
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Kaposi’s Sarcoma in a patient with rheumatoid arthritis treated with tofacitinib
Elisabet Castañeda-Estévez1; Tatiana Cobo-Ibáñez1; Iolanda Prats-Caelles2; María Beatriz Paredes-Romero1; Santiago Muñoz- Fernández1*
1Department of Rheumatology, Hospital Universitario Infanta Sofía, FIIB HUIS HHEN, Universidad Europea, Madrid, Spain.
2Department of Dermatology, Hospital Universitario Infanta Sofía, FIIB HUIS HHEN, Universidad Europea, Madrid, Spain.
*Corresponding Author : Muñoz- Fernández S
Department of Rheumatology, Hospital Universitario Infanta Sofía, Universidad Europea de Madrid, Madrid, Spain.
Email: santiago.munoz@salud.madrid.org
Received : Aug 28, 2024
Accepted : Sep 17, 2024
Published : Sep 24, 2024
Archived : www.jcimcr.org
Copyright : © Muñoz- Fernández S (2024).
Citation: Muñoz- Fernández S, Castañeda-Estévez E, Cobo-Ibáñez T, Prats-Caelles I, Paredes-Romero MB. Kaposi’s Sarcoma in a patient with rheumatoid arthritis treated with tofacitinib. J Clin Images Med Case Rep. 2024; 5(9): 3266.
Description
Kaposi’s Sarcoma (KS) is a multicentric antiproliferative tumor of mesenchymal origin with 4 variants, namely, classic, African, AIDS-associated, and iatrogenic. The iatrogenic variant has been associated with immunosuppressive treatment [1]. Iatrogenic Kaposi’s Sarcoma (IKS) co-occurring with Rheumatoid Arthritis (RA) seems to result from a complex interaction between geographic, genetic, environmental, and immunological factors, as well as various drugs used in patients with RA [2]. While the distribution patterns of KS subtypes remain unknown, the percentage of IKS in published case series ranges from 9% to 27%. In a cohort of 143 non-transplanted patients with IKS, RA was the most frequent underlying condition (12.7%) [1]. Two cases of IKS associated with JAK inhibitor (Jakinib) therapy were recently published. In one, a patient with ulcerative colitis treated with tofacitinib for 2 years developed IKS, which resolved after discontinuation of the drug. To our knowledge, this is the first published case in which treatment with tofacitinib could be associated with IKS [3]. In the other, a patient with RA associated with monoclonal gammopathy of undetermined significance treated with baricitinib developed IKS, although clear causality could not be established. We present a case of KS in a patient with RA treated with tofacitinib in which the Jakinib was not discontinued and the patient’s condition improved significantly after therapy with acitretin.s
The patient was a 70-year-old woman with a 15-year history of seronegative RA that responded poorly to methotrexate, infliximab, and tocilizumab. She was therefore prescribed tofacitinib 5 mg BID, with methotrexate maintained at 15 mg weekly and prednisone at 2.5-7.5 mg.
Twenty-four months after initiating treatment with tofacitinib, the patient developed palpable painful violaceous lesions on the dorsa of the feet, soles, and pretibial regions (Figure 1A) and was referred to the dermatology department. A thorough work-up that included blood tests, HIV serology, chest x-ray, and fecal occult blood test ruled out infection and neoplasia. A skin biopsy revealed histopathological changes typical of KS and positive findings for HHV-8. Treatment with prednisone and methotrexate was discontinued, tofacitinib was maintained, and oral acitretin 25 mg was prescribed for treatment of KS.
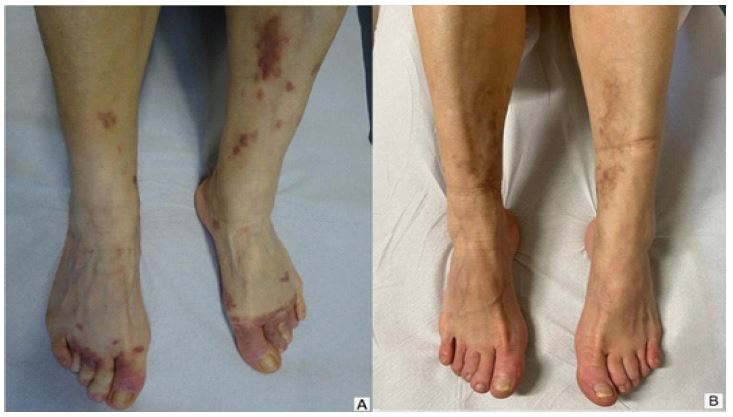
After 18 months of treatment with acitretin, the skin lesions recovered fully (Figure 1B). IKS has been reported in patients receiving corticosteroids and, less frequently, with azathioprine, methotrexate, leflunomide, mycophenolate, cyclophosphamide, and antitumor necrosis factor alpha agents [1,5,6].
Although the mechanism by which corticosteroids can induce or worsen KS is not fully understood, it could be related to direct or indirect stimulation of cell growth, which can enable proliferation of KS cells and induce an increase in viral replication of HHV-8 [7]. It is also known that inhibition of the JAK/STAT pathway can predispose to viral infections such as that caused by varicella zoster virus, although its association with HHV-8 has not been described. Some authors have suggested that Jakinibs such as ruxolitinib, which inhibits the JAK2/STAT3 pathway, could reduce levels of proinflammatory cytokines such as IL-6 and TNF and, possibly, CD4 and/or CD8 cell counts and impair natural killer cell function. These effects may favor the replication of viruses such as HHV-8 [8]. The immunosuppression caused by the combination of prednisone, methotrexate, and tofacitinib might have precipitated IKS. Therefore, we decided to continue treatment with tofacitinib to maintain low RA activity. This was achieved without precluding remission of IKS, suggesting that tofacitinib was not the only cause of IKS. The course of IKS can vary with the mechanisms underlying immune activation, individual responses to treatment, and other, associated risk factors. In conclusion, tofacitinib does not necessarily worsen IKS and could be maintained during treatment of IKS to ensure continued good control of RA.
Key message: Tofacitinib might not worsen IKS and makes it possible to sustain effective control of RA.
References
- Baykal C, Atci T, Buyukbabani N, Kutlay A. The spectrum of underlying causes of iatrogenic Kaposi’s sarcoma in a large series: A retrospective study. Indian J Dermatol. 2019; 64(5): 392-399. doi:10.4103/ijd.IJD_217_18
- Louthrenoo W, Kasitanon N, Mahanuphab P, Bhoopat L, Thongprasert S. Kaposi’s sarcoma in rheumatic diseases. Semin Arthritis Rheum. 2003; 32(5): 326-333. doi:10.1053/sarh.2002.50000
- Wetwittayakhlang P, Golovics PA, Afif W, Bessissow T, Lakatos PL. Tofacitinib-Associated Iatrogenic Kaposi Sarcoma in a Patient With Ulcerative Colitis. ACG Case Reports J. 2021; 8(11): e00678. doi:10.14309/crj.0000000000000678.
- Martínez Pallás I, Cuadrado Orden I, Cobeta García JC. Cutaneous Kaposi’s sarcoma in a patient with rheumatoid arthritis receiving baricitinib. Med Clin (Barc). 2022; 158(4): 193. doi:10.1016/j.medcli.2021.05.011
- Bergler-Czop B, Brzezinska-Wcisło L, Kolanko M. Iatrogenic Kaposi’s sarcoma following therapy for rheumatoid arthritis. Postep Dermatologii i Alergol. 2016; 33(2): 149-151. doi:10.5114/ada.2016.59163.
- Mariappan AL, Desai S, Locante A, Desai P, Quraishi J. Iatrogenic Kaposi Sarcoma Precipitated by Anti-Tumor Necrosis Factor-Alpha (Anti-TNF-α) Therapy. Cureus. 2021; 13(2): 2-6. doi:10.7759/cureus.13384
- González-Sixto B, Conde A, Mayo E, Pardavila R, De La Torre C, Cruces M. Sarcoma de Kaposi asociado a corticoterapia sistémica. Actas Dermosifiliogr. 2007; 98(8): 553-555. doi:10.1016/S0001-7310(07)70132-1
- Moutel M, Noel V, Jary A, et al. Iatrogenic Kaposi’s sarcoma in a myelofibrosis patient treated with ruxolitinib: Case-report, literature review, and French pharmacovigilance data. Am J Hematol. 2022; 97(1): E31-E34. doi:10.1002/ajh.26398