
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
First reported case of old world leishmaniasis in Greece affecting the oral mucosa
Olga S Koutsoni1; Sofia Makka2; Maria Evangelidou2; Evi Tsoutsoura3; Vassilis Filiopoulos3; Danai Pervanidou4; Smaragdi Marinaki3; Emmanouil Angelakis2; Despina Smirlis1,5*
1National Reference Laboratory for Leishmaniasis, Hellenic Pasteur Institute, 127 Vas. Sofias Avenue, 115 21, Athens, Greece.
2Diagnostic Department and Public Health Laboratories, Hellenic Pasteur Institute, Athens, Greece.
3Department of Nephrology & Renal Transplantation, National and Kapodistrian University of Athens, Laiko General Hospital, Athens, Greece.
4National Public Health Organization (EODY), 151 23 Athens, Greece.
5Molecular Parasitology Laboratory, Hellenic Pasteur Institute, Athens, Greece.
*Corresponding Author : Despina Smirlis
National Reference Laboratory for Leishmaniasis, Hellenic Pasteur Institute, 127 Vas. Sofias Avenue, 115 21, Athens, Greece.
Tel: +30-2106478841;
Email: penny@pasteur.gr
Received : Sep 03, 2024
Accepted : Sep 20, 2024
Published : Sep 27, 2024
Archived : www.jcimcr.org
Copyright : © Smirlis D (2024).
Abstract
Background: Leishmaniasis is an important infectious disease caused by kinetoplastid protozoan parasites of the genus Leishmania, transmitted to mammalian hosts by the bite of infected female phlebotomine sandflies. The clinical manifestations of the disease are broadly classified into three types: Visceral (VL), Cutaneous (CL), and Mucocutaneous (MCL) leishmaniasis, depending on the Leishmania species. Mucosal Leishmaniasis (ML) is a rare metastatic complication of Leishmania infection, presenting destructive and disfiguring outcomes of the nasal architecture and an airway compromise. Oral manifestations of leishmaniasis usually occur from infection by New World Leishmania species, while is an uncommon form of the disease in the Old World.
Case presentation: We present the first to our knowledge report of leishmaniasis with oral mucosa symptoms, in Greece. The causative species was identified as Leishmania infantum. The patient presented concurrent visceral symptoms and was a renal-transplanted patient with a previous medical history of leishmaniasis.
Conclusions: Overall, leishmaniasis with oral manifestations merits awareness towards differential diagnosis of oral lesions, in regions of the Old World where Leishmania spp. are endemic, including the Mediterranean basin where Leishmania infantum is prevalent.
Keywords: Oral mucosal leishmaniasis; Leishmania infantum; Greece; Diagnosis.
Citation: Smirlis D, Koutsoni OS, Makka S, Evangelidou M, Tsoutsoura E, et al. First reported case of old world leishmaniasis in Greece affecting the oral mucosa. J Clin Images Med Case Rep. 2024; 5(9): 3272.
Background
Leishmaniasis is a vector-borne complex of diseases caused by the bite of Phlebotomus and Lutzomyia female sandflies transmitting Leishmania (L.) parasites, the causative agents of the disease. Leishmaniasis is a growing public health concern as it has a worldwide distribution, being endemic in circumscribed geographic areas in Africa, Southern Europe, Middle East, and Central and South America [1]. An estimated 1 million new cases are reported annually from nearly 100 endemic countries, while about 15 million people are infected and 350 million are at risk of acquiring the disease [1]. Major risk factors are associated with the increase in incidence and prevalence of leishmaniasis, such as environmental conditions, socio-economic status, demographic and human behaviors like great migration, deforestation, urbanization and immunosuppression [2].
The clinical features of the disease include a wide range of manifestations with various degrees of severity that depend on the involved parasite species and the host’s immune response [3]. Despite the variety of clinical symptoms, there are three main manifestations. Cutaneous Leishmaniasis (CL), is the most common form of the disease, which causes self-curing skin lesions [3]. Visceral Leishmaniasis (VL) is the most severe form which affects host’s visceral organs, mainly the liver and the spleen, and is associated with high fatality if left untreated [3]. At last, Mucosal Leishmaniasis (ML) is a rare and serious condition typically affecting the larynx, pharynx, inner nostril wall and oral cavity [3]. The lesions may cause severe facial disfigurement and can lead to severe deformity if left untreated [4]. Several factors promote the ML onset, such as malnutrition, male sex and immunosuppression [5]. It is largely confined to regions of Central and South America, where more than 90% of ML cases are reported, and parasites that belong to the New World L. Vianna subgenus (L. braziliensis, L. panamensis, L. guyanensis, L. peruviana) are considered the main aetiological agents [4,6]. Even though the great majority of ML cases occur in America, an increased incidence is very likely to occur in other regions of the world, due to environmental and anthroponotic changes. The Old World Leishmania subgenus, notably from L. donovani complex (L. donovani and L. infantum) and L. tropica complex parasites (L. tropica and L. major), causing Visceral (VL) and Cutaneous (CL) Leishmaniasis respectively [6], is rarely suspected as a causative agent of ML, leading to remarkable delays in diagnosis and treatment.
In this manuscript, we report the first case of leishmaniasis in Greece, caused by Leishmania infantum, which affected the oral mucosa of an immunocompromised patient. Leishmania infantum is the basic autochthonous species of southern Europe, including Greece, causing VL. ML is a rare and unusual clinical presentation of an L. infantum infection and should be considered in the differential diagnosis in endemic regions [6-9].
Case presentation
In April 2023, a 61-year-old male patient presented symptoms of gingival hyperplasia in the oral cavity, and a deciduous febrile movement. At the time of the symptoms, the patient was receiving immunosuppressive therapy with mycophenolic acid (560 mg twice a day), tacrolimus (5-6 mg) and methylprednisolone (4 mg). His medical history included end-stage renal disdisease due to chronic glomerulonephritis, and renal transplantation in 2011. In 2014, the patient had displayed gastrointestinal manifestations and a colon biopsy test revealed a Leishmania infection. Blood PCR, bone-marrow biopsies and antibody rK39 dipstick test were negative. The patient recovered after treatment with Liposomal -Amphotericin B (L-AMB) administered for three weeks (cumulative dose 20 mg/kg).
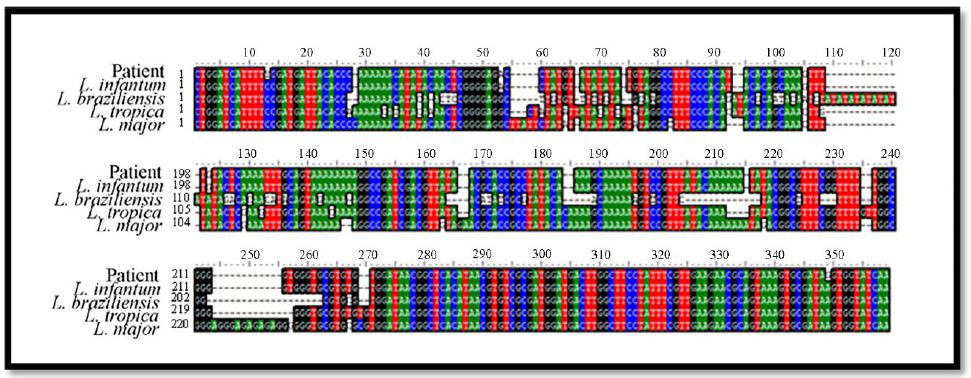
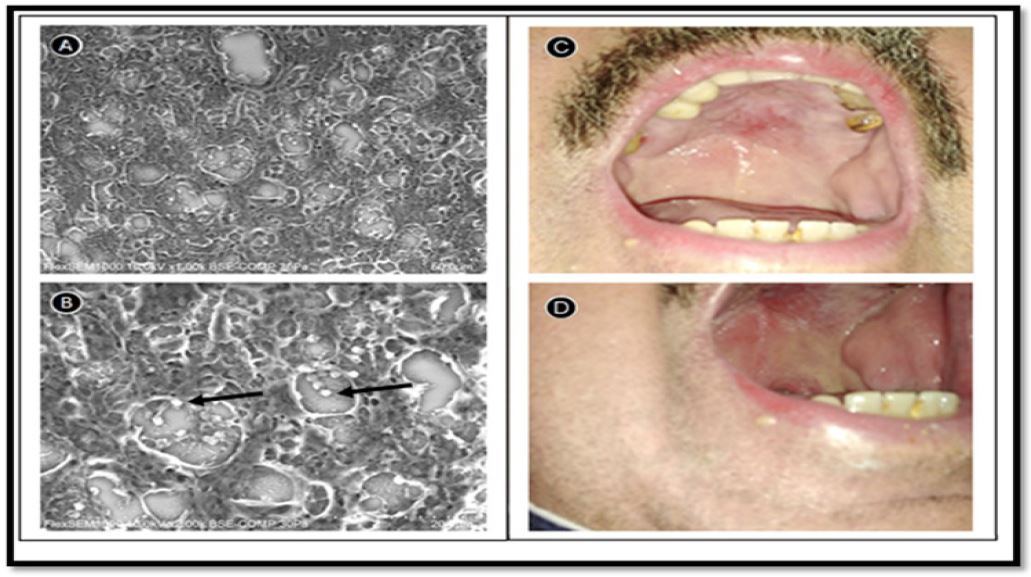
In order to investigate the patient’s gingival hyperplasia, a biopsy was performed. The histological examination of gingival tissue revealed intense inflammatory infiltration and the presence of Giemsa-positive microorganisms within the cytoplasm of macrophages. Thus, a possible Leishmania infection was suspected and the patient was hospitalized. Blood tests also revealed mild pancytopenia, while abdominal ultrasound confirmed splenomegaly (~14.3 cm diameter). A blood sample and a tissue sample from the gingival lesion were sent to the Hellenic National Reference Laboratory for Leishmaniasis for further diagnosis and confirmation of leishmaniasis and for molecular investigation of the causative species. DNA was extracted using the QIAamp DNA Mini Kit (Qiagen). Samples were handled under sterile conditions and were analyzed by quantitative real-time PCR targeting kinetoplast DNA [10]. Leishmania typing was performed by sequencing of the amplified Internal Transcribed Spacer 1 (ITS-1) product of PCR, as previously described [11]. The causative Leishmania species was identified as Leishmania infantum (Figure 1). In addition, the diagnosis of leishmaniasis was also performed by histology methods with detection of the parasites in the gingival lesion, were they were visualized as amastigotes, by variable pressure scanning electron HG microscopy (Figure 2A and 2B). Based on the leishmaniasis diagnosis, the patient was assigned to an intravenous L-AMB regimen, with a cumulative dose of 40 mg/kg for five weeks, followed by a reduction of the immunosuppressive therapy (360 mg mycophenolic acid, twice a day, 4 mg tacrolimus).
At the end of the antileishmanial treatment, fever regression was noticed and the spleen was determined with normal dimensions. Bone marrow histopathology test did not reveal pathological findings and the imaging of the chest and abdomen with a CT scan, was normal. As part of the checkup, a colonoscopy was performed, which revealed findings of colitis. Histological lesions were associated with a positive Cytomegalovirus (CMV) diagnostic test, negative for Leishmania infection. After the CMV diagnosis, the patient was additionally treated with valganciclovir for three weeks, while mycophenolic acid was reduced to 250 mg twice a day, and the dose of methylprednisolone was increased (6 mg) to protect the transplant. Due to persistent gingival hyperplasia (Figure 2C and 2D), the treatment with L-AMB continued for up to one year.
Discussion and conclusions
To the best of our knowledge, this is the first reported case of the rare Leishmania infantum leishmaniasis in a kidney-transplanted patient, with oral mucosal manifestations, in Greece. The patient presented also concurrent visceral manifestations. His medical history involved leishmaniasis affecting the colon nine years before the onset of the mucosal symptoms, although it is not clear if the subsequent mucosal manifestations represent a relapse or a new infection. It is noteworthy that immunosuppressed patients are at the greatest risk of leishmaniasis infection and reactivation [12]. Leishmania infantum leishmaniasis affecting the mucosal cavity is extremely rare in Europe and a recent surveillance of the disease in 15 European centers revealed that 5% of autochthonous infections caused ML [13]. In addition, there are reviews, which describe predisposing factors, including male sex and immunodeficiency that match this case report [14,15]. The majority of Leishmania infantum ML cases present localized lesions with no concurrent visceral disease [14,15], unlike the presented case report where the patient combined both mucosal and visceral symptoms. Factors allowing this concurrency of mucosal and visceral symptoms [16] may be attributed either to parasite factors and/or to the immune system of the host. Consequently, doctors in the Mediterranean basin, due to the presence of viscerotropic L. infantum, should suspect both forms of the disease. In this particular case, apart from the existing immunodeficiency, the CMV infection may have additionally affected the patient’s immune system, contributing to this rare manifestation. Overall, this report should raise the awareness of clinicians in the Mediterranean region for including ML in the differential diagnosis of oral mucosal lesions and for investigating the coexistence of visceral disease, especially in immunocompetent and immunocompromised individuals living in endemic areas or reporting travels to endemic areas.
Declarations
Acknowledgments: Not applicable.
Author contributions: Conceptualization was performed by D. S. and E.A. E.T., V.F., and Sm. M. treated the patient. D.S., E.T., V.F., So. M., M.E., E.A., and O.S.K. performed the data collection. O. S. K., So. M., and M. E. performed laboratory work and analysis. D.S., O.S.K., and D. P. analyzed the data. O.S.K. and D.S. contributed to the writing of the manuscript. All the authors drafted and approved the published version of the manuscript.
Funding: Leishmania molecular diagnosis and typing were funded by the Hellenic National Public Health Organization. The views and opinions expressed in this publication are solely those of the authors, and they do not purport to reflect the opinions, views or positions of the Hellenic Public Health Organization.
Data availability: The data that support the findings of this report are available from the corresponding author, upon reasonable request.
Ethical approval: The patient has given his written consent for publishing this case report with photographs.
Conflicts of Interest: The authors declare that they have no conflicts of interests.
References
- Torres-Guerrero E, Quintanilla-Cedillo M R, Ruiz-Esmenjaud J, Arenas R. Leishmaniasis: A review. F1000Res. 2017; 6: 750.
- Oryan A, M Akbari. Worldwide risk factors in leishmaniasis. Asian Pac J Trop Med. 2016; 9(10): 925-932.
- Mann S, Frasca K, Scherrer S, Henao-Martinez A F, Newman S, et al. A Review of Leishmaniasis: Current Knowledge and Future Directions. Curr Trop Med Rep. 2021; 8(2): 121-132.
- Strazzulla A, Cocuzza S, Pinzone M R, Postorino M C, Cosentino S, et al. Mucosal leishmaniasis: An underestimated presentation of a neglected disease. Biomed Res Int. 2013; 805108.
- Gianchecchi E, E Montomoli. The enemy at home: Leishmaniasis in the Mediterranean basin, Italy on the focus. Expert Review of Anti-Infective Therapy. 2020; 18(6): 563-577.
- Burza S, SL Croft, M Boelaert. Leishmaniasis. Lancet. 2018; 392(10151): 951-970.
- Ntais P, Sifaki-Pistola D, Christodoulou V, Messaritakis I, Pratlong F, et al. Leishmaniases in Greece. Am J Trop Med Hyg. 2013; 89(5): 906-15.
- Maia C, Conceicao C, Pereira A, Rocha R, Ortuno M, et al. The estimated distribution of autochthonous leishmaniasis by Leishmania infantum in Europe in 2005-2020. PLoS Negl Trop Dis. 2023; 17(7): e0011497.
- Gouzelou E, Haralambous C, Amro A, Mentis A, Pratlong F, et al. Multilocus microsatellite typing (MLMT) of strains from Turkey and Cyprus reveals a novel monophyletic L. donovani sensu lato group. PLoS Negl Trop Dis. 2012; 6(2): e1507.
- Mary C, Faraut F, Lascombe L, Dumon H. Quantification of Leishmania infantum DNA by a real-time PCR assay with high sensitivity. J Clin Microbiol. 2004; 42(11): 5249-55.
- El Tai N O, Osman O F, El Fari M, Presber W, Schonian G. Genetic heterogeneity of ribosomal internal transcribed spacer in clinical samples of Leishmania donovani spotted on filter paper as revealed by single-strand conformation polymorphisms and sequencing. Trans R Soc Trop Med Hyg. 2000; 94(5): 575-9.
- Grech P, S M Vella, T Piscopo. Leishmania donovani mucosal leishmaniasis in Malta. BMJ Case Rep. 2020; 13(11).
- Van der Auwera G, Davidsson L, Buffet P, Ruf M T, Gramiccia M, et al. Surveillance of leishmaniasis cases from 15 European centres, 2014 to 2019: A retrospective analysis. Eurosurveillance. 2022; 27(4).
- Faucher B, Pomares C, Fourcade S, Benyamine A, Marty P, et al. Mucosal Leishmania infantum leishmaniasis: Specific pattern in a multicentre survey and historical cases. J Infect. 2011; 63(1): 76-82.
- Aliaga L, Cobo F, Mediavilla J D, Bravo J, Osuna A, et al. Localized mucosal leishmaniasis due to Leishmania (Leishmania) infantum: Clinical and microbiologic findings in 31 patients. Medicine (Baltimore). 2003; 82(3): 147-58.
- Picarda G, C A Benedict. Cytomegalovirus: Shape-Shifting the Immune System. J Immunol. 2018; 200(12): 3881-3889.