
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Exploring the relationship between the degree of fatty infiltration of multifidus muscle and the maximum compression degree of lumbar spinal canal in patients with lumbar disc herniation
CY Zhang; WJ Wu; LQ Wang*
The Seventh People’s Hospital of Chongqing, Orthopaedic Chongqing, Banan District 401320, Chongqing, China.
*Corresponding Author : Liang Qian Wang
The Seventh People’s Hospital of Chongqing, Orthopaedic Chongqing, Banan District 401320, Chongqing, China.
Tel: +86-1762307015;
Email: 18108395779@163.com
Received : Sep 02, 2024
Accepted : Sep 19, 2024
Published : Sep 26, 2024
Archived : www.jcimcr.org
Copyright : © Wang LQ (2024).
Abstract
Objective: To explore the relationship between the degree of fatty infiltration of the lumbar multifidus muscle and the maximum compression degree of the lumbar spinal canal in patients with lumbar disc herniation (LDH); The second objective is to investigate the relationship between the degree of fatty infiltration of the lumbar multifidus muscle and the Oswestry Disability Index.
Methods: A total of 200 LDH patients in our hospital from July 2019 to September 2023 were selected. The maximum compression degree of the lumbar spinal canal (Lumbar canal compromise, MLC) were obtained from T2-weighted axial MR images at mid-disc, at the level of maximum cord compression and the level below. And the total Cross-Sectional Area (CSA) of the multifidus muscle, the fat infiltration area (FCSA) were measured by Image J suftware at this level. The ratio of FCSA/CSA is the Degree of Fat Infiltration (DFI). The relationships between DFI and MLC, and between DFI and ODI, were assessed using multivariate linear regression models.
Results: Greater DFI was associated with increased MLC (P = 0.032) at the same level; DFI was positively correlated with ODI scores.
Conclusion: The imaging manifestation of lumbar multifidus muscle degeneration in LDH patients is an increase in the degree of fat infiltration, and the larger the DFI, the greater the degree of spinal canal compression and the greater the degree of lumbar back dysfunction.
Keywords: Multifidus muscle; Lumbar disc herniation; Magnetic resonance imaging; Maximum spinal canal compression; Degree of fat infiltration.
Abbreviations: LDH: Lumbar Disc Herniation; MLC: The Maximum Spinal Canal Occupancy; CSA: Total Cross-Sectional Area; FA: Fat Area; FCSA: The Fat Infiltration Area; DFI: Fat Infiltration; ODI: The Oswestry Disability Index.
Citation: Zhang CY, Wu WJ, Wang LQ. Exploring the relationship between the degree of fatty infiltration of multifidus muscle and the maximum compression degree of lumbar spinal canal in patients with lumbar disc herniation. J Clin Images Med Case Rep. 2024; 5(9): 3269.
Introduction
Background: The incidence of Lumbar Disc Herniation (LDH) is increasing year by year in the middle-aged and elderly population. The protrusion of lumbar intervertebral discs compressing nerves, resulting in pain and neurological symptoms, is a characteristic of this disease. Lumbar disc herniation begins with the degeneration of the spine and the loss of structural integrity [1,2]. Lumbar disc herniation begins with degeneration of the spine and loss of structural integrity. The lumbar multifidus muscle is an important structure to maintain the balance of flexion and extension of the spine [3,4]. Patients with chronic low back pain will have a certain degree of changes in the muscles around the spine, such as area reduction and fat infiltration [5,6]. Decompression surgery is considered a practical option for patients with progressive LDH. In addition, changes in the shape of the lower back muscles have important effects on their function and behavior. It is necessary to further investigate the relationship between muscle morphology, clinical outcomes, and functional status. Therefore, the purpose of this study was to investigate between the degree of fatty infiltration of the lumbar multifidus muscle and the maximum compression degree of the lumbar spinal canal in patients with Lumbar Disc Herniation (LDH). The second objective is to investigate the relationship between the degree of fatty infiltration of the lumbar multifidus muscle and the Oswestry Disability Index. Recent studies have shown that degeneration of the lumbar back muscles, especially the multifidus muscle, is often damaged in lumbar degenerative diseases and it atrophies in patients with lumbar disc herniation or chronic low back pain. Therefore, the presence and degree of morphological changes in the muscles of LDH patients deserve further attention [7]. Previous studies have shown that the relationship between multifidus muscle fat infiltration and the occurrence of degenerative lumbar spondylolisthesis, but there are few studies on whether multifidus muscle degeneration is involved in the occurrence of lumbar disc protrusion [8]. This study directly measures the fat area in the multifidus muscle by retrospectively analyzing the cross-sectional MRI images of the multifidus muscle at the L4/5 and L5/S1 intervertebral space levels in LDH patients. Through statistical analysis of the related factors of multifidus muscle fat infiltration in patients, the relationship between multifidus muscle fat infiltration and the degree of lumbar spinal canal injury is discussed.
Materials and methods
Inclusion criteria: Spinal stenosis at L4/5 or L5/S1 with or without low back pain and lower extremity pain.
Age 40-70 years.
Clear MRI images.
Exclusion criteria: Spinal trauma, deformity, scoliosis, tumor, infection, ankylosing spondylitis, previous history of lumbar spine surgery.
Incomplete imaging and clinical data.
General information
From January 2019 to September 2023, a total of 200 papatients with lumbar disc protrusion were included according to the inclusion and exclusion criteria; the age was 40-70 years, with an average of (57.07±5.12) years; body mass index, BMI 16.67-28.69 kg/m2, with an average of (23.51±2.59) kg/m2; visual analog scale, VAS score 3-8 points, with an average of (5.96±1.43) points; Oswestry disability index, ODI 25-49 points, with an average of (35.59±4.38) points (Table 1). This study has been approved by the Ethics Committee of Banan Hospital Affiliated to Chongqing Medical University, and all patients have signed informed consent forms.
Data and measurement
The measurement of lumbar muscle was performed using Image J imaging software (version 1.43; National Institutes of Health, Bethesda, MD, USA, available for download at http://rsbweb.nih.gov/ij/download.html) and 32-bit osirix software program (version 3.8.1; Pixmeo, Geneva, Switzerland) to position the image slices perpendicular when necessary [9]. The level and degree of the maximum spinal canal occupancy (MLC) were determined using the following formula: MLC = [1 - D (D1 + D2)/2] × 100, as defined by 14 (Figure 1A) [10]. The multifidus muscle was measured at the midline of both sides of the intervertebral disc, at the level of the maximum spinal cord compression and below (Figures 1B and C). Measurements included: Total Cross-Sectional Area (CSA), Fat Area (FA), and the ratio of FA/CSA (fat infiltration). The values of the sum of CSA or FA on the left and right sides at all levels were calculated, and the mean of the ratio of FA/CSA was calculated for analysis. The measurement of CSA used a highly reliable threshold technique described in a previous study [15] (Figure 1C). The relevant parameters were measured jointly by two spinal surgeons and the average value was taken.
Statistical methods
Statistical analysis was performed using SPSS 25.0 software. Measurement data were expressed as mean ± standard deviation. The independent sample t-test was used for the comparison of two sets of measurement data that met the normal distribution, and the rank-sum test was used for those that did not meet the normal distribution. Count data were expressed as rates and frequencies, and the chi-square test was used. P< 0.05 was considered statistically significant.
Result
The clinical characteristics of the patients, MRI measurements, and functional scores are shown in Table 1. The CSA range of 200 patients is 16.25-27.86 cm2, the FA range is 1.28-3.43 cm2, the FA/CSA is 8.91-19.28 (%), the average is 37.55±6.13 (%); the MLC range is 27.31-50.17%, the average is 37.55±6.13%; ODI score: 25-49%, the average is 35.59±4.38%; VAS score: 3-8 points, the average is 5.96±1.43 points. Statistical analysis was used to calculate the mean and standard deviation of the multifidus muscle measurement values. A multivariate linear regression model was used to investigate the relationship between DFI and MLC, and the relationship between DFI and MLC is listed in Table 2. Similarly, multivariate linear regression models were used to investigate the association between DFI and ODI, and the relationship between ODI and MLC is listed in Table 3. A larger DFI is associated with a higher MLC at the same level (P=0.024). At the same time, a larger DFI is also associated with a higher ODI (P=0.02).
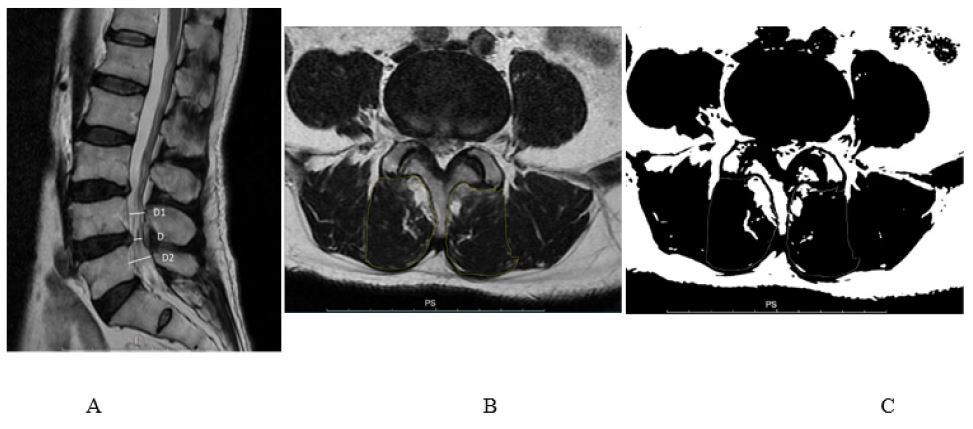
B: Total CSA of the MF muscle on the axial t2-weighted image at the L4/5 level.
C: The image shows the application of the signal threshold filter (Figure 1) to highlight the fat area and obtain the measurement value of the FA muscle.
Table 1: Basic situation of patients and imaging measurement statistics.
| Age | Sex | Segment | BMI | CSA(mm) | FA(mm) | FA/CSA(%) | MLC(%) | ODI(%) | VAS | |
|---|---|---|---|---|---|---|---|---|---|---|
| Range | 41-70 | Man:68Women:32 | L4/5:71L5/S1:29 | 16.25-27.86 | 14.36-17.79 | 1.28-3.43 | 8.91-19.28 | 27.31-50.17 | 25-49 | 3 -8 |
| Mean | 57.07±5.12 | 50 | 50 | 23.51±2.59 | 16.37±1.35 | 2.36±0.69 | 9.37±4.37 | 37.55±6.13 | 35.59±4.38 | 5.96±1.43 |
Table 2: The Relationship between DFI and MLC.
| DFI% | MLC% | T-value | p-value | |
|---|---|---|---|---|
| Sum | 9.37±4.37 | 37.55±6.13 | 2.128 | 0.024 |
| L4/5 | 9.49±3.68 | 34.02±4.32 | 3.576 | 0.032 |
| L5/S1 | 10.08±4.19 | 38.96±6.80 | 1.679 | 0.019 |
Table 3: Relationship between DFI and ODI Score.
| DFI% | ODI% | T-value | p-value | |
|---|---|---|---|---|
| Sum | 9.37±4.37 | 35.59±4.38 | 3.073 | 0.020 |
| L4/5 | 9.49±3.68 | 35.13±4.38 | 2.726 | 0.024 |
| L5/S1 | 10.08±4.19 | 35.62±4.38 | 4.351 | 0.017 |
Discussion
Studies have shown that the L4/5 and L5/S1 segments have large mobility, bear high and concentrated stresses, and lumbar intervertebral disc protrusion is common in these two segments. Bone, joint, muscle, and ligament jointly maintain the stability of the spine, and any change in the structure will cause instability of the spine [11]. Compared with other paraspinal muscles, the multifidus muscle dysfunction can lead to a decrease in the stability of the lumbar spine. At present, the research on the degeneration of the muscles around the spine focuses on the multifidus muscle [12,13]. Previous studies have found that compared with asymptomatic patients, the low back muscles of patients with low back pain show degenerative changes in terms of morphology (size, asymmetry, fat infiltration) and functional defects (delayed contraction, decreased muscle strength) [14-16]. In recent years, the research on fat infiltration in lumbar degenerative diseases has been increasing year by year. In the article “Study on the Relationship between Multifidus Fat Infiltration and Degenerative Lumbar Spondylolisthesis”. Tian Yahao [17] and others also explored that the imaging manifestations of multifidus muscle degeneration in patients with lumbar spondylolisthesis were an increase in the degree of fat infiltration, a decrease in the area of muscle tissue, and the degree of fat infiltration in the slipping segment was greater than that in the non-slipped segment. This study also discussed that the area of fat infiltration was closely related to the patient’s age. With the increase of age, the fat area gradually increased. The correlation between multifidus fat infiltration and lumbar sagittal parameters indicates that muscle characteristics may be related to sagittal alignment. However, there is little discussion on the relationship between the degree of multifidus fat infiltration and the degree of compression of the lumbar spinal canal [18].
This study screened 200 patients with lumbar intervertebral disc protrusion, collected the fat infiltration area of the multifidus muscle in the lower back at the maximum spinal canal compression level, and then calculated the degree of lumbar spinal canal injury. Data analysis of the results showed that there is a significant correlation between DFI and the MLC at the maximum compression level. The greater the spinal canal compression, the greater the fat infiltration. This is the same in both the L4/5 segment and the L5/S1 segment. The possible reason is that the more severe the lumbar degeneration, the greater the fat infiltration of the multifidus muscle, and the greater the imbalance of the sagittal plane of the spine due to the weakness of the muscle, resulting in more intervertebral disc protrusion, which ultimately leads to an increase in spinal canal compression [19]. Also believe that muscle mass may be one of the many factors affecting sagittal balance. Our research results also show a positive correlation between MLC and ODI scores. The more intervertebral disc protrusion, the more severe the spinal canal compression, the more severe the low back and leg pain symptoms, and the higher the ODI score. At the same time, the greater the fat infiltration of the low back muscles, the worse the muscle strength and the lower the quality of life. Dr. Neda Naghdi in “Morphological Changes of Deep Extensor Neck Muscles in Relation to the Maximum Level of Cord Compression and Canal Compromise in Patients with Degenerative Cervical Myelopathy” analyzed the relationship between the degree of spinal canal compression in the four segments of C3-C7 in patients with cervical spondylosis and the neck extensor muscles. The same as this study is that the greater the fat infiltration of the neck muscles, the greater the maximum compression of the cervical spinal cord. The difference is that this study also compared the relationship between the degree of cervical spinal cord injury and fat infiltration, which is also positively correlated [10].
In the current study, the degree of fat infiltration at the maximum level of spinal canal occupancy was measured on the MRI horizontal section, only assessing the relationship between the morphological changes of the multifidus muscle at the maximum compression level of MLC, and no direct comparison of fat volume was made. If the selected measurement levels are inconsistent, it may affect the results and the measurement of related paraspinal muscles [20,21]. Our research results also found that the more fat infiltration, the greater the asymmetry of the muscles on the left and right sides. Whether these markers of muscle degradation can be changed through pre- or postoperative rehabilitation exercises, thereby affecting the patient’s quality of life score and lumbar function, this requires further research [22]. Studied the relationship between different muscle qualities of the spine and different spinal pelvic parameters. They found that the reduction of pelvic anteversion is related to the reduction of the quality of the psoas muscle. This will be useful for studying whether the change of lumbar kyphosis and sagittal parameters will lead to changes in the morphology, composition, or functional outcomes of the paraspinal muscles. In view of the correlation of DFI with lumbar degenerative diseases, our research results are of great significance. We are now expanding this work to further evaluate the changes in the degree of fat infiltration of the multifidus before and after fusion surgery to study whether the morphology and composition of fat infiltration of the multifidus can predict postoperative outcomes, and whether it is related to the probability of postoperative infection.
Conclusion
In summary, the imaging manifestations of lumbar multifidus muscle degeneration in patients with lumbar intervertebral disc protrusion show that the larger the ratio of multifidus muscle fat infiltration, the greater the degree of spinal canal compression, and the greater the degree of low back dysfunction. Multifidus muscle fat infiltration is a risk factor for LDH.
Acknowledgments: We thank corresponding authors Wu Wenjie and Liangqian Wang for their guidance and help, and Banan Hospital Affiliated to Chongqing Medical University for providing a good platform.
References
- Wang Hg, Li Y. Analysis of the occurrence of adjacent segment degeneration after two surgical methods in the treatment of lumbar disc protrusion with instability J. Laboratory Medicine and Clinic. 2021; 18(01): 120-122.
- Wang X, Liu H, Wang W, Sun Y, Zhang F, et al. Comparison of multifidus degeneration between scoliosis and lumbar disc herniation. BMC Musculoskelet Disord. 2022; 23(1): 891. doi: 10.1186/s12891-022-05841-5.
- Agha O, Mueller-Immergluck A, Liu M, Zhang H, Theologis AA, et al. Intervertebral disc herniation effects on multifidus muscle composition and resident stem cell populations. JOR Spine. 2020; 3(2): e1091. doi: 10.1002/jsp2.1091.
- Liu C, Xue J, Liu J, Ma G, Moro A, et al. Is there a correlation between upper lumbar disc herniation and multifidus muscle degeneration? A retrospective study of MRI morphology. BMC Musculoskelet Disord. 2021; 22(1): 92. doi: 10.1186/s12891-021-03970-x.
- Zang Cy, Yang Wq, Jia Wp, et al. Research progress on the morphological and functional changes of paraspinal muscles in patients with lumbar disc protrusion J. Guangxi Medical Journal. 2021; 43(19): 2363-2365.
- Hu Ls, Zhao Y, Zhang Cz, et al. Imaging study on the fat changes of the multifidus lumbosacral in patients with lumbar disc protrusion J. Chinese Journal of Orthopedics and Traumatology. 2020; 33(02): 173-177.
- Tian G, Wang Y, Xia J, Wen J, Li T, et al. Correlation of multifidus degeneration with sex, age and side of herniation in patients with lumbar discherniation. BMC Musculoskelet Disord. 2023; 24(1): 652. doi: 10.1186/s12891-023-06783-2.
- Cao B, Zuo Y, Xu Y, Wu F, Du H, et al. Correlation between fatinfiltration of paraspinal muscle and L4 degenerative lumbar spondylolisthesis in asymptomatic adults. Asian J Surg. 2023; 46(2): 834-840. doi:10.1016/j.asjsur.2022.08.097.
- Zhang Yr, Zhang Ym, Wang Xy, et al. Predictive value of multifidus cross-sectional area in the recurrence of percutaneous endoscopic decompression through intervertebral foramen in patients with lumbar disc protrusion J. Journal of Cervicodynia and Lumbodynia, 2022, 43(05): 660-663+666.
- Naghdi N, Elliott JM, Weber MH, Fehlings MG, Fortin M. Morphological Changes of Deep Extensor Neck Muscles in Relation to the Maximum Level of Cord Compression and Canal Compromise in Patients With Degenerative Cervical Myelopathy. Global Spine J. 2022; 21925682221136492. doi: 10.1177/21925682221136492.
- Wang Xz. Study on scoliosis and multifidus muscle degeneration in lumbar intervertebral disc protrusion D. Hebei Medical University. 2022. DOI: 10.27111/d.cnki.ghyku.2022.000197.
- Hofste A, Soer R, Hermens HJ, et al. Inconsistent descriptions of lumbar multifidus morphology: A scoping review J. BMC Musculoskelet Disord, 2020; 21(1): 312.
- Ohyama S, Aoki Y, Inoue M, et al. The quantity and quality of lumbar muscles and lumbopelvic parameters in patients with degenerative spondylolisthesis J. Cureus. 2021; 13(10): e18428.
- Shi L, Yan B, Jiao Y, Chen Z, Zheng Y, et al. Correlation between the fatty infiltration of paraspinal muscles and disc degeneration and the underlying mechanism. BMC Musculoskelet Disord. 2022; 23(1): 509. doi: 10.1186/s12891-022-05466-8.
- Faur C, Patrascu JM, Haragus H, Anglitoiu B. Correlation between multifidus fatty atrophy and lumbar disc degeneration in low back pain. BMC Musculoskelet Disord. 2019; 20(1): 414. doi: 10.1186/s12891-019-2786-7.
- Colakoglu B, Alis D. Evaluation of lumbar multifidus muscle in patients with lumbar disc herniation: Are complex quantitative MRI measurements needed?. J Int Med Res. 2019; 47(8): 3590-3600. doi: 10.1177/0300060519853430.
- Tian Yh, Wu W, Li F. A study on the relationship between multifidus muscle fat infiltration and the occurrence of degenerative lumbar spondylolisthesis J. Biomedical Materials and Clinical Research. 2022; 19(05): 27-31.
- Zhang Y, Mandelli F, Mündermann A, Nüesch C, Kovacs B, et al. Association between fatty infiltration of paraspinal muscle, sagittal spinopelvic alignment and stenosis grade in patients with degenerative lumbarspinal stenosis. N Am Spine Soc J. 2021; 5: 100054. doi:10.1016/j.xnsj.2021.100054.
- Jun HS, Kim JH, Ahn JH, et al. The effect of lumbar spinal muscle on spinal sagittal alignment: Evaluating muscle quantity and quality. Neurosurgery. 2016; 79(6): 847-55.
- Rai RR, Shah Y, Shah S, et al. A radiological study of the association of facet joint tropism and facet angulation with degenerative spondylolisthesis J. Neurospine. 2019; 16(4): 742-747.
- Wang G, Karki SB, Xu S, et al. Quantitative MRI and X-ray analysis of disc degeneration and paraspinal muscle changes in degenerative spondylolisthesis J. J Back Musculoskelet Rehabil. 2015; 28(2): 277-285.
- Masaki M, Ikezoe T, Fukumoto Y, et al. Association of sagittal spinal alignment with thickness and echo intensity of lumbar back muscles in middle-aged and elderly women. Arch Gerontol Geriatr. 2015; 61(2): 197-201.