
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Gigantomastia with thyroiditis in a child: About an uncommon association
Rabiy El Qadiry; Soraya Hani*; Najwa Imad; Lagrine Mariem; Houda Nassih; Aicha Bourrahouat; Imane Ait Sabb
Department of Pediatrics, Mother and Child Hospital, Mohammed VI University Hospital, Marrakech, Morocco.
*Corresponding Author : Soraya Hani
Department of Pediatrics, Mother and Child Hospital, Mohammed VI University Hospital, Marrakech, Morocco.
Email: dr.sorayahani@gmail.com
Received : Sep 02, 2024
Accepted : Sep 20, 2024
Published : Sep 27, 2024
Archived : www.jcimcr.org
Copyright : © Hani S (2024).
Abstract
Gigantomastia is a rare condition in pediatric patients characterized by excessive breast growth.
We report the case of a female patient, 13 years old, followed up in the B pediatric department of Mohammed VI University Hospital in the year 2022, presenting a gigantomastia with Hashimoto thyroiditis, which is an uncommon association. The aim of this case report is to explain the mechanisms underlying those conditions’ association.
The patient is non-consanguineous, with no pathological history. She reported a progressive increase in the volume and size of her two breasts within the onset of the puberty, associated with hair loss, dry and friable skin, with a delayed eruption of teeth.
On clinical examination, the patient had a statural delay with a BMI of 29.5 kg/m², cervical examination did not noticed any mass in regard to a possibly goiter, and the examination of the external genital organs showed a pubis without pilosity, with gigantomastia.
The biological assessment revealed hypothyroidia with positive anti thyroperoxidase and anti thyroglobulin antibodies, and a cervical ultrasound in favour of a thyroiditis.
Breast tissue is a target tissue to several diseases, the mechanisms of breast hypertrophy are multiple, related mainly to autoimmune diseases.
Keywords: Gigantomastia; Thyroiditis; Pediatric; Morocco.
Citation: EI Qadiry R, Hani S, Imad N, Mariem L, Nassih H, et al. Gigantomastia with thyroiditis in a child: About an uncommon association. J Clin Images Med Case Rep. 2024; 5(9): 3271.
Introduction
Breast diseases are very heterogeneous and usually idiopathic, a proliferation of the breast such as juvenile hypertrophy is less common, where a rapid breast enlargement occurs during puberty, leading to physical and psychological complications [1]. The differential diagnosis of hyperplastic breast anomalies in adolescents includes pregnancy, fibrocystic disease, adolescent macromastia, virginal (or juvenile) breast hypertrophy, tumors of the breast, and excessive endogenous or exogenous hormonal levels. Malignant tumors of the breast are extremely rare in the adolescent population [2]. The observation of breast hypertrophy in patients presenting with autoimmune diseases has rarely been clearly studied, we present the case of a female adolescent having a gigantomastia associated to Hashimoto thyroiditis, to discuss the various hypotheses for the mechanisms underlying this association [3].
Case presentation
We report the case of a female patient, 13 years old, non-consanguineous, the eldest of two siblings, with no pathological history, no known history of congenital lymphedema, no recurrent ENT or respiratory infections, and no chronic constipation.
In the other hand, the patient reported a progressive increase in the volume and size of her two breasts during her puberty, associated with hair loss, dry and friable skin, with a delayed eruption of teeth.
On clinical examination, the patient was pale, with dry skin, having a good weight development (weight at 52 Kg), and a statural delay (Height at 133 cm) with a BMI of 29.5 kg/m².
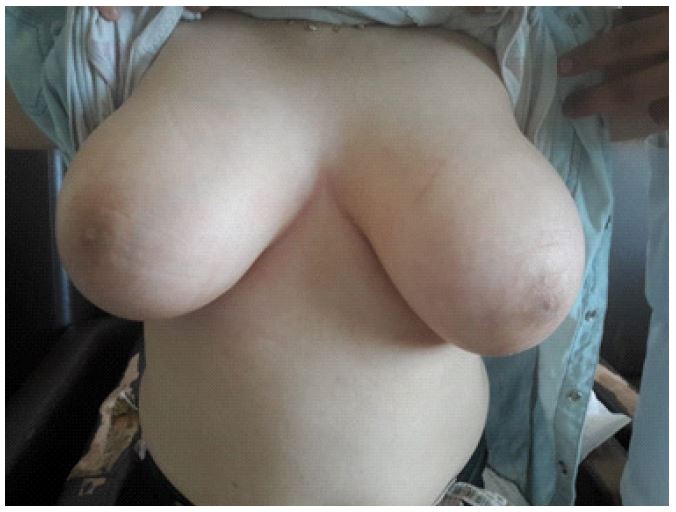
On cervical examination, we have not noticed any mass in regard to a possibly goiter, and the examination of the external genital organs showed a pubis without pilosity, with very developed breasts, a small nipple, and without any notion of breast discharge (Figures 1,2).
The biological assessment revealed a TSH of 100 uUI/mL, a T4 of 0.5 pmol/L, and a positive anti thyroperoxidase and anti thyroglobulin antibodies at a value of 5.6 UI/ml and 21.4 UI/ml respectively, the anti TG antibodies negative. The prolactin level came to a level of the estrogene, progesterone and prolactin level came at a breast ultrasound was performed and came back without any anomaly, the cervical ultrasound was in favour of a thyroiditis.
A treatment with oral Levothyroxin was initiated at a dose of 4 mg/Kg/day which leaded to a TSH of 0.005 uUI/mL and a T4 of 33.1 pmol/L after six months of treatment, with a reduction of the breast hypertrophy (Figure 3).


Discussion
Gigantomastia is a rare and disabling condition with excessive breast growth, there is no universally accepted definition of gigantomastia [4]. Breast hypertrophy appeared in a context of autoimmune or immunerelated diseases, the role of hormones as a possible promoting event remains highly probable to [3], estradiol appears as a stimulating factor, other hormones may also be involved in this process as progesterone and prolactine, these hormones are known to exert a proliferative role on epithelial mammary cells, which was not observed in our patient. The onset of breast hypertrophy is correlated with major changes in hormonal environment such as puberty as it was seen in our case.
The development of such hypertrophy in a context of immunemediated diseases, with the hormonal milieu playing a promoting role. Autoimmune mastitis has been described in the medical literature and includes a wide range of autoimmune diseases, this condition is still underdiagnosed [5].
The clinical presentation of autoimmune mastitis is variable: it can be asymptomatic as seen in our case, while others have breast inflammation, painful nodules, nipple discharge or retraction, and/or lymphadenopathy [5].
The demonstration of an immune process within the breast was evidenced by immunohistochemical analysis of breast tissue. Histological features were very close to those observed in diabetic mastopathy [6], myasthenia, Sjogren syndrome [7], systemic lupus erythematosus [8], mixed connective tissue disease [9], or dysthyroidia Graves-Basedow disease [10-12] with either Graves-Basedow disease or Hashimoto’s thyroiditis as reported in our patient. Other associations have also been described such as systemic granulomatous diseases and vasculitis [5].
A high incidence of thyroid abnormalities has been reported; in particular, thyroid antimicrosomal antibody titer elevated in about 50% of patients [10] as seen in our patient.
Hashimoto thyroiditis associated to gigantomastia shows histological features as lymphocytic mastitis, Boullu & al. reported histological pattern of diabetic mastopathy and associated autoimmune thyroiditis, and found that the disease, designated a fibrous mastopathy with perivascular and periductal lymphocytic infiltration [13]. Soler & al also demonstrated a fibrotic breast parenchyma in 5 of 12 women having thyroiditis and type I diabetes mellitus, presenting autoimmunity as a relating factor [10]. We did not perform a breast biopsy on our patient.
Hence the most characteristic pathologic feature is circumscribed perilobular and perivascular lymphocytic aggregates with increased expression of class II Human Leukocyte Antigens (HLA) by the lobular and ductal epithelium combined incidence of HLA-DR 3, 4, and 5 [10,14]. Increased HLA-DR expression and association with other autoimmune diseases support the view that this disease entity has an autoimmune pathogenesis [14].
Conclusion
Physicians should be aware of autoimmune mastitis; any autoimmune diseases can target the mammary glands. An early diagnosis of this condition can avoid unnecessary repeated breast biopsies or surgery, and initiate specific treatments, thereby improving the prognosis and the evolution of the disease.
References
- E M Wolfswinkel, V Lemaine, WM Weathers, C J Chike-Obi, A S Xue, et al. Hyperplastic Breast Anomalies in the Female Adolescent Breast. Semin. Plast. Surg. 2013; 27(1): 49‑55. doi: 10.1055/s-0033-1347167.
- S Pruthi, K N Jones, J C Boughey, P S Simmons, et al. Breast masses in adolescents: Clinical pearls in the diagnostic evaluation. Am. Fam. Physician. 2012; 86(4): 325‑326.
- P Touraine, et al. Breast inflammatory gigantomastia in a context of immune-mediated diseases. J. Clin. Endocrinol. Metab. 2005; 90(no 9): 5287‑5294. doi: 10.1210/jc.2005-0642.
- H Dafydd, K R Roehl, L G Phillips, A Dancey, F Peart, et al. Redefining gigantomastia. J. Plast. Reconstr. Aesthet. Surg., vol. 64, no 2, p. 160‑163, févr. 2011, doi: 10.1016/j.bjps.2010.04.043.
- R Goulabchand, et al. Mastitis in Autoimmune Diseases: Review of the Literature, Diagnostic Pathway, and Pathophysiological Key Players. J. Clin. Med. 2020; 9(no4): 958. doi: 10.3390/jcm9040958.
- D Fong, M A Lann, C Finlayson, D L Page, M Singh, et al. Diabetic (lymphocytic) mastopathy with exuberant lymphohistiocytic and granulomatous response: A case report with review of the literature, Am. J. Surg. Pathol. 2006; 30(no 10): 1330‑1336. doi: 10.1097/01.pas.0000213284.27789.a8.
- R Goulabchand, et al. Mastitis associated with Sjögren’s syndrome: A series of nine cases. Immunol. Res. 2017; 65(no 1): 218‑229. doi: 10.1007/s12026-016-8830-x.
- Y Tanaka, H Manabe, W Shinzaki, Y Hashimoto, Y Komoike, et al. A case of lupus mastitis in a patient with systemic lupus erythematosus. Breast J. 2020; 26 (no 4): 780‑781. doi: 10.1111/tbj.13582.
- Breast involvement in mixed connective tissue disease - PubMed. 2022. https://pubmed.ncbi.nlm.nih.gov/30701011/ (consulté le 23 janvier 2022).
- N G Soler, R Khardori, et al. Fibrous disease of the breast, thyroiditis, and cheiroarthropathy in type I diabetes mellitus. Lancet Lond. Engl. 1984; 1no 8370: 193‑195. doi: 10.1016/s0140-6736(84)92114-7.
- M Dubenko, D Breining, M I Surks, et al. Sclerosing lymphocytic lobulitis of the breast in a patient with Graves’ disease. Thyroid Off. J. Am. Thyroid Assoc. 2003; 13(no3): 309‑311. doi: 10.1089/105072503321582141.
- S H Park, S J Choi, H K Jung, et al. Sclerosing Lymphocytic Lobulitis Manifesting as Suspicious Microcalcifications with Hashimoto’s Thyroiditis in a Young Woman », Breast J, p. n/a-n/a. 2013. doi: 10.1111/tbj.12156.
- S Boullu, L Andrac, L Piana, P Darmon, A Dutour, et al. Diabetic mastopathy, complication of type 1 diabetes mellitus: Report of two cases and a review of the literature, Diabetes Metab. 1998; 24(no5): 448‑454.
- G A Lammie, L G Bobrow, M D Staunton, D A Levison, G Page, et al. Sclerosing lymphocytic lobulitis of the breast-evidence for an autoimmune pathogenesis. Histopathology. 1991; 19(no1): 13‑20. doi: 10.1111/j.1365-2559.1991.tb00889.x.