
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Cerebral venous thrombosis as an uncommon etiology of spontaneous subarachnoid hemorrhage: Case report
Gloire Chubaka Magala1*; Muriel Amon-Tanoh1,2; Désirée Arlette Aka1; Fiacre Delors Offoumou1; Cédric Valéry Kadjo1,2; Constance Yapo-Ehounoud1,2; Mavouloh Kourouma1; Abel Christian Tanoh1,2; Mariam Doumbia-Ouattara2,4; Paulette Yapo-Yapi Chia3; Évelyne Aka-Anghui Diarra1,2; Berthe Assi1,2
1Neurology Department, Cocody Teaching Hospital, Abidjan, Ivory Coast.
2Nervous System and Rehabilitation Department, Felix Houphouët-Boigny University, Abidjan, Ivory Coast
3International Training Center for French-speaking African Radiologists, Felix Houphouët-Boigny University, Abidjan, Ivory Coast.
4Neurology Department, Treichville Teaching Hospital, Abidjan, Ivory Coast.
*Corresponding Author : Gloire Chubaka Magala
Neurology Department, Cocody Teaching Hospital, Abidjan, Ivory Coast.
Tel: +2250711109368;
Email: drmagalagloire@gmail.com
Received : Sep 02, 2024
Accepted : Sep 19, 2024
Published : Sep 26, 2024
Archived : www.jcimcr.org
Copyright : © Chubaka Magala G (2024).
Abstract
Background: Spontaneous or non-traumatic subarachnoid hemorrhage is predominantly attributed to the rupture of an aneurysm, accounting for 85% of cases, while non-aneurysmal peri mesencephalic hemorrhage constitutes approximately 10%. Although rare, cerebral venous thrombosis can also lead to subarachnoid hemorrhage, presenting clinical and radiological signs that may closely resemble those of an intracranial aneurysm rupture, thereby complicating the diagnostic process. It is essential to rule out cerebral venous thrombosis in instances of spontaneous subarachnoid hemorrhage, as this condition is treatable and can help prevent recurrences. This case marks the first documentation of such an occurrence in the West African sub-region.
Case presentation: A 66-year-old female patient with a history of hypertension, was admitted to our department due to the sudden onset of acute headaches. These headaches, described as a thunderclap, had been persisting for approximately ten days and accompanied by a cavernous syndrome characterized by complete ophthalmoplegia of the left oculomotor nerve and pain localized to the left hemiface along the distribution of the V1 branch of the trigeminal nerve and meningeal syndrome. Magnetic Resonance Imaging (MRI), which included morphological sequences such as T1-weighted, T2-weighted, Fluid-Attenuated Inversion Recovery (FLAIR), and gradient echo sequences, as well as vascular sequences including Magnetic Resonance Venography (MRV), revealed a subarachnoid hemorrhage, associated with left-sided venous sinus thrombosis (transverse, sigmoid, and left internal jugular sinuses). Anticoagulant therapy was initiated, and the clinical course improved under this treatment.
Conclusion: it is essential to consider and rule out the possibility of cerebral venous thrombosis in cases of spontaneous subarachnoid hemorrhage, facilitated by significant advancements in neuroimaging techniques. The initiation of anticoagulant therapy should not be postponed, as timely intervention is crucial for optimizing short-term outcomes and preventing potential severe neurological sequelae.
Keywords: Cerebral venous thrombosis; Subarachnoid hemorrhage; Uncommon etiology Abidjan; Case report.
Citation: Chubaka Magala G, Amon-Tanoh M, Aka Arlette D, Delors Offoumou F, Valéry Kadjo C, et al. Cerebral venous thrombosis as an uncommon etiology of spontaneous subarachnoid hemorrhage: Case report. J Clin Images Med Case Rep. 2024; 5(9): 3270.
Introduction
Subarachnoid hemorrhage (SAH) represents a pathological condition marked by bleeding in the space between the brain and the dura mater [1]. Although this type of stroke is relatively uncommon, it carries significant severity, primarily impacting individuals approximately 55 years of age. The leading causes of SAH are the rupture of an aneurysm and arteriovenous malformations. Additionally, it is noteworthy that cerebral venous sinus thrombosis can occasionally present symptoms similar to those of an intracranial aneurysm rupture [2], which creates substantial diagnostic difficulties and may result in serious outcomes if not swiftly and accurately diagnosed and managed.
Cerebral Venous Sinus Thrombosis (CVT) is an uncommon type of stroke, comprising roughly 1% of all stroke occurrences. It is defined by the presence of blood clots in the dural venous sinuses, which are large vessels found between the two layers of the dura mater and are essential for draining blood from the brain into the systemic circulation. Cortical venous thrombosis specifically refers to the obstruction of veins on the brain’s surface, while cerebral venous thrombosis encompasses both dural and cortical thromboses [3].
CVT has an annual incidence ranging from 0.22 to 1.57 per 100,000 individuals [2], a figure that is on the rise due to the increased utilization of Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) in the assessment of patients presenting with acute headaches and/or first seizures. However, the diagnosis of this condition can be challenging due to its clinical and radiological polymorphism [4]. It is observed more frequently in women and children compared to adult men, with a mortality rate of approximately 30% [5]. Clinical symptoms vary based on the location and rate of thrombus progression, with headache being the most consistent symptom [6], followed by seizures, encephalopathy, and cranial nerve paralysis. Major radiological findings include cerebral edema, venous infarction (which may be hemorrhagic). Superficial manifestations, such as cortical or perimesencephalic subarachnoid hemorrhage associated with cerebral venous thrombosis, are considered to be quite rare [7].
Non-traumatic SAH is primarily caused by the rupture of an intracranial aneurysm in approximately 85% of cases [8]. The sudden onset of a severe headache, frequently characterized as “thunderclap headaches,” represents the predominant clinical feature [9]. Only 15% of SAH cases are not aneurysmal in origin, which may include arteriovenous malformations, vascular dissections, dural venous fistulas, metastatic diseases, and diathesis-related hemorrhages [10]. Additionally, cerebral venous thrombosis has been documented as a cause of SAH, often in conjunction with hemorrhagic venous infarction [11].
Recognizing CVT as the underlying cause SAH is essential for appropriate management, as the treatment protocols differ significantly from those employed for aneurysmal SAH [12]. CVT is amenable to medical treatment and requires prompt anticoagulation to avert long-term neurological complications. In contrast, anticoagulation in the context of aneurysmal SAH can lead to severe adverse outcomes [8].
This study outlines the case of a patient diagnosed with thrombosis of the right-sided sinuses (transverse sinus, sigmoid sinus, right jugular vein) alongside a Fischer IV type subarachnoid hemorrhage, with clinical manifestations that mimic an aneurysmal rupture. There is a scarcity of reported cases in sub-Saharan Africa, and this finding represents the first clinical description in Côte d’Ivoire and the broader West African region.
Observation
We present the case of a 66-year-old female patient with a history of hypertension, who was admitted to the neurology department of the COCODY University Hospital Center due to recent and unusual headaches. These headaches, which manifested abruptly like a thunderclap, occurred ten days prior to her admission. They were localized at the vertex with radiation to the orbitofrontal region, characterized by high intensity, persistence, and absence of nausea or photophobia. The headaches worsened with physical exertion and did not respond to standard analgesics. One day later, the patient developed a low-grade fever and generalized fatigue, prompting her to seek care at several peripheral healthcare facilities. During these visits, a hypertensive crisis was noted, and she was initially treated for hypertensive encephalopathy; however, there was no improvement in her symptoms, leading to her transfer to our neurology department.
The initial neurological assessment revealed both extrinsic and intrinsic ophthalmoplegia affecting the left oculomotor nerve, along with hemifacial pain following the V1 pathway on the same side and meningeal syndrome. The patient remained conscious and showed no signs of sensory or motor impairment in the extremities.
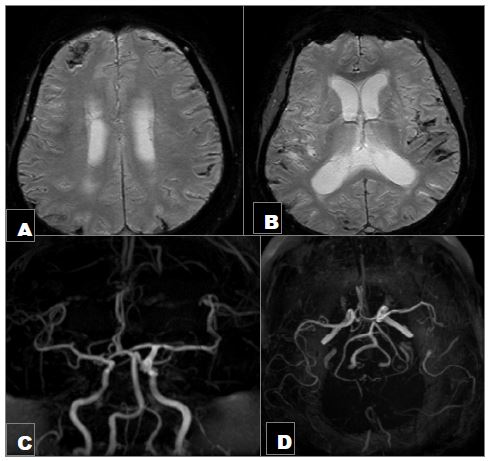
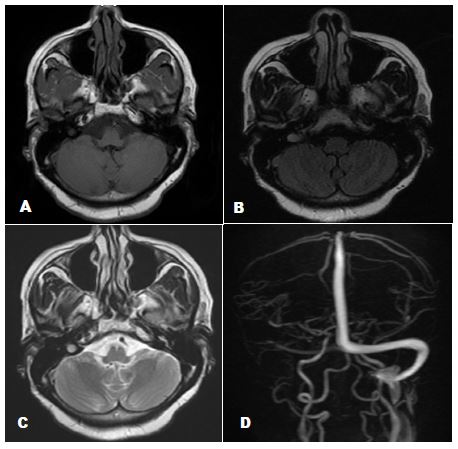
In the context of a cavernous syndrome accompanied by meningeal symptoms, the initial diagnosis of subarachnoid hemorrhage resulting from the rupture of an intracranial aneurysm was considered. A subarachnoid hemorrhage was confirmed through morphological sequences of brain MRI, particularly utilizing gradient echo sequences (Figure 1A,1B). Magnetic Resonance Angiography (MRA) with Maximum Intensity Projection (MIP) and Time-of-Flight (3D TOF) techniques ruled out the presence of an intracranial aneurysm or other arteriovenous malformations (Figure 1C,1D). Additionally, magnetic resonance venography (MRV) indicated thrombosis of the right-sided sinuses, including the transverse sinus, sigmoid sinus, and right internal jugular vein (Figure 2D). Laboratory tests showed D-Dimer levels at 9200 ng/l, which is 13 times the normal range for the patient’s age.
Consequently, a diagnosis of cerebral venous thrombosis complicated by subarachnoid hemorrhage was established, and anticoagulant therapy was promptly initiated, leading to favorable clinical outcomes.
Discussion
The initial description of cerebral venous thrombosis was provided by Ribes in 1825 [7]. For many years, this condition was perceived as an infectious disease that resulted in the obstruction of the superior sagittal sinus. The advent of imaging technologies has significantly improved the reliability of diagnosing CVT, facilitating a deeper understanding of its clinical manifestations [8]. According to the largest international study, the “International Study on Cerebral Vein and Dural Sinus Thrombosis” (ISCVT) [9], the incidence of this condition in the general population is estimated to be between 1 and 2 cases per 100,000 individuals [13-15].
Spontaneous SAH occurs in 85% of cases due to the rupture of an aneurysm, while 10% is attributed to non-aneurysmal perimesencephalic hemorrhage. The remaining 5% is linked to rare conditions such as arterial dissection, dural arteriovenous fistulas, pituitary apoplexy, and cocaine abuse [16,17]. Additionally, CVT has been identified in the literature as a potential cause of SAH and hemorrhagic venous infarction [11,18].
The diagnosis of CVT is challenging due to its clinical and radiological polymorphism [19]. There are no clearly defined anatomical-clinical syndromes, and a lack of correlation exists between the severity of parenchymal lesions and the extent of sinus thrombosis; all sinuses and veins may be involved, often in combination in approximately 60% of cases [4]; A thrombosis of the cavernous sinus might be implicated, despite not being visible on imaging studies, potentially elucidating the cavernous syndrome exhibited by our patient. The diagnostic process becomes even more complicated when patients initially present with acute subarachnoid hemorrhage, particularly if symptoms suggestive of an aneurysm are present, such as sudden thunderclap headaches accompanied by a cavernous syndrome upon neurological examination, as illustrated in our case. Approximately 35% of patients exhibiting cavernous syndrome during neurological assessment have an aneurysm located at the junction of the distal internal carotid artery and the posterior communicating artery, or, less frequently, at the level of the superior cerebellar artery [20].
The research carried out by Bruijn et al. involved 76 patients diagnosed with confirmed CVT, among whom ten exhibited thunderclap headaches. The clinical features of these headaches, as well as the accompanying signs, were indistinguishable from those found in subarachnoid hemorrhage cases. At the time of admission, the computed tomography results were deemed normal for five patients, showed evidence of subarachnoid hemorrhage in three patients, and indicated multiple intracranial hemorrhagic lesions in the others [21].
MRI serves as the gold standard for diagnosing CVT [22], and its increased availability in resource-limited countries has facilitated more frequent diagnoses. In the case of our patient, the brain MRI conducted approximately 12 days after the onset of symptoms, utilizing T2-weighted and FLAIR sequences, revealed hyperintensity in the right sigmoid sinus and the right internal jugular bulb, indicating the presence of endoluminal thrombosis. Furthermore, Magnetic Resonance Angiography (MRA) showed an absence of flow in the right lateral sinus, with no aneurysm detected. The gradient echo sequence (T2*) highlighted a subarachnoid hemorrhage accompanied by a heterogeneous hemorrhagic focus in the right frontopolar region. D-dimer serves as a valuable marker for diagnosis due to its negative predictive value concerning thromboembolic diseases. In the case of our patient, the D-dimer levels measured at 9200 ng/l are 13 times higher than the normative values for her age, thereby supporting our diagnosis.
Endoluminal thrombosis exhibits a variable signal depending on its age. In the initial days, it typically presents as iso- or hypointense on T1 and T2 sequences, which can lead to diagnostic confusion. The definitive diagnosis relies on venous MR angiography with contrast agent administration, alongside the analysis of T1 sequences post-gadolinium injection, which reveals an intraluminal lacunar image accompanied by an amputation [22]. The T2* gradient echo sequence facilitates early diagnosis, potentially within a week, by highlighting an intraluminal hypo intensity. However, this was not applicable in the current case, as the MRI was conducted two weeks following the onset of clinical symptoms. By the end of the first week, thrombosis is characterized by hyperintensity on T1, T2 SE, and FLAIR sequences [23], as noted in this instance at the junction of the sigmoid sinus and the right internal jugular bulb (Figure 2A-2C).
The precise mechanisms underlying SAH in the context of CVT are not fully elucidated. A hemorrhagic venous infarct can result in secondary ruptures in the subarachnoid spaces, which may trigger SAH. Furthermore, the presence of dural sinus thrombosis, along with secondary venous hypertension, can contribute to SAH in the subarachnoid space through the rupture of delicate, thin-walled cortical veins. This condition may lead to the dilation of cortical veins, increasing the risk of rupture and subsequent bleeding into the subarachnoid space, thus causing SAH.
Non-invasive angiographic techniques, such as CT or MR angiography focused on the arteries of the circle of Willis, employed in our clinical setting for the assessment of patients with acute SAH, do not provide satisfactory imaging of distal arteries or the venous system within a single imaging session. Unless cerebral venous thrombosis is routinely included in the diagnostic evaluation of SAH, this condition may be overlooked when utilizing these non-invasive angiographic methods [17]. The presence of acute SAH accompanied by an intraparenchymal hemorrhagic focus, without involvement of the basal cisterns, should warrant not only dedicated vascular imaging of the intracranial arteries but also specific imaging of the dural sinuses to investigate potential cerebral venous thrombosis that may require urgent medical intervention with anticoagulants.
Conclusion
The recognition of cerebral venous thrombosis as an underlying cause of subarachnoid hemorrhage is of paramount importance to prevent diagnostic errors and inappropriate management. Even when clinical symptoms suggestive of an intracranial aneurysm rupture are present, it is essential for clinicians to consider the possibility of venous thrombosis. This perspective may prompt radiologists to investigate the venous sinuses, facilitating early diagnosis and enhancing the vital and functional prognosis for affected patients.
Declarations
Consent for publication: Written informed consent was obtained from the patient for publication of this case report.
Conflict of interest: There is no conflict of interest that the authors of this case are aware of.
Authors’ contribution: Chubaka write case report, all author read the case and they approve to publish.
Acknowledgment: The lead author, Gloire Chubaka Magala, expresses profound gratitude to the entire committee of the BEBUC Excellence Scholarship Program for their steadfast confidence, encouragements and financial assistance rendered throughout his master’s studies in clinical neuroscience.
References
- S R Ahmadi Koupaei, et al. An Epidemiological Investigation on Patients with Non-traumatic Subarachnoid Hemorrhage from 2010 to 2020. Bull Emerg Trauma. 2024; 12(1): 35‑41. doi: 10.30476/BEAT.2024.101708.1495.
- D Jesuyajolu, O Olukoya, et al. Simultaneous occurrence of subarachnoid hemorrhage and cerebral venous sinus thrombosis: A systematic review of cases. Clin Case Rep. 2022; 10(8): e6200. doi: 10.1002/ccr3.6200.
- H A Algahtani, A A Aldarmahi, et al. Cerebral venous sinus thrombosis. Neurosciences (Riyadh). 2014; 19(1): 11‑16.
- M G Bousser, J M Ferro, et al. Cerebral venous thrombosis: An update. Lancet Neurol. 2007; 6(2): 162‑170. doi: 10.1016/S1474-4422(07)70029-7.
- Prognosis of Cerebral Vein and Dural Sinus Thrombosis Stroke. Consulté le. 2024; 23. Disponible sur: https://www.ahajournals.org/doi/full/10.1161/01.STR.0000117571.76197.26.
- C Tanislav, et al. Cerebral vein thrombosis: Clinical manifestation and diagnosis. BMC Neurol. 2011; 11(69). doi: 10.1186/1471-2377-11-69.
- Sahin. Cerebral venous thrombosis as a rare cause. Google Scholar. Consulté le. 2024; 23. Disponible sur: https://scholar.google.com/scholar_lookup?journal=Clin+Imaging&title=Cerebral+venous+thrombosis+as+a+rare+cause+of+subarachnoidal+hemorrhage;+case+report+and+literature+review&author=N+Sahin&author=A+Solak&author=B+Genc&author=N+Bilgic&volume=38&publication_year=2014&pages=373-9&pmid=24746346&doi=10.1016/j.clinimag.2014.03.005&.
- J I Suarez, R W Tarr, W R Selman, et al. Aneurysmal subarachnoid hemorrhage. N Engl J Med. 2006; 354(4): 387‑396. doi: 10.1056/NEJMra052732.
- D’Souza. Aneurysmal subarachnoid hemorrhage - Google Scholar. Consulté le. 2024. Disponible sur: https://scholar.google.com/scholar_lookup?journal=J+Neurosurg+Anesthesiol&title=Aneurysmal+subarachnoidhemorrhage&author=S+D%E2%80%99Souza&volume=27&publication_year=2015&pages=222-240&pmid=25272066&.
- C Spitzer, M Mull, V Rohde, M Kosinski, et al. Non-traumatic cortical subarachnoid haemorrhage: diagnostic work-up and aetiological background. Neuroradiology. 2005; 4(7): 525‑531. doi: 10.1007/s00234-005-1384-6.
- H. Rice et Y. M. Tang. Acute subarachnoid haemorrhage: a rare presentation of cerebral dural sinus thrombosis. Australas Radiol. 2006; 50(3): 241‑245. doi: 10.1111/j.1440-1673.2006.01569.x.
- M. Azeemuddin, M. Awais, F. Mubarak, A. Rehman, et N. U.-A. Baloch. Prevalence of subarachnoid haemorrhage among patients with cranial venous sinus thrombosis in the presence and absence of venous infarcts. Neuroradiol J. 2018; 31(5): 496‑503. doi: 10.1177/1971400918783060.
- D. Kombate et al. Prevalence hospitaliere et facteurs de risque de la thrombose veineuse cerebrale au Togo. African Journal of Neurological Sciences. 2017; 36(1): 1.
- E. Masson. Les thromboses veineuses cérébrales en milieu hospitalier à Ouagadougou (Burkina Faso), EM-Consulte. Consulté le: 29 février 2024. [En ligne]. Disponible sur: https://www.em-consulte.com/article/248797/les-thromboses-veineuses-cerebrales-en-milieu-hosp
- Z. Traore, O. A. Maiga, H. Diallo Seybou, S. Youssouf, D. Salimata, et M. Youssoufa. Thrombose veineuse cérébrale dans le service de neurologie du CHU Gabriel Touré. Revue Neurologique, vol. 175, p. S135, avr. 2019, doi: 10.1016/j.neurol.2019.01.354.
- E. Chilvers et P. Rudge. Cerebral venous thrombosis and subarachnoid haemorrhage in users of oral contraceptives. Br Med J (Clin Res Ed), vol. 292, no 6519, p. 524, févr. 1986.
- Subarachnoid haemorrhage: diagnosis, causes and management | Brain | Oxford Academic ». Consulté le: 29 février 2024. [En ligne]. Disponible sur: https://academic.oup.com/brain/article/124/2/249/402215
- Y. Kato et al. Subarachnoid hemorrhage as the initial presentation of cerebral venous thrombosis. Intern Med, vol. 49, no 5, p. 467‑470, 2010, doi: 10.2169/internalmedicine.49.2789.
- J. M. Ferro. Cerebral venous thrombosis. J Neuroradiol. vol. 29, no 4, p. 231‑239, déc. 2002.
- K. Munawar et al. Cavernous sinus lesions. Clin Imaging, vol. 68, p. 71‑89, déc. 2020, doi: 10.1016/j.clinimag.2020.06.029.
- S. de Bruijn, J. Stam, et L. J. Kappelle. Thunderclap headache as first symptom of cerebral venous sinus thrombosis. The Lancet, vol. 348, no 9042, p. 1623‑1625, déc. 1996. doi: 10.1016/S0140-6736(96)07294-7.
- A. Ghoneim, J. Straiton, C. Pollard, K. Macdonald, et R. Jampana. Imaging of cerebral venous thrombosis. Clin Radiol, vol. 75, no 4, p. 254‑264, avr. 2020, doi: 10.1016/j.crad.2019.12.009.
- J. L. Leach, R. B. Fortuna, B. V. Jones, et M. F. Gaskill-Shipley. Imaging of cerebral venous thrombosis: current techniques, spectrum of findings, and diagnostic pitfalls. Radiographics, vol. 26 Suppl 1, p. S19-41; discussion S42-43, oct. 2006, doi: 10.1148/rg.26si055174.