ESR/CRP/procalcitonin; 5. Evidence of SARS-CoV2 infection - any of the following: Possitive SARS-Cov2 RT-PCR/Positive serology/Positive antigen test/Contact with an individual with COVID-19; 6. No other obvious microbial cause of inflammation including bacterial sepsis and staphylococcal/streptococcal toxic shock syndrome [7].
Additional relevant information
We compared patients demographic characteristics (age, gender, comorbidities), symptoms of presentation (fever, hiperemic conjunctivitis, adenopathy, gastro-intestinal, respiratory, neurological, muco-cutaneous), lab results (PCR SARS-COV2, Ag. SARS-COV2, C-reactive protein, ESR, fibrinogen, ferritin, procalcitonin, Lactat Dehydrogenase (LDH), hemoglobin, white blood cells, lymphocytes, neutrophyles, platelete, D-dimeri, troponin, NT-proBNP, coagulation status, sodium, calcium, potasium, urea, creatinin, uric acid, aminotransferases, albumin, glucose, faringian and nasal swab, cultures), EKG, cardiac assesment and treatment.
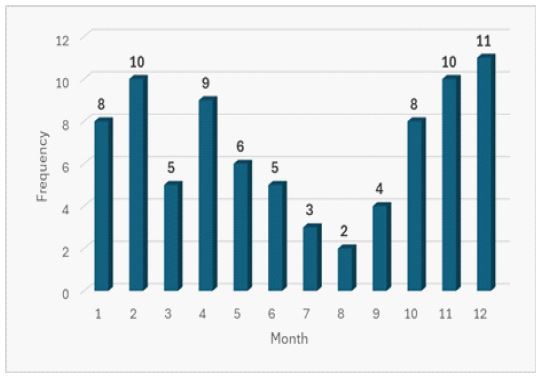
Table 1: Symptoms found at presentations.
| Characteristics | No.(%) |
|---|---|
| Mean age (years) | 5.05 |
| Males/Females | 55/25(68,75%/31,25%) |
| Urban area/Rual area | 46/34(57,5%/42,5%) |
| Known SARS-CoV2 infection | 14 (17,5%) |
| Fever | 78 (97,5%) |
| Pharingeal hyperemia | 61 (76,2%) |
| Skin rash | 38 (47,5%) |
| Hyperemic conjunctivitis | 33 (41,2%) |
| Gastrointestinal manifestations | 53 (66,2%) |
| Abdominal pain | 24 (30%) |
| Vomiting | 27 (33,75%) |
| Nausea | 19 (23,75) |
| Stool modifications | 22 (27,5%) |
| Respiratory manifestations | 38 (47.5%) |
| Couch | 35 (43,75) |
| Pulmonary rales | 12 (15%) |
| Respiratory distress | 9 (11,25) |
| Cardiovascular manifestations | 18 (22,5%) |
| Heart rate | 18 (22,5%) |
| Neurological symptoms | 20 (25%) |
| Headache | 16 (20%) |
| Signs of meningism | 5 (6,25) |
| Altered mental status | 2 (2,5%) |
| Paresthesia | 1 (1.25%) |
| Myalgias | 5 (6,25%) |
Inflammatory markers were found in all patients with higher median value in older children. In patients younger than 1 year median values were: 51,27 mg/dl for C-reactive protein (NV 0-1), 206,57 microg/l for ferritin (NV 10-120), 60,61 mm/1h for eritrocyte sedimentation rate and 317,51 U/l for Lactat Dehydrogenase (LDH) (NV 135-225). In contrast, in the group with patients over 10 years, the median values were significantly higher for C reactive protein (121,72 mg/dl), and ferritin (849,63 microg/l) but lower for eritrocyte sedimentation rate (36,66 mm/1h).
We found a significant p-value for CRP between the group of patients with less than 1 year and the group of patients between 1 and 5 years (p=0.04), for ferritin between the group of pacients between 1 and 5 years and the group of patients with greater that 10 years (p< 0.01) and for D-dimer between the patients between 1 to 5 years and the group of patients with age greater that 10 years (p< 0.02). We also demonstrated a statistical correlation between days of hospitalization and high levels of CRP (p< 0.005) and ferritin (p=0.003). Complete blood count shows, out of 80 patients, higher values of leukocytes in 37 patients (NV 4500-13000/microL) with lower values of lymphocytes in 25 patients (NV 1500-6500/microL). Anemia was found in 42 patients (NV of Hemoglobin 11,7-16,6 g/dl). We also found high values of cardiac enzyme (troponin and NT proBNP) in the group with patients over 10 years old. Coagulation markers were high in all 4 groups such as D-dimer that were higher than normal range in 36 patients with a median value of 2,98 microg/l (NV< 0,5) and fibrinogen with a median value of 505,97 mg/dl (VN 160-450 mg/dl). Beside inflammatory and coagulation markers there was also an electrolyte imbalance in a few pacients: 1 patients with hypernatremia (NV 136-145 mmol/l), 6 patients with hyperkalemia (NV 3,5-5 mmol/l) and 4 patients with hyperchloremia (NV 90-106 mmol/l). Hepatic enzymes were also higher than normal in 16 patients out of 80 (20%) (VN ALT< 40U/l; AST< 37U/l).
Treatment in more than half of the patients was with imunoglobulin IV (48/80; 60%) and nearly all received corticoterapy (75/80; 93,75%). Also 77 patients out of 80 (96,25%) were treated with antibiotics. Other teatments such as anticoagulation therapy was administered in 32 patients (40%) of which only 19 patients (23,75%) had d-dimer values higher than normal. Other treatments that were administered were: at one patient antiviral therapy, 2 patients had received antiedematous therapy (mannitol), 4 patients albumin and other 2 patients antifungal therapy.
Results
We divided the patients into 4 groups based on age: under 1 year with 6 pacients, 1 to 5 years with 37 pacients, 5 to 10 years with 26 pacients and over 10 years with 11 pacients. We found a mean age of 5.05 years. We analized the number of cases in each month of the years between 2020 and 2022 and we found more patients presenting at the emergency department in the period from September to February, with a peak in April also demonstrating the normal course of an infectious disease often described as multiple waves during the epidemic period characterized of an increase in casese number.
Most common symptom is fever (78/80; 97,5%) followed by pharingeal hyperemia (61/80; 76,2%). Symptoms similar to Kawasaki disease, such as rash (38/80; 47,5%) and hyperemic conjunctivitis (33/80; 41,2) also occured. Gastrointestinal symptoms were as follow: loss of appetite (37/80; 46,25%), abdominal pain (24/80; 30%), vomiting (27/80; 33,75%), nausea (19/80; 23,75%) and stool abnormalities (22/80; 27,5%). The most common respiratory symptom was cough (35/80; 43,75%), followed by pulmonary rales (12/80; 15%) and respiratory distress (9/80; 11,25%). Cardiovascular manifestation were found: changes in heart rate (bradycardia or tachycardia) (18/80; 22,5%). Some of the patients had neurological symptoms: headache (16/80; 20%), signs of meningism with neck stiffness (5/80; 6,25%), altered mental status (2/80; 2,5%) and paresthesia (1/80; 1,25%).
Table 2: Mean values of laboratory result.
| Laboratory findings | Under 1 year | 1-5 years | 5-10 years | Above 10 years |
|---|---|---|---|---|
| CRP (mg/dl) | 53.78 | 52.24 | 88.23 | 112.79 |
| Ferritin (microg/l) | 173.9 | 277.99 | 531.58 | 742.68 |
| ESR (mm/1h) | 69,33 | 51,56 | 45.64 | 38 |
| Lactat dehydrogenase (U/l) | 318.81 | 305,01 | 276,98 | 297,18 |
| NT proBNP | 2202.26 | 1867.3 | 1616.14 | 6512.49 |
| D-dimer (mg/dl) | 6.32 | 2.17 | 3.6 | 2.2 |
| Fibrinogen | 463,16 | 523.04 | 484.43 | 522.82 |
| Natremia | 136 | 136,2 | 136,7 | 137,18 |
| AST | 36,83 | 41.36 | 36.53 | 43.82 |
| ALT | 27,66 | 41.36 | 68.14 | 46.92 |
We found a significant p-value for CRP between the group of patients with less than 1 year and the group of patients between 1 and 5 years (p=0.04), for ferritin between the group of pacients between 1 and 5 years and the group of patients with greater that 10 years (p< 0.01) and for D-dimer between the patients between 1 to 5 years and the group of patients with age greater that 10 years (p< 0.02). We also demonstrated a statistical correlation between days of hospitalization and high levels of CRP (p< 0.005) and ferritin (p=0.003). Complete blood count shows, out of 80 patients, higher values of leukocytes in 37 patients (NV 4500-13000/microL) with lower values of lymphocytes in 25 patients (NV 1500-6500/microL). Anemia was found in 42 patients (NV of Hemoglobin 11,7-16,6 g/dl). We also found high values of cardiac enzyme (troponin and NT proBNP) in the group with patients over 10 years old. Coagulation markers were high in all 4 groups such as D-dimer that were higher than normal range in 36 patients with a median value of 2,98 microg/l (NV<0,5) and fibrinogen with a median value of 505,97 mg/dl (VN 160-450 mg/dl). Beside inflammatory and coagulation markers there was also an electrolyte imbalance in a few pacients: 1 patients with hypernatremia (NV 136-145 mmol/l), 6 patients with hyperkalemia (NV 3,5-5 mmol/l) and 4 patients with hyperchloremia (NV 90-106 mmol/l). Hepatic enzymes were also higher than normal in 16 patients out of 80 (20%) (VN ALT<40U/l; AST<37U/l).
Treatment in more than half of the patients was with imunoglobulin IV (48/80; 60%) and nearly all received corticoterapy (75/80; 93,75%). Also 77 patients out of 80 (96,25%) were treated with antibiotics. Other teatments such as anticoagulation therapy was administered in 32 patients (40%) of which only 19 patients (23,75%) had d-dimer values higher than normal. Other treatments that were administered were: at one patient antiviral therapy, 2 patients had received antiedematous therapy (mannitol), 4 patients albumin and other 2 patients antifungal therapy.
Discussion
To the best of our knowledge this is the first study for Romania regarding MIS-C comprising three different hospitals in our country. The mean age of 5.05 years was lower than in studies from Unites States that showed a median age of 7.3-10.8 years or studies from Italy with a mean age of 7.54 years. In our study we observed that more patients were in the group of 1 to 5 years (37 patients) followed by the group of 5 to 10 years (26 patients) [8,9]. Less patients were found in the other two groups: 6 patients with less that 1 year and 11 patients with more that 10 years. Studies made in Italy and the one made by Dufort in Unites States observed a higher incidence in children between 5 and 10 years [8,9]. We highlighted the high incidence of the disease in late fall and winter similar to the study from Italy that showed a higher incidence in December, February, March and April. Only 17 of our patients (17,5%) had a positive history of SARS-Cov2 infection, demonstrating the reduced severity of the disease in children and also providing an explanation why many of them were not tested [8]. Compared to published data, we found in our study similar results according to the symptoms, with 66.2% of cases presenting with gastrointestinal problems, 95% with mucocutaneous findings (pharyngeal hyperemia, conjunctivitis and rash) and 47.5% presenting with respiratory symptoms. The most frequently encountered symptoms in our study in children with MIS-C were fever, and pharyngeal hyperemia with 97.5%, respectively 76.2% [10]. Neurological symptoms (headache, altered mental status, paresthezia and meningism) were found in 20 patients out of 80. Published articles pointed out that around 50% of cases presented with headache, which is more than what we found in our study. Also, in our study we did not find any patient with encephalopathy nor with seizures. Compared with published data where neurological involvement does not determine a severe outcome, our study describes a statistical correlation between neurological symptoms at presentation and number of hospitalization days [11]. (p< 0.005 for headache, p=0.02 for altered metal status, p=0.03 for paresthesia, p=0.02 for signs of meningism) [12]. Lymphopenia is frequently found. It is demonstrated that its levels are correlated with severity and mortality of MIS-C. Interleukine-6, an inflammation marker, may trigger massive death of lymphocytes [13]. Lower levels of lymphocytes are a result of low levels of both CD4+ and CD8+ cells. In our study we found low levels of lymphocytes in 25 cases out of 80 (31,25%) and were correlated with prolonged hospitalziation (p=0.01). Our study highlights the differences in median value of the inflammatory markers between the 4 study groups with higher values in the older children, demonstrating a milder inflammatory respons in younger children. Several published studies underlined that higher values of inflammatory markers are correlated with severity of the disease. We demonstrated no difference in CRP values between the first two groups of patients (less than 1 year and 1 to 5 year) and no difference between the second group (1 to 5 years) and the last group (more than 10 years) for Ferritin and D-dimeri [14]. Overall high values of CRP and Ferritin may indicate a longer and more sever evolution of the disease in our children and they were correleted with more days of hospitalization. Differential diagnosis of MIS-C with other diseases such as macrophage activation syndrome toxic shock syndrome and Kawasaki disease is very difficult due to the fact that clinical findings are very similar. We found in our study a higher mean age of presentation compared to non- COVID-19 KD cases (median age 2.0-2.7y) [15,16]. Considering the unpredictable evolution of the disease and the limited data about the long-term sequelae, practitioners must follow several protocols and choose the beneficial strategy for each individual patient. Numerous guidelines have been developed to help in the management of the disease. All these guidelines recommend the use of Intravenous Immunoglobulins (IVIg) with a dose of 2 g/kg/dose as first line treatment. Because of the increased dose of IVIG that is require the pacients are at risk of developing hemolytic anemia and volume overload [3]. In our study more than a half received imunoglobulin with no adverse effects. Corticosteroids are also frequently recommended especially in patients with shock or organ-threatening disease. In published literature we find that corticosteroids were used after IvIg administration in those patients that did not respond to treatment. In our study 60% of the patients received both therapies from the beginning of the hospitalization and 25 patients received only corticosteroids without IVIg. After evaluating the coagulation factors, a small dose of aspirin may be used prophylactically, especially in patients who develop symptoms similar to Kawasaki disease. Some guidelines such as AAP or Children’s Hospital and Clinics of Minnesota also add antibiotics to the treatment (vancomycin, ceftriaxone or clindamycin). Our study showed an incresed use of antibiotics, although the etiology is considered to be a viral one, but we deescalade the antibiotic usage [3,7]. Guidelines recomand antibiotic discontinuation in patients with negative cultures and no signs of bacterial infection.
Limitations
Our study has several limitations. The number of enrolled patients was relatively small. We could not analyze the long term outcome of the patients due to the retrospective nature of the study and also because parents did not come back as requested for the follow up of their children. Finally, regarding treatment there was no reevaluation of antibiotic therapy, the patients receiving it in almost all cases.
Conclusion
To the best of our knowledge this is the first multicenter study regarding MIS-C in our country. We demonstrated the similarities and differences between our patients and published data and we highlighted the importance of knowing possible evolution of the disease in order to choose the best treatment plan. We also demonstrated the markers that can predict a longer and more severe evolution of the disease.
Declarations
Competing interests: None to declare.
Funding statement: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
- Martin B, DeWitt PE, Russell S, et al. Characteristics, Outcomes, and Severity Risk Factors Associated With SARS-CoV-2 Infection Among Children in the US National COVID Cohort Collaborative. 2022; 5(2): 2143151. doi: 10.1001/jamanetworkopen.2021.43151.
- COVID 19 Weekly surveillance report. 2022.
- Algarni AS, Alamri NM, Khayat NZ, et al. Clinical practice guidelines in multisystem inflammatory syndrome (MIS-C) related to COVID-19: A critical review and recommendations. 2022; 18(2): 83-90. doi: 10.1007/s12519-021-00499-w. Epub 2022 Jan 4.
- Bar-Meir M, Guri A, Godfrey ME, et al. Characterizing the differences between multisystem inflammatory syndrome in children and Kawasaki disease. Sci Rep. 2021; 11(1): 13840. doi: 10.1038/s41598-021-93389-0.
- Yonker LM, Gilboa T, Ogata AF, et al. Multisystem inflammatory syndrome in children is driven by zonulin-dependent loss of gut mucosal barrier. 2021; 131(14): 149633. doi: 10.1172/JCI149633.
- Godfred-Cato S, Abrams JY, Balachandran N, et al. Distinguishing Multisystem Inflammatory Syndrome in Children From COVID-19, Kawasaki Disease and Toxic Shock Syndrome. 2022; 41(4): 315-323. doi: 10.1097/INF.0000000000003449.
- Henderson LA, Canna SW, Friedman KG, et al. American College of Rheumatology Clinical Guidance for Multisystem Inflammatory Syndrome in Children Associated With SARS-CoV-2 and Hyperinflammation in Pediatric COVID-19: Version 1. 2020; 72(11): 1791-1805. doi: 10.1002/art.41454.
- La Torre F, Elicio MP, Monno VA, et al. Incidence and Prevalence of Multisystem Inflammatory Syndrome in Children (MIS-C) in Southern Italy. 2023; 10(5): 766. doi: 10.3390/children10050766.
- Dufort EM, Koumans EH, Chow EJ, et al. New York State and Centers for Disease Control and Prevention Multisystem Inflammatory Syndrome in Children Investigation Team. Multisystem Inflammatory Syndrome in Children in New York State. 2020; 383(4): 347-358. doi: 10.1056/NEJMoa2021756.
- Yasuhara J, Watanabe K, Takagi H, et al. COVID-19 and multisystem inflammatory syndrome in children: A systematic review and meta-analysis. 2021; 56(5): 837-848. doi: 10.1002/ppul.25245.
- Fink EL, Robertson CL, Wainwright MS, et al. Global Consortium Study of Neurologic Dysfunction in COVID-19 (GCS-NeuroCOVID) Investigators. Prevalence and Risk Factors of Neurologic Manifestations in Hospitalized Children Diagnosed with Acute SARS-CoV-2 or MIS-C. 2022; 128: 33-44. doi: 10.1016/j.pediatrneurol.2021.12.010.
- Bova SM, Serafini L, Capetti P, et al. Neurological Involvement in Multisystem Inflammatory Syndrome in Children: Clinical, Electroencephalographic and Magnetic Resonance Imaging Peculiarities and Therapeutic Implications. An Italian Single-Center Experience. 2022; 10: 932208. doi: 10.3389/fped.2022.932208.
- Gowin E, Dworacki G, Siewert B, et al. Immune profile of children diagnosed with multisystem inflammatory syndrome associated with SARS-CoV-2 infection (MIS-C). 2022; 47(2): 151-159. doi: 10.5114/ceji.2022.116385.
- Zhao Y, Yin L, Patel J, et al. The inflammatory markers of multisystem inflammatory syndrome in children (MIS-C) and adolescents associated with COVID-19: A meta-analysis. 2021; 93(7): 4358-4369. doi: 10.1002/jmv.26951.
- Vogel TP, Top KA, Karatzios C, et al. Multisystem inflammatory syndrome in children and adults (MIS-C/A): Case definition & guidelines for data collection, analysis, and presentation of immunization safety data. 2021; 39(22): 3037-3049. doi: 10.1016/j.vaccine.2021.01.054.
- Hoste L, Van Paemel R, Haerynck F. Multisystem inflammatory syndrome in children related to COVID-19: A systematic review. 2021; 180(7): 2019-2034. doi: 10.1007/s00431-021-03993-5.