
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 5
Overexpression of HHLA2 and PD-L1 anticipates weak prognosis in esophageal cancer patients
Fun-Lan Guo1; Peng-Zhi Zhu2; Xiao-Dong Zheng1; Shi-Wei Nie1; Li-Hua Wang1; Ning Zhang1; Yuan-Yuan Ji1; Jin Xia1*
1Anyang Tumor Hospital, The Fourth Affiliated Hospital of Henan University of Science and Technology, Henan Medical key Laboratory of Precise Prevention and Treatment of Esophageal Cancer, Henan Province, Anyang 455000, China.
2Tianjin Hospital, Tianjin 300200, China.
*Corresponding Author : Jin Xia
Anyang Tumor Hospital, The Fourth Affiliated Hospital of Henan University of Science and Technology, Henan Medical key Laboratory of Precise Prevention and Treatment of Esophageal Cancer, Henan Province, Anyang 455000, China.
Email: 15890750990@126.com
Received : Aug 20, 2024
Accepted : Sep 13, 2024
Published : Sep 20, 2024
Archived : www.jcimcr.org
Copyright : © Xia J (2024).
Abstract
Esophageal cancer is one of the most common leading causes of cancer-related mortality worldwide, its incidence has increased particularly in the last few decades in the Western world. Esophageal cancer also has a poor prognosis as it cannot be diagnosed until the advanced stages due to the shortage of early clinical symptoms. The increasing incidence and poor prognosis of esophageal cancer emphasize the necessity for developing the detection and prediction approaches which are important before the medication. Also, only a small percentage of esophageal cancer patients might benefit from the conventional surgery, chemotherapy or current immunotherapy. Therefore, exploring novel immunotherapies or immune checkpoints for improving the pharmacological treatment of esophageal cancer patients is truly required. Here we identify a newly discovered B7 family member and widely expressed in numerous cancers, HHLA2 is also overexpressed in esophageal cancer. The current research intended to investigate the prognostic impact of HHLA2 and PD-L1 expression on esophageal cancer patients and its association with CD8 expression (tumor-infiltrating lymphocytes). The protein levels of HHLA2, PD-L1, and CD8 in tissues from 69 patients with surgically resectable primary esophageal cancer were detected using immunohistochemistry technique. We found the positive rates of high-HHLA2 expression in tumor were much higher than in adjacent noncancerous tissues of esophageal cancer. Also, the high-HHLA2 expression was associated with smoking but not with necrosis, depth of invasion, lymph node metastasis, distant metastasis, TNM stage and there was no significant difference with the Overall Survival (OS). Besides, high HHLA2 expression was strongly correlated with high PD-L1 and low CD8 expression. In conclusion, the expression of HHLA2 and PD-L1 are frequent in esophageal cancer. High expression of HHLA2 and PD-L1 results in poor prognoses of esophageal cancer, which suggests that HHLA2 may be an important checkpoint and provides a rationale predication and detection for patients with esophageal cancer.
Keywords: Human endogenous retrovirus-H long terminal repeat associating protein 2 (HHLA2); Esophageal cancer; Programmed death 1 ligand 1 (PD-L1); Prognosis; Checkpoint.
Citation: Fun-Lan G, Peng-Zhi Z, Xiao-Dong Z, Shi-Wei N, Xia J, et al. Overexpression of HHLA2 and PD-L1 anticipates weak prognosis in esophageal cancer patients. J Clin Images Med Case Rep. 2024; 5(9): 3261.
Introduction
Its known to us all that esophageal cancer represents as one of the most terrible malignancies internationally, which accounts for 1.1% (20640/ 1918030) of the USA cancer burden in 2022 [1]. World Health Organization has estimated the new cases of esophageal cancer is approximately 324,000 cases in China, which approximately accounts for half of the total cases worldwide. Meahwhile, 90% of esophageal cancer patients are esophageal squamous cell carcinoma in China, whereas in western countries esophageal adenocarcinoma occurrence is the most common [2]. Likewise, in the current study 69 esophageal cancer cases are esophageal squamous cell carcinoma, which were diagnosed by a professional clinical pathologist. In addition, nearly 75% of the patients have developed advanced stage or associated with distant metastasis. Various types of esophageal cancer have significant differences in genetic background, pathogenesis, pathological typing, diagnosis and treatment. The incidence of esophageal cancer has increased significantly in the Western world and it varies considerably across the globe [3]. Exploring potential risk factors may have an influential impact on the incidence of esophageal cancer, among which only about 5% of patients diagnosed with esophageal adenocarcinoma. Esophageal cancer is one of the primary causes of cancer inducing death, approximately 16510 of the 20640 clinical cases in relation with cancer are estimated as new esophageal cancer cases (80.0%) and 20640 of the 983160 whole cancer cases (20.1%), approximately 13250 of the 16410 esophageal cancer deaths (80.07%) and 13250 of the 322090 whole cancer deaths (4%) are expected to occur in 2022 [1]. Currently, the standard first-line therapy for advanced or metastatic esophageal squamous cell carcinoma is chemotherapy or camrelizumab (an anti-programmed death receptor 1 [PD-1] antibody, or camrelizumab in combination with chemotherapy [2]. Therefore, there is a necessity to expand the therapy of clinical patients with esophageal cancer. It’s still extremely poor of the overall 5-year survival rates (~10%) and 5-year post-esophagectomy survival rates (~15-40%) [4]. The main reason of poor outcomes of esophageal cancer patients is the high rates of recurrence or metastasis. Therefore, it is clinical necessary to develop new approaches to improve the adverse clinical consequences in esophageal cancer. Since the last century the immune checkpoints have received significant attention in the pharmacological therapies, which have been recognized as critical mediators affecting occurrence development, prognosis, and clinical immune response of the disease [5-7]. Including facilitation of tumor immune escape and increasing the invasion of suppressive immune cells. Nowadays 25 inhibitory immune checkpoints have been explored and used to predict spontaneous tumor reversion and immune checkpoint blockade responses [8]. Abnormally high expression of inhibitory immune checkpoints like PD-L1, PD-1, PD-L2, B7-H3, CD155, CTLA-4 and TIGIT was considered to be correlated with worse overall survival in patient. Though one comprehensive study has detected the clinical responses of esophageal cancer patients to immune checkpoint blockade [9], which evaluated a novel approach of using a checkpoint inhibitor CheckMate 577 as adjuvant treatment after neoadjuvant chemoradiotherapy and surgery for esophageal, while adverse events like atigue, diarrhea, pruritus, and rash still took place in patients receiving nivolumab and diarrhea and fatigue in those receiving placebo. Although ICIS have been approved and integrated into the therapeutic process for DMMR/MSI-H metastatic colorectal cancer, their role is evolving even as first-line therapy. Universal screening for MSI status by a combination of PCR-and IHC-based methods in all patients diagnosed with metastatic colorectal cancer, testing of approved and non-approved ICIS in combination with chemotherapy, targeted therapy, or other immunotherapeutic agents to enhance immune responses and therapeutic efficacy in two subtypes of metastatic colorectal cancer is currently underway, while, upcoming data are expected to integrate ICIs more substantively into the management of CRC disease, providing additional non-biomarker-related indications for the late and early stages [10]. 408/2000 Despite the unprecedented success of Immune Checkpoint Inhibitors (ICIS) as anticancer therapies, additional mechanisms to determine the efficacy of ICI treatment and potential resistance remain a widespread clinical need, with studies suggesting that, pablizumab or nablizumab in combination with chemotherapy is approved as first-line treatment for apoptotic process ligand 1(PD-L1)-expressing Esophageal Squamous-Cell Carcinoma (ESCC), and therefore, the FDA approved the protocol regardless of PD-L1 expression. The superiority of programmed death 1(PD-1) antibody in combination with chemotherapy over chemotherapy alone remains controversial in ESCC patients with low expression of PD-L1 [11]. Human endogenous retrovirus subfamily H long terminal repeat associating protein 2 (HHLA2, also known as B7H5 and B7H7) is a frequently found member of the B7 family and similar checkpoint as PD-L1, PD-L2 and B7-H3 [12]. Numerous research has demonstrated that HHLA2 was over-expression in various types of carcinoma such as clear cell renal cell carcinoma, lung cancer, gastric cancer, hepatocellular carcinoma, osteosarcoma, bladder urothelial cancer and ovarian cancer, which is in relation with poor prognosis and poor overall survival [13-19]. However, a recent study evaluated the expression of HHLA2 in solid tumors with a meta-analysis on account of the Chinese population and found that high expression of HHLA2 protein was associated only with poor OS in patients with clear cell renal cell carcinoma, gastric cancer, intrahepatic cholangio-carcinoma and lung cancer, but not with epithelial ovarian cancer patients [19]. Nevertheless, high HHLA2 protein level was in relation with enhanced overall survival in pancreatic ductal adenocarcinoma patients [20]. So, the impact of HHLA2 expression on the prognosis of human cancers remains controversial. Over-expression of HHLA2 in patients’ tissues with cancer has been studied to be in relation with the cancer development and malignant characteristics, whereas knockout of HHLA2 could inhibit non-small cell lung cancer cell development, migration, invasion and M2 macrophage polarization of TAMs via downregulating IL-10 levels [21]. However, the biological characters of HHLA2 in human esophageal cancer have not been fully understood though one recent study reported HHLA2 and ICOSLG were combined to foresee survival and immune structures in esophageal squamous cell carcinoma [22]. HHLA2 was reported to stimulate tumor proliferation by affecting the immunity responses of immune cells in tumor microenvironment. Both high expression of HHLA2 and PD-L1 affect prognosis in clear cell renal cell carcinoma patients as individuals with high HHLA2/PD-L1 expression suffered of the highest risk of disease development and death by a significant phenomenon, which is in relation with the high concentration of CD8+ and CD4+ TILs in the tumor microenvironment [13]. A recent study demonstrated that higher HHLA2 expression promotes immune evasion by boosting M2 polarization and chemotactic migration of macrophages mainly through IFNG/IFR1/HHLA2 axis in hepatocellular carcinoma [23]. Besides, HHLA2 engagement could recruit KIR3DL3 to the immunological synapse and work together to block the function of CD8+ T and NK cells and stimulating the immune-evasive HHLA2+ tumors [24]. In addition, a recent study found overexpression of HHLA2 blocked the proliferation and predicted improved survival in ovarian cancer by affecting the tumor differentiation and high CD8+ TIL levels [19]. However, the relationship between HHLA2, specific CD8+ T cell phenotypes and the cancer prognosis deserves further research. Immune checkpoints correlated complicatedly with the tumor microenvironment. However, no reports have been conducted to uncover their comprehensive parts in the tumor microenvironment of esophageal cancer patients. Here in this research, we were aiming at demonstrating the prognostic impact of HHLA2 and PD-L1 expression in tumor and adjacent noncancerous tissues. We also intended to explore how HHLA2 and PD-L1 influence affects immunological features in esophageal cancer patients. Additionally, we assessed the relationship between the expression of HHLA2, PD-L1, CD8 and the clinic-pathological features by analyzing data from a cohort with 69 patients mainly with esophageal squamous cell carcinoma using the immunohistochemistry technique, on a condition that is a primary foundation for finding new immunotherapeutic targets for esophageal cancer.
Materials and methods
Patients and samples: 69 esophageal squamous cell carcinoma samples and associated adjacent noncancerous tissues with patients’ basic parameters and overall survival information were obtained from the Department of Pathology, Anyang Tumor Hospital, The Fourth Affiliated Hospital of Henan University of Science and Technology with the informed consent and the approval from the Institutional Ethics Committee of Anyang Tumor Hospital. The Fourth Affiliated Hospital of Henan University of Science and Technology [the ethical approval number: AZLL022020050200116]. Patients in the cohort undertook surgical resection for esophageal cancer from September 2017 to October 2020. In addition, each participant or his/her legal guardians was informed and agreed with the purpose of the study that their personal case details to be published and signed informed consent before participation which showed in the supplementary files. The tissues were collected, fixed with formalin and embedded with paraffin by the pathology department of the hospital. Two professional pathologists were assigned to confirm each patient’s pathological features including the depth of invasion (T), lymph node metastasis (N), TNM stage through H&E dyeing tumor slides, according to the American Joint Committee On Cancer (AJCC) 2010 TNM classification for esophageal cancer. All specimens were confirmed as esophageal squamous cell carcinoma by pathology. Distant metastasis was evaluated by imaging examination. The overall survival of patients was defined as time span from the date of surgery to the date of death. And the data obtained for this study was obtained prospectively.
Immunohistochemistry: The protein levels of HHLA2, PD-L1 and CD8 were detected using the Immunohistochemistry (IHC) staining method, which was conducted by a professional pathologist according to the previous studies [25,26]. Briefly, the 4 μM-thick sample sections were incubated with primary antibodies including anti-HHLA2 (Abcam, ab 214327), anti-PD-L1 (cell signaling technology, CST #13684), anti-CD8 (CST, #85336) at 4°C overnight after deparaffinization, rehydration, antigen retrieval, endogenous peroxidase inactivation with corresponding reagents and followed with blocking non-specific binding blocked with 5% bovine serum albumin [27]. Subsequently, the slides were washed three times with PBS and was incubated with the corresponding secondary antibodies and visualized using a DAKO EnVision Detection System (Dako). The slides were cover-slipped by the clean cover glasses after counterstained with hematoxylin.
Immunohistochemistry analysis: 10 random visual fields close to the center of each tissue at 100×, 400× magnification was observed and captured under the microscopy, and the immunostaining images were assessed by two different investigators in a double-blinded fashion. The protein level of HHLA2, PD-L1 and CD8 was recorded with H-score in a semi-quantitation method according to the Area of Positivity (AP) and the Intensity of Staining (IS). Area of positivity is closely correlated with the percentage of positive stained cells. The staining intensity was determined according to the following rules: 1) point denoted as weak intensity; 2) points as moderate intensity i; 3) points as strong intensity. The percentage of positive cells was calculated as follows: 1 points as 0~25%; 2 points as 26~50%; 3 points as 51~75%; 4 points as 76~100%. The expression of HHLA2, PD-L1 and CD8 was scored as the product of staining intensity multiplied by the percentage of stained cells. Based on the final scores, specimens were categorized into negative (-), ≤5% cells were stained, regardless of intensity; weak (+), 1~4 points; moderate (++), 5~8 points; and strong (+++), 9~12 points. For the following statistical analysis, the negative and weak groups (- and +) were considered to be HHLA2, PD-L1 and CD8 low expression and the moderate and strong groups (++ and +++) were considered to be HHLA2, PD-L1 and CD8 high expression. Overall, the final H-score was calculated by the following equation: H-score = AP×IS. Additionally, the number of positive cells was counted in each core of esophageal cancer for the CD8 evaluation. The cutoff point of high or low expression was determined on the median of total scores.
Statistical analysis
All statistical analysis was performed using SPSS V.24.0 software or Graphpad Prism 7 software (La Jolla, California, USA). p value < 0.05 was considered statistically significant for the groups that compared with each other. Patients with clinical outcomes were separated into two groups based on the mean level of HHLA2 protein expression. Log-rank test was used to measure the statistical difference between the high HHLA2 and low HHLA2 groups for Kaplan-Meier curves. The correlation analyses were performed using the X2 test or Fisher exact test. The Kaplan-Meier method was applied to assess the effect of HHLA2, PD-L1 and CD8 overexpression on the esophageal cancer patient survival and the significance was evaluated by the log-rank test. Student’s t-test was conducted to determine the association between CD8 T-cell counts and HHLA2 expression. Variables with p< 0.05 of the univariate analysis were combined into multivariate survival analysis by employing the Cox proportional hazards model.
Results
Baseline characteristics of patients: Amid the 69 esophageal cancer patients, 44 (63.8%) patients were male and 25 (36.2%) patients were female, and most of the patients 61 (88.4%) were above 60 years and only 8 patients (11.6%) were below 60 years of age. At the end of follow-up, 22 (31.9%) patients died and 47 (68.1%) patients survived. Out of 69 patients, 22 (31.9%) and 6 (8.7%) patients have a history of smoking and alcohol consumption, respectively. According to the depth of tumor invasion, 31 (44.9%) were T2, 36 (52.2%) were T3, and 2 (2.9%) was T4. For the lymph node metastasis, 48 (69.6%) were N0, 11 (15.9%) were N1, and 10(14.5%) were N2. Furthermore, 19 (27.5%) patients were classified as Stage I, 31 (45.0%) as Stage II, and 19 (27.5%) as Stage III according to the 8th AJCC staging system (Table 1) of esophageal cancer. Meanwhile, the baseline of patient clinic-pathological characteristics of the esophageal cancer cohort is listed in the (Table 1). As illustrated in Table S1, the average age for surgery was 65 years (ranging from 49 to 81 years). At the end of follow-up 31.9% (22/69) patients died from esophageal cancer. The median OS time was 38 months (ranging from 1 to 45 months).
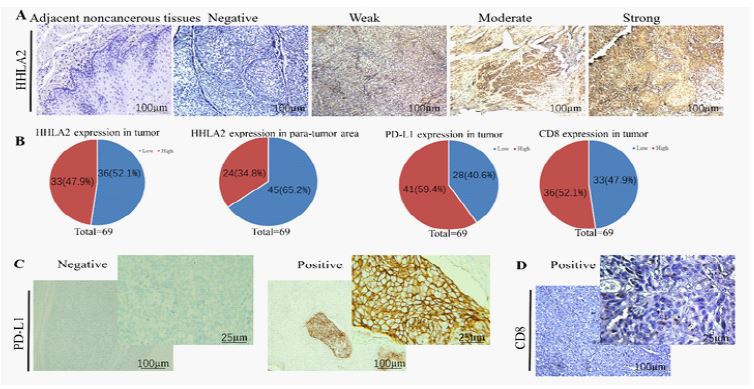
Expression pattern of HHLA2 and PD-L1 in esophageal cancer: Representative Immunohistochemistry (IHC) photomicrographs for HHLA2, PD-L1 and CD8 in esophageal cancer were depicted in (Figure 1). Typical microphotographs of PD-L1 expression were shown in (Figure 1A) as shown in (Figure 1B), the positive rates of high HHLA2 expression 47.9% (33/69) in the tumor tissue, which is significantly higher compared to the HHLA2 expression in para-tumor area with 34.8% (24/69). In the meantime the positive rates of high PD-L1, CD8 expression were 59.4% (41/69) and 52.1% (36/69), respectively in the tumor tissue. As shown in (Figure 1A and S1), the increase in HHLA2 expression was observed in esophageal cancer tissues. A high HHLA2 staining was observed in esophageal cancer compared to para-tumor, which mostly overlap cytoplasm and tumor cells membrane (Figure 1A), our results are highly consistent with previous reports such as cholangio carcinoma, epithelial ovarian cancer and hepatocellular carcinoma [19-29]. The level of HHLA2 protein expression in esophageal cancer tissue and para-tumor tissues obtained from 69 patients with esophageal cancer surgically operated between 2017 and 2019 was examined, and graded as follows: absent staining, weak staining, moderate staining, and strong staining (Figure 1A). Meanwhile, The H-score of HHLA2 ranged from 2.0 to 12.0 and with a median score9.0. The median score was used to determine the cutoff value of high or low HHLA2 expression level. A H-score >9.0 was defined as a high HHLA2 expression, while H-score ≤9.0 indicated low HHLA2 expression. In the current study, 47.9% (33/69) esophageal cancer tissues show the high positive rate of HHLA2 expression, which is in accordance with the previously published studies, with 47.6% in colorectal cancer [30], 50% in clear cell renal cell carcinoma[31] and 56% in triple-negative breast cancer [32]. Recently, B7 family member reported the high expression level of PD-L1 in many murine and human cancers. In addition to cancer cells, PD-L1 was also commonly expressed in multiple types of host cells in the tumor microenvironment and lymph nodes, including dendritic cells, macrophages, fibroblasts, and T cells, in order to reduce anti-tumor immunity and PD-L1 has been reported to decrease TCR-mediated proliferation and cytokine secretion [33]. Typical microphotographs of PD-L1 expression of the esophageal cancer were showed in Figure 1C, the stained area was highly colocalized with tumor cells membrane, which is consistence with the previous reports that PD-L1 is a class I transmembrane protein with a transmembrane hydrophobic region and an intracellular region. Similar to HHLA2, the median score was used to determine the cutoff value of high or low PD-L1 expression level. A H-score >9.0 was defined as high PD-L1 expression, and H-score ≤ 9.0 indicated low PD-L1 expression. In 69 esophageal cancer tissues, the high expression of PD-L1 was 59.4% (41/69) (Figure 1B), which is significantly higher compared to the low expression of PD-L1 with 40.6% (28/69) in cancer tissue. So, the positive rate of PD-L1 is higher in the esophageal cancer compared to para-tumor tissues as shown in the supplementary excel table with the Raw data.
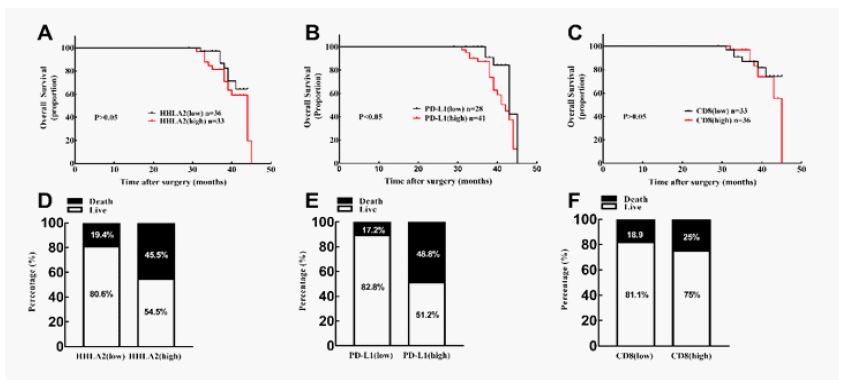
Next, we also checked the CD8 expression in both esophageal cancer tissues and para-tumor tissues with immunohistochemistry staining method. The mean and median value of CD8 T-cell numbers was 362.3 and 244.0, respectively (range 100-1,830). A CD8 T-cell count >244.0 was considered as a positive, and counts ≤244.0 was negative according the reported method [30]. CD8 was positive at the cellular membrane of cytotoxic T lymphocytes as shown in (Figure 1D), among 69 patients with esophageal cancer, the CD8 positive was 52.1% (36/69) (Figure 1B), which is slightly more than the CD8 negative with 47.9% (33/69) in cancer tissues. Expression of HHLA2 in esophageal cancer patients and clinic-pathological variables. The relationship between HHLA2 expression and clinic-pathological parameters in esophageal cancer was tested by χ2 test. As shown in Table 2, significant correlation was found between the smoking and HHLA2 expression (P=0.021), whereas HHLA2 expression was not significantly associated with age, gender, depth of invasion (T), lymph node metastasis (N), TNM stage, demographics and alcohol history in patients with esophageal cancer. Relationship between HHLA2, PD-L1 expression and CD8 T-cell infiltration in esophageal cancer The results of χ2 test illustrated that HHLA2 expression was correlated with CD8 T-cell infiltration (P=0.000, Table 2), PD-L1 (P=0.006, Table 2) in patients with esophageal cancer. Impact of HHLA2, PD-L1 and CD8 expression on the overall survival. Consequently, the prognostic value of HHLA2, PD-L1 and CD8 expression in esophageal cancer was investigated (supplementary materials S2 and S3). Survival analysis determined by the Kaplan–Meier curve and log-rank test demonstrated that high expression of PD-L1 predicted poor survival and high mortality rate in patients with esophageal cancer (Figure 2B, P=0.0414<0.05). However, high expression of HHLA2 or high CD8 were found having no significant prognostic value for the overall survival of patients with esophageal cancer (P=0.3095>0.05, Figure 2A; P=0.5440>0.05, Figure 2C). While the IHC staining findings confirmed that esophageal tumor tissues have significantly higher levels of HHLA2 than peritumoral tissues. We classified esophageal cancer patients based on their H-score median value. The median overall survival in the HHLA2-high cohort was little shorter (median 44 months vs undefined, P>0.05; Figure 2A), while the probability of death increased (45.5% vs. 19.4%; Figure 2D). The median overall survival in the PD-L1-high cohort was significantly shorter (median 42 months vs undefined, P< 0.05; Figure 2B), and the probability of death increased (48.8% vs. 17.2%; Figure 2E). The median overall survival in the CD8-high cohort was a little shorter (median 45 months vs undefined, P>0.05; Figure 2C), and the probability of death increased (25% vs. 18.9%; Figure 2F). To explore the prognostic significance of HHLA2, PD-L1 and CD8, univariate and multivariate analyses of the Cox proportional hazard model on overall survival was performed. To determine the prognostic value of HHLA2 expression and other clinic-pathological variables.
Table 1: Patient characteristics (N=69).
| Characteristic | Sub-characteristic | Value (%) |
|---|---|---|
| Age | < 60 | 8 (11.6%) |
| ≥60 | 61 (88.4%) | |
| Gender | Male | 44 (63.8%) |
| Female | 25 (36.2%) | |
| Survival status | Death | 22 (31.9%) |
| Survival | 47 (68.1%) | |
| Depth of invasion(T) | T2 | 31 (44.9%) |
| T3 | 36 (52.2%) | |
| T4 | 2 (2.9%) | |
| Lymph node metastasis(N) | N0 | 48 (69.6%) |
| N1 | 11 (15.9%) | |
| N2 | 10 (14.5%) | |
| TNM stage | Ⅰ | 19 (27.5%) |
| Ⅱ | 31 (45.0%) | |
| Ⅲ | 19 (27.5%) | |
| Smoking history | Yes | 22 (31.9%) |
| No | 47 (68.1%) | |
| Alcohol history | Yes | 6 (8.7%) |
| No | 63 (91.3%) | |
| Demographics | Yes | 39 (56.5%) |
| No | 30 (43.5%) | |
| Total | 69 (100%) |
Table 2: The association of HHLA2 expression level with clinicopathological characteristics in the cohort with esophageal cancer.
| Characteristics | Patients | n | HHLA2 expression | ||
|---|---|---|---|---|---|
| Low [n (%)] | High [n (%)] | p-value | |||
| Gender | Male | 44 | 21 (30.4) | 23 (33.4) | 0.327 |
| Female | 25 | 15 (21.7) | 10 (14.5) | ||
| Age | ≥60 | 61 | 31 (44.9) | 30 (43.5) | 0.712 |
| <60 | 8 | 5 (7.2) | 3 (4.4) | ||
| Infiltration | T1\T2 | 31 | 17 (24.6) | 14 (20.4) | 0.689 |
| T3\T4 | 38 | 19 (27.5) | 19 (27.5) | ||
| LN metastasis | Absent | 48 | 26 (37.7) | 22 (31.9) | 0.616 |
| Present | 21 | 10 (14.5) | 11 (15.9) | ||
| TNM stage | I-II | 50 | 28 (40.6) | 22 (31.9) | 0.302 |
| III-IV | 19 | 8 (11.6) | 11 (15.9) | ||
| Smoking | Present | 22 | 7 (10.1) | 15 (21.7) | 0.021 |
| Absent | 47 | 29 (42.1) | 18 (26.1) | ||
| Alcohol | Present | 6 | 3 (4.3) | 3 (4.4) | 1.000 |
| Absent | 63 | 33 (47.8) | 30 (43.5) | ||
| Demographics | Present | 39 | 19 (27.5) | 20 (29.1) | 0.512 |
| Absent | 30 | 17 (24.6) | 13 (18.8) | ||
| CD8 | Low | 33 | 3 (4.3) | 30 (43.5) | 0.000 |
| High | 36 | 33 (47.8) | 3 (4.4) | ||
| PD-L1 | Low | 28 | 19 (27.5) | 9 (13.1) | 0.006 |
| High | 41 | 14 (20.3) | 27 (38.1) | ||
P values < 0.05 in bold are statistically significant. Analysis were performed using the χ2 test or Fisher exact test with SPSS V.24.0 software. HHLA2: Human Endogenous Retrovirus-H Long Terminal Repeat-Associating Protein 2; LN Metastasis: Lymph Node Metastasis; PD-L1: Programmed Death 1 ligand 1.
Table 3: COX proportional hazard models on overall survival of patients.
| COX proportional hazard models | ||||
|---|---|---|---|---|
| Factors | Univariate analysis | Multivariate analysis | ||
| P-value | HR (95% CI) | P-value | HR (95% CI) | |
| Gender | ||||
| Male vs female | 0.2247 | 0.5706(0.2307-1.411) | ||
| Age | ||||
| <60 vs ≥60 | 0.5895 | 0.7022(0.1944-2.537) | ||
| HHLA2expression | ||||
| Low vs high | 0.3095 | 0.6609(0.2905-1.504) | ||
| PD-L1 expression | ||||
| Low vs high | 0.0414 | 0.4068(0.1814-0.912) | 0.0516 | 1.024(0.384-2.728) |
| CD8 status | ||||
| Low vs high | 0.5440 | 0.7302(0.2651-2.011) | ||
| Depth of invasion(T) | ||||
| T2 vs T3T4 | 0.0491 | 0.396(0.1701-0.922) | 0.0729 | 0.4127(0.1709-0.9964) |
| Lymph node metastasis(N) | ||||
| N0 vs N1,N2 | 0.5765 | 1.302(0.5155-3.29) | ||
| TNM stage | ||||
| I, II vsIII | 0.5241 | 1.31(0.5538-3.1) | ||
| Smoking history | ||||
| Yes vs no | 0.9839 | 0.9918(0.4242-2.319) | ||
| Alcohol history | ||||
| Yes vs no | 0.1079 | 2.55(0.4286-15.17) | ||
| Demographics | ||||
| Yes vs no | 0.1722 | 1.697(0.7317-3.937) | ||
P values < 0.05 in bold are statistically significant. The Kaplan-Meier method and Cox proportional hazards model were applied by using Graphpad Prism 7 software. Of invasion (HR=0.4127, 95% CI=0.1709-0.9964, P=0.0729), were not independent HHLA2 expression showed no significant correlation to the survival of patients with esophageal cancer (HR=0.6609, 95% CI=0.2905-1.504, P=0.3095). Meanwhile, PD-L1 (HR=0.4068, 95% CI=0.1814-0.912, P=0.0414) and depth of invasion (HR=0.396, 95% CI=0.1701-0.922, P=0.0491) were found to be in relation with patients’ survival (Table 3). The independent prognostic value was detected by multivariate analysis (Table 3). The results indicated that PD-L1 (HR=1.024, 95% CI=0.384-2.728, P=0.04516) and depth prognosis factors in the overall survival of patients with esophageal cancer. Moreover, lymph node metastasis(N), TNM stage, and CD8-positive cell-infiltration status, gender, age, smoking history, alcohol history and demographics were not dependent on the overall survival here in our research, either.
Information of supplementary materials:
S1: All patients‘ original information
S2: Original IHC results of HHLA2
S3: Original IHC results of CD8
Discussion
To the best of our knoweledge, this is the first research representing the clinical significance of HHLA2 in esophageal cancer especially the esophageal squamous cell carcinoma, and also demonstrated for the first time that HHLA2 might be an innovative immunosuppressive target in esophageal cancer microenvironment for cancer immunotherapy. The HHLA2 pathway illustrates a novel immune checkpoint blockade in the tumor microenvironment and an attractive factor for clinical cancer therapy during the past several decades. Here, we found that HHLA2 was high expressed in the tumor tissues compared to the adjacent normal tissues in patients with esophageal squamous cell carcinoma. The HHLA2 protein level was statistically correlated with the smoking, PD-L1 level and CD8 T-cell infiltration status. High expression of HHLA2 predicted a high mortality rate compared with the low expression of HHLA2 in esophageal carcinoma patients as shown in the (Figure 2D). The depth of invasion, PD-L1 but not HHLA2 acts as prognostic factor to affect the overall survival of patients with esophageal cancer. Esophageal cancer is known as one of the most horrible malignancies all around the world, with a poor prognosis, high mortality and histrionic incidence growth in the western world taking place over the past several decades. Squamous cell carcinoma and adenocarcinoma present more than 95% of esophageal cancers [34]. The most important risk factors of squamous cell carcinoma and adenocarcinoma are smoking, alcohol use chronic gastroesophageal reflux disease, and obesity [34]. Meanwhile, the general 5-year survival rates remains very poor with 10% overall survival rates, same as the 5-year postesophagectomy with 15~40% overall survival rates [4]. Esophageal cancer is usually diagnosed at an advanced stage because of the lack of early clinical symptoms. The treatment of resectable esophageal cancer has evolved into a multidisciplinary process over the past few decades, and although esophagectomy is still clinically considered the cornerstone of curative treatment for severe esophageal cancer, it is still associated with poor postoperative morbidity and prognosis for patients [35]. The poor prognosis and increasing incidence of esophageal cancer indicates improved prediction and detection methods especially the potential risk factors are essential prior to treatment. However, no research was conducted to prove the specific prevention strategies or recommendations for esophageal cancer screening. Identifying susceptible genes and biomarkers that could predict or identify patients who may or may not respond well to concurrent chemoradiotherapy can contribute physicians in predicting and choosing the appropriate therapy for patients so as to improve their survival rates.
Immune checkpoint blockade treatments such as PD-L1, PD-1, PD-L2, CTLA-4 bring incredible clinical benefits to fighting numerous solid malignancies. However, the function of immune checkpoint factor in esophageal cancer remains debatable. HERV-HLTR-Associating 2 (HHLA2), is a newly recognized B7 family member, has been demonstrated to be widely expressed with positive rates ranging from 0% to 70% in different type of cancers during the past decades [16-32] and associated with poor prognosis in various cancers, such as lung cancer, hepatocellular carcinoma, pancreatic carcinoma, malignant glioma and osteosarcoma [18-37]. Previous studies reported that combination of novel immune checkpoints HHLA2 and ICOSLG could predict survival and immune features and independently identify high-risk patients with esophageal squamous cell carcinoma [22]. However, no such a study was performed that can illustrate the role of HHLA2 in the progression and overall survival of patients with esophageal cancer. Here in this research, we evalauted the protein level of HHLA2 and its clinical significance in 69 esophageal cancer, and we found that the positive rate of high HHLA2 expression in esphageal tumor tissues was over 47%, which is significantly higher than the high HHLA2 expression in the para-tumor area with 34.8%, and the HHLA2 high expression is not statistically correlatted with poor overall survival rate. Moreover, the positive rate of high PD-L1 expression and CD8 was 59.4% and 52.1% respectively. And the high PD-L1 expression was statistically related to poor overall survival of the esophageal cancer patients.The high CD8 expression was correlated with the poor overall survival but not so significantly. Meanwhile, the expression level of HHLA2 was in relation with the smoking, PD-L1 and CD8 T-cell infiltration status. And the high expression level of CD8n in the high expression of HHLA2 group was statistically lower than the low expression of HHLA2 group which is same as previous study, CD8 expression is highly related with CD8 T-cell infiltration status [30]. Although a published research reported that HHLA2 acted as a co-stimulatory role so as to promote cytokine secretion [38], while numerous studies discovered that HHLA2 could inhibit T-cell proliferation and function [39-41], consistantly, our results showed that high expression of HHLA2 is in relation with low expression of CD8, CD8 expression is associated with CD8 T-cell infiltration status, which indicates that HHLA2 may predominantly functions as a T-cell co-inhibitory ligand. The expression level and clinical features of HHLA2 have been well studied in several clinical patients who diagnosed as triple negative breast cancer, osteosarcoma and non-small-cell lung cancer [32-43]. In negative non-small-cell lung cancer cases, 66% cases were HHLA2 positive (413/625), and high expression level of HHLA2 was closely in relation with EGFR mutation and high tumor infiltrating lymphocytes (TILs) density [43]. Research showed that patients with high level of HHLA2 were more probable to develop into advanced and metastatic cancer and HHLA2 was widely expressed in low PD-L1 expression non-small-cell lung cancer specimens [42]. Most normal organs in healthy person do not express HHLA2 except the placenta, gut, gallbladder, and breast whereas HHLA2 is generally overexpressed in several tumor [32,40]. Herein we demonstrated that HHLA2 was expressed in both esophageal tumor specimens and adjucent normal specimens from esophageal cancer patients. However, the IHC results showed that staining intensity of HHLA2 in tumor tissues was stronger than in adjucent normal tissues of esophageal patients, which indicated that HHLA2 is upregulated in tumor tissues of esophageal cancer. Additionally, our results showed the high expression of HHLA2 was in relation with Poor prognosis in patients with esophageal cancer, which is consistent with previous studies in human lung cancer, breast cancer, and osteosarcoma and is closely in ralation with poor prognosis and worse overall survival for clinical patiens [13-19] . In summary, we confirmed that HHLA2 is over expression in patients with esophageal cancer and this is the first reseach reported that HHLA2 is a prognostic checkpoint factor that can affect the overall survival of human esophageal cancer through immunosuppressive mode. High expression of HHLA2 is correlated with smoking, PD-L1 and low CD8 expression, and predicted a poor overal survival in patients with esophageal cancer. Our results demonstrated that HHLA2 is a critical immune checkpoint in eaophageal cancer. Our results together with these literatures illustrated that HHLA2 was potentially participated in cancer progression through immunosuppressive pattern and could be a preditive factor except the PD-L1 checkpoint for cancer diagnosis and immunotherapy [16], while further studies are necessary to clarify the mechanisms of high HHLA2 expression and its therapeutic values in cancer progression. Several limitations relating to this study were underlined as follows. Firstly, our study was based on a cohort with 69 esophageal cancer cases in total, the number of which is too less and maybe the reason why HHLA2 was associated with poor prognostic value for overall survival in patients with esophageal cancer but not so significantly. Secondly, most esophageal cancer patients here in this study were more than 60 years old as esophageal cancer is usually diagnosed at an advanced stage due to the lack of early clinical symptoms.Thirdly, all of the patients here in the research having esophageal squamous cell cancers. Finally, we just combined HHLA2 with PD-L1 to conduct immune classification. However, other B7 family members, like B7-H3 and B7x, or other immunosuppressive factors like metabolites also contribute to immunosuppression in the tumor microenvironment[44,45], so further studies including more esophageal cancer cases are necessary to valiadte the results of this study and elucidate the detail mechanisms.
Declarations
Author contributions
Conception, design and drafting of the article: Jun-Lan Guo and Xia Jin. Performing experiments:Peng-Zhi Zhu, Xiao-Dong Zheng, Shi-Wei Nie and Li-Hua Wang. Acquisition and interpretation of data: Yuan-Yuan Ji and Ning Zhang. Review, editing and approval of the manuscript: all authors.
Conflict of interest: The authors declare no competing financial interests in this research.
Acknowledgements: This study was supported in part by a project (2018021021) from the Medical Science and Technology Research of Henan Province.
Funding: Not applicable.
Availability of data and materials: All have been shown in the manuscript.
Ethics approval and consent to participate: The trial was approved by the local ethics committee of all participating centres. All recruited patients provided written informed consent before participating in the trial. The study was performed in accordance with declaration of Helsinki.
Consent for publication: All authors agree to the publication of the article.
References
- Siegel R L, Miller KD, Fuchs HE, Jemal A. 2022; 72(1): 7-33.
- Luo H, Lu J, Bai Y, Mao T, Wang J, et al. Effect of Camrelizumab vs Placebo Added to Chemotherapy on Survival and Progression-Free Survival in Patients With Advanced or Metastatic Esophageal Squamous Cell Carcinoma: The ESCORT-1st Randomized Clinical Trial. 2021; 326(10): 916-925.
- Pickens A, Orringer MB. Geographical distribution and racial disparity in esophageal cancer. 2003; 76(4): 1367-1369.
- Huang FL, Yu SJ. Esophageal cancer: Risk factors, genetic association, and treatment. Asian J 2018; 41(3): 210-215.
- Francis DM, Manspeaker MP, Schudel A, Sestito LF, O’Melia MJ, et al. Blockade of immune checkpoints in lymph nodes through locoregional delivery augments cancer immunotherapy. 2020; 12(563).
- Pardoll D M. The blockade of immune checkpoints in cancer immunotherapy. 2012; 12(4): 252-264.
- Isazadeh A, Hajazimian S, Garshasbi H, Shadman B, Baghbanzadeh A, et al. Resistance mechanisms to immune checkpoints blockade by monoclonal antibody drugs in cancer immunotherapy: Focus on myeloma. 2021; 236(2): 791-805.
- Auslander N, Zhang G, Lee JS, Frederick DT, Miao B, et al. Publisher Correction: Robust prediction of response to immune checkpoint blockade therapy in metastatic melanoma. 2018; 24(12): 1942.
- Kelly RJ, Ajani JA, Kuzdzal J, Zander T, Van Cutsem E, et al. Adjuvant Nivolumab in Resected Esophageal or Gastroesophageal Junction Cancer. 2021; 384(13): 1191-1203.
- Boukouris AE,Theochari M, Stefanou D, Papalambros A, Felekouras E, et al. Latest evidence on immune checkpoint inhibitors in metastatic colorectal cancer: A 2022 update. Crit Rev Oncol Hematol. 2022; 173(103663).
- Wu HX, Pan YQ, He Y, Wang ZX, Guan WL, et al. Clinical Benefit of First-Line Programmed Death-1 Antibody Plus Chemotherapy in Low Programmed Cell Death Ligand 1-Expressing Esophageal Squamous Cell Carcinoma: A Post Hoc Analysis of JUPITER-06 and Meta-Analysis. 2023; 41(9): 1735-1746.
- Xiao Y, Freeman GJ. A New B7: CD28 Family Checkpoint Target for Cancer Immunotherapy: HHLA2. 2015; 21(10): 2201-2203.
- Zhou QH, Li KW, Chen X, He HX, Peng SM, et al. HHLA2 and PD-L1 co-expression predicts poor prognosis in patients with clear cell renal cell carcinoma. 2020; 8(1).
- Farrag MS, Ibrahim EM, El-Hadidy TA, Akl MF, Elsergany AR, et al. Human Endogenous Retrovirus-H Long Terminal Repeat- Associating Protein 2 (HHLA2) is a Novel Immune Checkpoint Protein in Lung Cancer which Predicts Survival. 2021; 22(6): 1883-1889.
- Bolandi N, Derakhshani A, Hemmat N, Baghbanzadeh A, Asadzadeh Z, et al. The Positive and Negative Immunoregulatory Role of B7 Family: Promising Novel Targets in Gastric Cancer Treatment. 2021; 22(19).
- Koirala P, Roth ME, Gill J, Chinai JM, Ewart MR, et al. HHLA2, a member of the B7 family, is expressed in human osteosarcoma and is associated with metastases and worse survival. 2016; 6(31154).
- Lin G, Ye H, Wang J, Chen S, Chen X, et al. Immune Checkpoint Human Endogenous Retrovirus-H Long Terminal Repeat-Associating Protein 2 is Upregulated and Independently Predicts Unfavorable Prognosis in Bladder Urothelial Carcinoma. 2019; 141(4): 256-264.
- Xu Y, Huang Z, Yu X, Li Z, Zheng L, et al. HHLA2 Expression is Associated with Poor Survival in Patients with Hepatocellular Carcinoma. 2021; 15(329-341).
- Xu G, Shi Y, Ling X, Wang D, Liu Y, et al. HHLA2 predicts better survival and exhibits inhibited proliferation in epithelial ovarian cancer. 2021; 21(1): 252.
- Zhang C, Xu J, Ye J, Zhang X. Prognostic value of HHLA2 expression in solid tumors: A meta-analysis based on the Chinese population. 2021; 100(30): 26789.
- Sun W, Li S, Tang G, Sun S, Luo Y, et al. HHLA2 deficiency inhibits non-small cell lung cancer progression and THP-1 macrophage M2 polarization. 2021; 10(15): 5256-5269.
- Zhang C, Wang F, Sun N, Zhang Z, Zhang G, et al. The combination of novel immune checkpoints HHLA2 and ICOSLG: A new system to predict survival and immune features in esophageal squamous cell carcinoma. 2022; 9(2): 415-428.
- Wang R, Guo H, Tang X, Zhang T, Liu Y, et al. Interferon Gamma-Induced Interferon Regulatory Factor 1 Activates Transcription of HHLA2 and Induces Immune Escape of Hepatocellular Carcinoma Cells. 2022; 45(1): 308-330.
- Wei Y, Ren X, Galbo PM, Moerdler S,Wang H, et al. KIR3DL3-HHLA2 is a human immunosuppressive pathway and a therapeutic target. 2021; 6(61).
- Xie R, Chen X, Chen Z, Huang M, Dong W, et al. Polypyrimidine tract binding protein 1 promotes lymphatic metastasis and proliferation of bladder cancer via alternative splicing of MEIS2 and PKM. 2019; 449(31-44).
- Chen X, Xie R, Gu P, Huang M, Han J, et al. Long Noncoding RNA LBCS Inhibits Self-Renewal and Chemoresistance of Bladder Cancer Stem Cells through Epigenetic Silencing of SOX2. 2019; 25(4): 1389-1403.
- Robsahm TE, Aagnes B, Hjartåker A, Langseth H, Bray FI, et al. Body mass index, physical activity, and colorectal cancer by anatomical subsites: a systematic review and meta-analysis of cohort studies. 2013; 22(6): 492-505.
- Jing CY, Fu YP, Yi Y, Zhang MX, Zheng SS, et al. HHLA2 in intrahepatic cholangiocarcinoma: an immune checkpoint with prognostic significance and wider expression compared with PD-L1. 2019; 7(1): 77.
- Ding L, Yu Q, Yang S, Yang WJ, Liu T, et al. Comprehensive Analysis of HHLA2 as a Prognostic Biomarker and Its Association With Immune Infiltrates in Hepatocellular Carcinoma. 2022; 13(831101).
- Zhu Z, Dong W. Overexpression of HHLA2, a member of the B7 family, is associated with worse survival in human colorectal carcinoma. 2018; 11(1563-1570).
- Chen D, Chen W, Xu Y, Zhu M, Xiao Y, et al. Upregulated immune checkpoint HHLA2 in clear cell renal cell carcinoma: a novel prognostic biomarker and potential therapeutic target. 2019; 56(1): 43-49.
- Janakiram M, Chinai JM, Fineberg S, Fiser A, Montagna C, et al. Expression, Clinical Significance, and Receptor Identification of the Newest B7 Family Member HHLA2 Protein. 2015; 21(10): 2359-2366.
- Zou W, Wolchok JD, Chen L. PD-L1 (B7-H1) and PD-1 pathway blockade for cancer therapy: Mechanisms, response biomarkers, and combinations. 2016; 8(328): 328rv324.
- Short MW, Burgers KG, Fry VT. Esophageal Cancer. 2017; 95(1): 22-28.
- Borggreve AS, Kingma BF, Domrachev SA, Koshkin MA, Ruurda JP, et al. Surgical treatment of esophageal cancer in the era of multimodality management. 2018; 1434(1): 192-209.
- Qi Y, Deng G, Xu P, Zhang H, Yuan F, et al. HHLA2 is a novel prognostic predictor and potential therapeutic target in malignant glioma. 2019; 42(6): 2309-2322.
- Yan H, Qiu W, Koehne de Gonzalez AK, Wei JS, Tu M, et al. HHLA2 is a novel immune checkpoint protein in pancreatic ductal adenocarcinoma and predicts post-surgical survival. 2019; 442(333-340).
- Zhu Y, Yao S, Iliopoulou BP, Han X, Augustine MM, et al. B7-H5 costimulates human T cells via CD28H. 2013; 4(2043).
- Zhao R, Chinai JM, Buhl S, Scandiuzzi L, Ray A, et al. HHLA2 is a member of the B7 family and inhibits human CD4 and CD8 T-cell function. Proc Natl Acad Sci U S A. 2013; 110(24): 9879-9884.
- Janakiram M, Shah UA, Liu W, Zhao A, Schoenberg MP, et al. The third group of the B7-CD28 immune checkpoint family: HHLA2, TMIGD2, B7x, and B7-H3. 2017; 276(1): 26-39.
- Schildberg FA, Klein SR, Freeman GJ, Sharpe AH. Coinhibitory Pathways in the B7-CD28 Ligand-Receptor Family. 2016; 44(5): 955-972.
- Cheng H, Borczuk A, Janakiram M, Ren X, Lin J, et al. Wide Expression and Significance of Alternative Immune Checkpoint Molecules, B7x and HHLA2, in PD-L1-Negative Human Lung Cancers. 2018; 24(8): 1954-1964.
- Cheng H, Janakiram M, Borczuk A, Lin J, Qiu W, et al. HHLA2, a New Immune Checkpoint Member of the B7 Family, Is Widely Expressed in Human Lung Cancer and Associated with EGFR Mutational Status. 2017; 23(3): 825-832.
- Stagg J, Smyth MJ. Extracellular adenosine triphosphate and adenosine in cancer. 2010; 29(39): 5346-5358.
- Munn DH, Mellor AL. IDO in the Tumor Microenvironment: Inflammation, Counter-Regulation, and Tolerance. 2016; 37(3): 193-207.