
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Early dysfunction of mitral bioprostheses: A challenge in identifying the underlying mechanisms
Hele Viorel-George; Sara Sary Eldim Campanati; Luis Henrique Coelho Pinto; Thiago Pinheiro Junqueira; Lilian Paula de Souza; Sara Regina Silva Cupertino; Gustavo Brandao de Oliveira; Carolina Kuchenbecker Soares; Renato Braulio; Maria Carmo Pereira Nunes*
Department of Internal Medicine, School of Medicine of the Federal University of Minas Gerais, Av, Professor Alfredo Balena, 190, Santa Efigênia, 30130 100 - Belo Horizonte, MG, Brazil.
*Corresponding Author : Pereira Nunes MC
Department of Internal Medicine, School of Medicine of the Federal University of Minas Gerais, Av, Professor Alfredo Balena, 190, Santa Efigênia, 30130 100 - Belo Horizonte, MG, Brazil.
Tel: +55-31-34099746 & +55-31-34099437;
Email: mcarmo@waymail.com.br
Received : Sep 03, 2024
Accepted : Sep 23, 2024
Published : Sep 30, 2024
Archived : www.jcimcr.org
Copyright : © Pereira Nunes MC (2024).
Abstract
Introduction: Bioprosthetic Valve Dysfunction (BVD) and Bioprosthetic Valve Failure (BVF) can be divided into structural valve deterioration, non-structural valve dysfunction, thrombus and endocarditis. BVF is a clinical consequence of BVD, leading to both morphological and hemodynamic deterioration, often requiring reintervention.
Objective: This case report aims to explore the mechanisms contributing to BVD.
Methods: The method used was clinical observation of the patient’s progress following bioprosthetic valve implantation, coupled with imaging assessments and histopathological analysis of the explanted prosthesis to assess the underlying causes of BVD.
Conclusion: Accelerated degradation of bioprosthetic valves can occur in some patients, driven by factors such as the host’s immune response, valve thrombosis, or endocarditis. However, accurately identifying patients at higher risk for rapid degradation and determining the exact underlying cause remain significant challenges.
Keywords: Rheumatic heart disease; Valve replacement; Valve dysfunction; Valve failure; Bioprosthetic valve.
Citation: Pereira Nunes MC, Viorel-George H, Eldim Campanati SS, Coelho Pinto LH, Pinheiro Junqueira T, et al. Early dysfunction of mitral bioprostheses: A challenge in identifying the underlying mechanisms. J Clin Images Med Case Rep. 2024; 5(9): 3273.
Introduction
Bioprosthetic Valve Dysfunction (BVD) and Bioprosthetic Valve Failure (BVF) can be classified into four categories: Structural Valve Deterioration (SVD), non-structural valve dysfunction, endocarditis, and thrombus formation. BVF represents a clinical endpoint of BVD and is characterized by the presence of one or more of the following criteria: 1) Any BVD with clinically significant manifestations, such as new or worsening symptoms, left ventricular dilation/hypertrophy/dysfunction, or pulmonary hypertension; 2) Irreversible Stage 3 BVD confirmed through imaging that demonstrates leaflet or stent abnormalities and invasive assessments corroborating BVD; 3) The need for reintervention based on hemodynamic or symptomatic indications; or 4) Valve-related mortality [1].
Non-structural valve dysfunction refers to valve dysfunction resulting from external factors unrelated to the structural integrity of the valve prosthesis itself, leading to hemodynamic disturbances. Examples include paravalvular regurgitation, subvalvular pannus overgrowth, improper valve positioning (due to procedural misplacement or post-implantation migration), prosthesis size mismatch (either under- or oversizing), and prosthesis-patient mismatch [2].
Structural valve deterioration, in contrast, involves intrinsic degenerative changes in the valve’s components, including the bioprosthetic leaflets, stent, sewing ring, or struts. Common structural complications include leaflet tears or disruption, flail leaflets, leaflet fibrosis, calcification, thickening, and fractures or deformities of the stent or supporting structures [3].
Thrombosis typically occurs shortly after valve implantation, particularly in suboptimal anticoagulation settings, and is more commonly associated with mechanical prostheses. However, it can also develop in bioprosthetic valves, sometimes manifesting long after the initial implantation [3].
Bioprosthetic valve endocarditis is diagnosed when there is evidence of infective endocarditis, primarily based on the Duke criteria, including the presence of abscesses or vegetations. Endocarditis frequently results in both morphological and hemodynamic deterioration of the valve, often requiring treatment with intravenous antibiotics. In more severe cases, where BVF occurs, surgical intervention may be necessary [4].
In this case report, we detail the clinical course of a patient with rheumatic heart disease who underwent both aortic and mitral bioprosthetic valve replacements. One year after surgery, the patient developed mitral BVF, likely due to thrombus formation and pannus overgrowth.
Presentation of the case
A 65-year-old patient with rheumatic heart disease underwent mitral and aortic valve replacement with biological prostheses in March 2023. She had been on oral anticoagulants following an acute arterial occlusion in the lower limbs in November 2023. However, anticoagulation therapy was discontinued after an episode of oral cavity bleeding in May 2024.
Subsequently, the patient began experiencing dyspnea classified as functional class III/IV after the discontinuation of anticoagulants. She sought care at an emergency department and was initially treated with antibiotics, with no improvement of her symptoms.
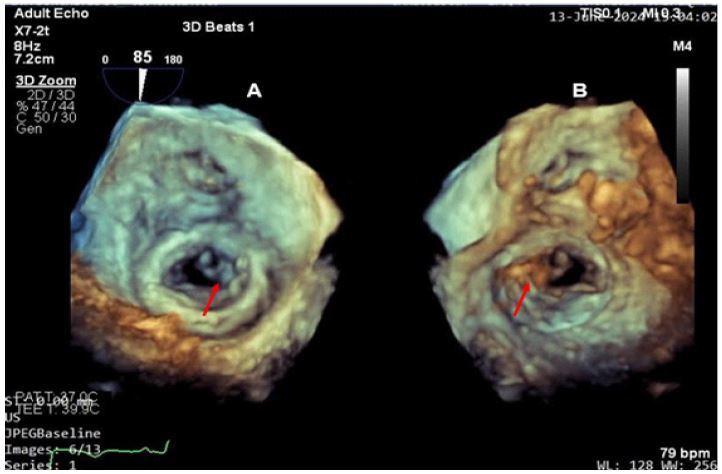
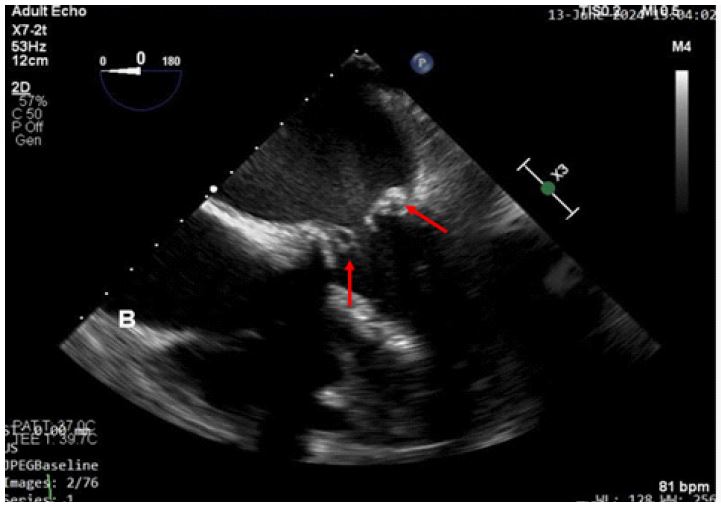
In June 2024, a routine transthoracic echocardiogram revealed severe dysfunction of the mitral prosthesis, characterized by elevated mean gradients. The patient was then admitted in the hospital for further investigation. A follow-up transesophageal echocardiogram demonstrated thickening of the mitral prosthesis leaflets (Figures 1 and 2), with one leaflet showing complete immobility, another exhibiting partial restriction, and only one leaflet maintaining adequate mobility. Additionally, an echogenic mass was noted on the ventricular surface of one of the leaflets. The mean gradient was 24 mmHg.
Suspecting thrombus formation, thrombolysis with Alteplase (four doses) was attempted, but the elevated gradients across the prosthesis persisted, progressing to right ventricular dysfunction due to severe pulmonary hypertension with Systolic Pulmonary Artery Pressure (SPAP) of 89 mmHg. Consequently, the patient underwent a second mitral valve replacement surgery on August 2, 2024, with a biological prosthesis (Figure 3).
The explanted prosthesis (Figure 4) was sent for histopathological examination, which revealed areas of cellular fragmentation and destruction of collagen fibers in various regions, accompanied by detachment of endocardial tissue. Slightly prominent thrombosis and fibrin deposits were also observed. No signs of inflammatory activity were detected.


The patient demonstrated good progress in the postoperative period, with an echocardiogram showing a bioprosthetic mitral valve with adequate leaflet mobility and a reduction in SPAP and improvement of right ventricular function. The patient was discharged from the hospital 10 days after surgery.
Discussion
In this report, we present the case of a patient who underwent mitral bioprosthetic valve replacement due to rheumatic valve disease and subsequently developed prosthetic dysfunction 16 months later. A transthoracic echocardiogram revealed elevated mean gradients across the prosthesis and an echogenic mass on the ventricular surface of one of the leaflets.
Prosthetic valve dysfunction can be divided into structural valve deterioration, non-structural valve dysfunction, endocarditis and thrombus [1]. The age of the prosthesis, anatomical and hemodynamic aspects, as well as the patient’s clinical characteristics can reveal the most plausible underlying cause and guide clinical decision-making [4]. Prosthetic valve dysfunction may be suspected in a recently symptomatic patient or it can be detected with routine echocardiography.
After adequate clinical evaluation, echocardiography is the main technique used to confirm the diagnosis of prosthetic valve dysfunction, as well as to assess its severity and prognosis [3]. Transesophageal echocardiography should be performed for etiologic definition, especially for mitral prostheses [5].
Valve obstruction is a serious complication in patients with prosthetic heart valves and can be associated with significant morbidity and mortality. Stenosis of a bioprosthetic may occur due to progressive structural degeneration of the valve, through the formation of pannus, or it may occur due to thrombus formation on the valve cusps, despite bioprosthetic valves being less thrombogenic than mechanical. Distinguishing between thrombus formation and pannus based on clinical signs can be difficult. The duration of symptoms, anticoagulation status and the qualitative and quantitative ultrasound intensity of the mass in a mechanical prosthetic valve can help in this differentiation [6].
Once the etiological diagnosis of prosthesis stenosis has been established, treatment will be based on the patient’s NYHA functional class, the presence of embolism, the availability of surgery, the possible contraindications of each therapeutic option and local experience [6]. In cases of prosthetic thrombosis, fibrinolysis can be considered surgery as it is not an option, but it presents a risk of bleeding and thromboembolism. Emergency valve replacement is recommended for obstructive prosthetic valve thrombosis in seriously ill patients who have no contraindication to surgery [4,7].
Conclusion
Early dysfunction of bioprostheses is a serious complication and distinguishing between differential diagnoses is essential for adequate treatment. Diagnosis of the etiology of valve dysfunction is challenging due to the general lack of knowledge of the disease and the lack of formal echocardiographic diagnostic criteria. Therefore, a clinical-echocardiographic correlation is necessary to make the correct diagnosis of this condition.
Conflict of interest: I declare not to be associated with any type of conflict of interest between the participants or any other collaborator, direct or indirect, for the development of this case report.
References
- Pibarot P, Herrmann HC, Wu C, Hahn RT, Otto CM, et al. Heart Valve Collaboratory. Standardized Definitions for Bioprosthetic Valve Dysfunction Following Aortic or Mitral Valve Replacement: JACC State-of-the-Art Review. J Am Coll Cardiol. 2022; 80(5): 545-561. doi: 10.1016/j.jacc.2022.06.002.
- Barbetseas J, Nagueh SF, Pitsavos C, et al. Differentiating thrombus from pannus formation in obstructed mechanical prosthetic valves: An evaluation of clinical, transthoracic and transesophageal echocardiographic parameters. J Am Coll Cardiol. 1998; 32: 1410-1417.
- Fazzari F, Baggiano A, Fusini L, Ghulam Ali S, Gripari P, et al. Early Biological Valve Failure: Structural Valve Degeneration, Thrombosis, or Endocarditis? J Clin Med. 2023; 12(17): 5740. doi: 10.3390/jcm12175740. PMID: 37685807.
- Vahanian A, et al. ESC/EACTS Guidelines for the management of valvular heart disease: Developed by the Task Force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). European Heart Journal. 2021; ehab395.
- Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP 3rd, et al. ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021; 143(5): e35-e71. doi: 10.1161/CIR.0000000000000932. Erratum in: Circulation. 2021; 143(5): e228. doi: 10.1161/CIR.0000000000000960. Erratum in: Circulation. 2021; 143(10): e784. doi: 10.1161/CIR.0000000000000966.
- Kostyunin AE, Yuzhalin AE, Rezvova MA, Ovcharenko EA, Glushkova TV, et al. Degeneration of Bioprosthetic Heart Valves: Update. J Am Heart Assoc. 2020; 9(19): e018506. doi: 10.1161/JAHA.120.018506.
- Bonou M, Lampropoulos K, Barbetseas J. Prosthetic heart valve obstruction: thrombolysis or surgical treatment? Eur Heart J Acute Cardiovasc Care. 2012; 1(2): 122-7. doi: 10.1177/2048872612451169.