
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Pyogenic liver abscess with massive intravascular hemolysis
Diana Tavares Aguiar1*; Daniel Martins2; Erico Costa1; Diana Adriao1; Isabel Pereira1
1Intensive Care Department, Unidade Local de Saude de Gaia/Espinho, Vila Nova de Gaia, Portugal.
2General Surgery Department, Unidade Local de Saude de Gaia/Espinho, Vila Nova de Gaia, Portugal.
*Corresponding Author : Diana Tavares Aguiar
Intensive Care Department, Unidade Local de Saude de Gaia/Espinho, Vila Nova de Gaia, Portugal.
Email: diana.aguiar@ulsge.min-saude.pt
Received : Sep 05, 2024
Accepted : Sep 23, 2024
Published : Sep 30, 2024
Archived : www.jcimcr.org
Copyright : © Aguiar DT (2024).
Abstract
Pyogenic liver abscesses are rare, caused mostly by Enterobacteriaceae and anaerobes. Liver abscesses caused by Clostridium perfringens commonly exhibit a strong association with extensive hemolysis and multiorgan failure, resulting in a high mortality rate, especially in immunocompromised individuals. The authors describe a case of liver abscess in a patient without any identified risk factors and no clinical or radiologic suspicious findings upon admission. The patient’s condition rapidly deteriorated and he developed multiorgan failure less than 30 hours after admission, despite intensive care admission and early antibiotic therapy. Although two microorganisms were identified, the clinical course and laboratorial findings are highly suggestive of Clostridium perfringens being the main bacteria accountable for patient’s semiology and evolution. A review of relevant literature ensues, emphasizing the diagnostic and therapeutic challenges encountered in such patients.
Keywords: Pyogenic liver abscess; Clostridium perfringens; Massive intravascular hemolysis; Critically ill patient.
Citation: Tavares Aguiar D, Martins D, Costa E, Adriao D, Pereira I. Pyogenic liver abscess with massive intravascular hemolysis. J Clin Images Med Case Rep. 2024; 5(9): 3274.
Introduction
Background: Pyogenic Liver Abscesses (PLA) are rare conditions with variable incidence rates, which depend on geographical distribution. They predominantly affect males between the ages of 50 and 60 years old [1,2].
PLA can originate from various sources, namely the biliary tract (associated with biliary tract cancer, choledocholithiasis, cholangitis), arterial dissemination (occurring with hepatic artery thrombosis, following intra-arterial procedures such as chemoembolization or radiofrequency ablation, or also bacteremia), portal dissemination (arising from infections in the digestive tract or pelvic region, often leading to right-sided abscesses), direct extension (such as subphrenic or perirenal abscesses or cholecystitis), traumatic injury, or cryptogenic causes.
Most liver abscesses occur as solitary nodules, primarily in the right lobe [3]. The microbiology of these abscesses varies depending on the etiology and regions. In Western countries, the main causative agents are Escherichia coli, Klebsiella pneumoniae, Enterococcus species, and Streptococcus species, similar to the findings of a Portuguese review conducted in 2006 with the majority of isolates being E. coli, followed by Streptococci, and only a quarter of the cases being polymicrobial [4].
PLA caused by Clostridium are rare and have high mortality due to their rapid bacterial replication and virulence mechanisms. Clostridium species are known to produce six types of toxins (alpha, beta, epsilon, gamma, enterotoxin, and necrotizing enterotoxin) and are classified into seven classes based on the toxins they produce [5]. Beside the exponential growth rate, one of the key factors contributing to the significant morbidity and mortality of Clostridium infections in humans is its ability to induce intravascular hemolysis, attributed to the alpha toxin (a type of phospholipase C, also responsible for the clostridial myonecrosis) and accountable for major mortality increase [6-8]. The diagnosis of Clostridium abscesses relies on a high clinical suspicion along with supportive laboratory and imaging find ings, namely evidence of massive hemolysis, rapid progression to metabolic acidosis, and respiratory failure, and eventually Clostridium identification in cultures.
Treatment of Clostridium abscesses involves antibiotic therapy, typically consisting of beta-lactam (penicillin being one of the most effective [7]) and clindamycin, with studies showing that metronidazole and clindamycin are effective in inactivating the alpha toxin [9]. It is crucial to address the source of the infection through invasive focus control. Additional therapies mentioned in the literature include hyperbaric oxygen therapy [7,10,11], as well as the use of antitoxins and anti-interleukin-6 (IL-6) in animal studies [12,13].
Also rare, liver abscesses caused by Haemophilus parainfluenzae are serious conditions, presenting low mortality rate when promptly treated. They typically respond well to antibiotic therapy, commonly employing cephalosporins and metronidazole [14,15]. The hepatobiliary system is the most likely source of infection, due to the abundance of factor V in the digestive tract, a growth factor for Haemophilus parainfluenzae, and the adherence of its outer membrane proteins to the intestinal mucosa, making it a habitual colonizer of the duodenum [16].
Case presentation
A male patient in his mid 50’s with a history of arterial hypertension and dyslipidemia presented to the Emergency Department (ED) with symptoms of epigastric pain, dyspepsia, and intermittent heartburn, which had been ongoing for approximately 14 days but worsened on the day of admission. Physical examination revealed tenderness in the upper and middle abdominal quadrants without signs of peritonitis. The patient was afebrile and hemodynamically stable. Laboratory tests showed elevated lipase levels (206 IU/l, normal range 13-60 IU/l), with no other significant abnormalities, such as elevated C-reactive protein or leukocytosis. Abdominal ultrasound revealed moderate to severe hepatic steatosis and two hepatobiliary cysts, one of which displayed thin internal septa.
Approximately 5 hours after arriving at the ED the patient was admitted in a general ward for observation. Over the next 12 hours, he developed mild tachycardia (heart rate of 110 bpm) and hypotension (systolic blood pressure 90 mmHg). Nearly 20 hours after hospital admission, the patient developed hyperthermia (40.3°C) and experienced intense pain in the right hypochondrium and epigastrium, which did not respond to analgesia. Blood gas analysis revealed hyperlacticaemia (6.6 mmol/L, normal range < 2 mmol/L) without metabolic acidosis or respiratory insufficiency.
Fluid resuscitation was started and an abdominal CT scan was performed, revealing multiple abscesses, most prominent in the right lobe. In the left hepatic lobe, biliary cists where present, up to 3.5 cm, but not gaseous necrosis was found. Gas was additionally detected in the portal spaces, likely originating from the described necrotic lesions (Figure 1).
The patient was started on antibiotics, ceftriaxone and metronidazole, with prior blood cultures obtained for further analysis. He was admitted to ICU, where in the following 2 hours he progressed to multiple organ failure, with neurological dysfunction (lethargy), acute kidney injury (AKIN stage 3), severe metametabolic acidosis (pH< 7,10), hyperlacticaemia reaching 20 mmol/L, liver dysfunction and cardiovascular dysfunction characterized by refractory septic shock. Massive intravascular hemolysis also occurred, with a decrease in hemoglobin levels of 6 g/dL in less than 6 hours, increased bilirubin and macroscopic evidence of haemolysis in blood samples. There was no criteria for hemophagocytic syndrome nor intravascular disseminated coagulation. Table 1 depicts the evolution of haematological and biochemical parameters.
Despite all the efforts, the patient did not respond to supportive treatments and remained unstable, precluding surgical intervention. Although a cardiac arrest was initially reversed, subsequent cardiac arrest reoccurred, ultimately resulting in the patient’s demise less than 30 hours after admission to the hospital.
Blood cultures yielded positive results within 24 hours, with Clostridium perfringens identified in one anaerobic sample, and Haemophilus parainfluenzae detected in three sample. These a posteriori data allowed classification as polymicrobial pyogenic liver abscess, with clinical evolution presenting a typical toxin producing Clostridium species bacteriemia.
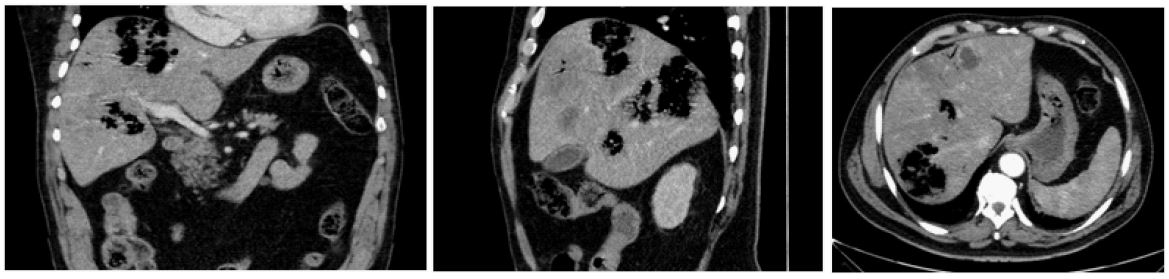
Table 1: Haematological and biochemical results of blood samples withdrawn on admission, after the first fever episode (22 h), at initiation of attempts to stabilize within Intensive Care Unit (25 h) and shortly before death (28 h). * Hemolysis precluded values determination, and values of lactate dehydrogenase and triglycerides were never able to be determined.
| Admission (T0) | T0 + 22h | T0 + 25h | T0 + 28h | |
|---|---|---|---|---|
| Hemoglobin (N 13-18g/dl) | 13.3 | 12.2 | 8.6 | 6.3 |
| Leukocytes (N 3.8-10.6x103 /uL) | 9.32 | 20.000 | 28.910 | 25.570 |
| Platelets (N 150-440x103 /uL) | 259 | 265 | 68 | 20 |
| apTT (N 25-35seg) | - | - | 76.6 | 122.8 |
| INR | - | - | 1,75 | 2,35 |
| Fibrinogen (N 200-400 mg/dl) | - | - | 389 | 225 |
| Creatinine (N 0.67-1.17 mg/dl) | 1.12 | 1.4 | - | Hemolysis* |
| Total bilirubin (0.1-1 mg/dl) | 1.93 | 11.42 | - | 9.5 |
| ALT (N 4-50U/L) | 842 | 1079 | - | Hemolysis* |
| AST (N 4-50U/L) | Hemolysis* | Hemolysis* | - | Hemolysis* |
| Alkaline phosphatase (N 40-129 U/L) | 151 | 235 | - | - |
| Reactive C protein (N<0.5mg/dl) | 0.3 | 15.4 | - | - |
| Lypase (N 13-60 U/L) | 206 | 25 | - | - |
| Lactate levels (mmol/L) | - | 6,6 | 19 | 20 |
| Arterial pH | - | 7,45 | 7,06 | 6,88 |
Table 2: Case reports of pyogenic liver abscesses with microbiological documentation of clostridium perfringens, since 2000, with special focus on occurrence of significant intravascular hemolysis and therapeutic strategies, numbered with corresponding references. F: Female, M: Male, NA: Data not available. Liver procedure includes procedures as thermal ablation (microwave or radiofrequencies), and all pancreatic surgeries consisted of cephalic duodenopancreatectomies.
| Author | Year | Sex | Age | Risk factor | Hemolysis | Source control | Death | Time to death (h) |
|---|---|---|---|---|---|---|---|---|
| Eckel F | 2000 | F | 65 | Liver procedure | NA | Yes (drainage) | No | - |
| Kreidl KO | 2002 | M | 80 | Diabetes | Yes | No | Yes | NA |
| Pichon N | 2003 | F | 42 | Liver cyrrhosis | No | No | No | - |
| Quigley M | 2003 | M | 73 | Neoplasm | NA | No | Yes | NA |
| Au WY | 2005 | M | 65 | Diabetes | Yes | No | Yes | 72 |
| Fondran J | 2005 | M | 63 | Neoplasm | NA | Yes (Surgery) | No | - |
| Daly JJ | 2006 | M | 80 | Diabetes, liver procedure | Yes | No | Yes | 3 |
| Ohtani S | 2006 | M | 78 | Diabetes | NA | No | Yes | 3 |
| Loran MJ | 2006 | F | 69 | No | NA | No | Yes | 6 |
| Eigenberger B | 2006 | M | 60 | Transplant receptor | NA | No | Yes | 8 |
| Umgelter A | 2007 | F | 87 | Neoplasm | NA | Yes (drainage) | No | - |
| Tabarelli W | 2009 | F | 65 | Neoplasm, pancreatic surgery | No | Yes (drainage) | Yes | 120 |
| Del Agua IA | 2009 | M | 74 | No | NA | Yes (Surgery) | No | - |
| Merino A | 2009 | F | 83 | No | Yes | No | Yes | 72 |
| Meyns E | 2009 | M | 64 | Diabetes | Yes | Yes (drainage) | Yes | 52 |
| Macias I | 2009 | M | 72 | No | Yes | No | Yes | 22 |
| Ng H | 2010 | F | 61 | Diabetes | Yes | Yes (Surgery) | No | - |
| Bradly DP | 2010 | M | 52 | Neoplasm | NA | No | Yes | 6 |
| Rajendran G | 2010 | M | 58 | No | Yes | Yes (Surgery) | No | - |
| Law ST | 2012 | F | 50 | Neoplasm | NA | Yes (drainage) | Yes | 168 |
| Qandeel H | 2012 | M | 59 | Diabetes | Yes | Yes (Surgery) | No | - |
| Oshima S | 2013 | M | 74 | Neoplasm | Yes | Yes (Surgery) | Yes | 72 |
| M | 70 | Liver procedure | No | Yes (Surgery) | No | - | ||
| Imai J | 2014 | M | 76 | No | Yes | Yes (drainage) | Yes | 6,5 |
| Eltawansy SA | 2014 | F | 81 | No | No | Yes (drainage) | Yes | NA |
| Kitterer D | 2014 | M | 71 | Transplant receptor | NA | Yes (Surgery) | Yes | 13 |
| Kurasawa M | 2014 | M | 65 | Diabetes | Yes | No | Yes | 6 |
| Kusumoto K | 2014 | M | 64 | No | Yes | Yes (drainage) | No | - |
| Rives C | 2015 | M | 63 | Neoplasm | NA | Yes (Surgery) | No | - |
| Li JH | 2015 | M | 71 | Neoplasm | Yes | No | No | - |
| Lim AG | 2015 | M | 58 | No | Yes | No | Yes | 7,5 |
| Vuolio S | 2016 | F | 76 | Diabetes | Yes | Yes (Surgery) | Yes | 34 |
| Carretero RG | 2016 | M | 65 | Diabetes | Yes | Yes (drainage) | No | - |
| Kyang LS | 2016 | M | 84 | Neoplasm, liver procedure | No | Yes (drainage) | No | - |
| Hashiba M | 2016 | M | 82 | Diabetes | Yes | No | Yes | 3 |
| Gelonch LM | 2017 | M | 63 | Pancreatic surgery | Yes | No | Yes | 3 |
| M | 66 | Pancreatic surgery | Yes | No | Yes | 6 | ||
| Shibazaki S | 2017 | F | 68 | Diabetes | Yes | no | Yes | 1 |
| Paasch C | 2017 | M | 64 | Diabetes | NA | Yes (Surgery) | No | - |
| Yoshikawa T | 2018 | M | 70 | Neoplasm, liver procedure | No | No | No | - |
| Hamada K | 2018 | M | 68 | Neoplasm | Yes | No | Yes | 10 |
| Sakaue M | 2019 | M | 76 | No | Yes | No | Yes | 2,5 |
| Uojima H | 2019 | M | 83 | Neoplasm, liver procedure | Yes | no | Yes | 6 |
| Amjad W | 2019 | M | 77 | Neutropenia | yes | No | Yes | 24 |
| Dahl S | 2020 | M | 68 | Neoplasm | Yes | Yes (drainage) | No | - |
| Fujikawa H | 2020 | F | 77 | Neoplasm, pancreatic surgery | No | No | Yes | 14 |
| Wang MH | 2021 | F | 63 | Neoplasm, liver procedure | No | Yes (drainage) | No | - |
| Satoh M | 2021 | F | 81 | Diabetes | No | Yes (drainage) | No | - |
| Wong A | 2022 | M | 80 | Diabetes | Yes | No | Yes | 8 |
| Takahashi G | 2022 | M | 70 | Neoplasm, pancreatic surgery | Yes | Yes (drainage) | No | - |
| Guo J | 2022 | M | 62 | Neoplasm, liver procedure | Yes | No | yes | 12 |
| Ósório C | 2023 | M | 74 | Gallblader surgery | Yes | Yes (Surgery) | Yes | 13 |
Table 3: Case reports of pyogenic liver abscesses with microbiological documentation of Haemophylus parainfluenza, numbered with corresponding references.
| Author | Year | Sex | Age | Risk factor | Hemolysis | Source control | Death | Time to death(h) |
|---|---|---|---|---|---|---|---|---|
| Chattopadhyay B | 1983 | M | 26 | No | No | No | No | - |
| Desir G | 1986 | F | 57 | Transplant receptor | No | Yes (drainage) | No | - |
| Friedl J | 1998 | F | 58 | Transplant receptor | No | No | No | - |
| Hwang J | 2002 | M | 44 | No | No | Yes (drainage) | No | - |
| Cavrič G | 2015 | F | 78 | No | No | Yes (drainage) | No | - |
| Athreya A | 2017 | F | 53 | No | No | No | No | - |
| Perez BG | 2017 | M | 64 | No | No | Yes (surgery) | No | - |
| Finiss M | 2022 | F | 56 | Neoplasm | No | No | No | - |
Discussion
Clostridium abscesses are associated with a significant mortality rate, surpassing 50% in cases involving bacteremia [17]. The mortality rate further escalates to 80-100% in instances characterized by massive intravascular hemolysis [5,17,18], with a rapid decline and progression towards death typically occurring within 12 hours, as reported in numerous reviews [17,18].
In contrast, Haemophilus parainfluenza as a commensal organism of the digestive tract has a low pathogenic potential, and is present in over 20% of the fecal samples analyzed. It is an uncommon agent of human infection, but it has been found to be associated with endocarditis, bacteremia, soft tissue infection, septic arthritis, meningitis and brain abscesses, osteomyelitis, upper respiratory tract infections and rarely, liver abscess [19].
To provide a comprehensive overview, a literature review was conducted utilizing articles indexed in PubMed. Specifically, studies were selected that reported clinical cases of liver abscesses with confirmed microbiological evidence of Clostridium perfringens infection and Haemophilus parainfluenza, separately, since 2000. The summarized cases are presented in Table 2 and Table 3, respectively.
Regarding epidemiological characteristics, Clostridium perfringens PLA reviewed articles indicate a mean age around 65 years, similar to the subset of Clostridium perfringens PLA cases presenting with hemolysis (61 to 66.5 years [17]), with a male predominance. These findings are consistent with our review and presented case, with a mean age of 69 years and 74,1% occurring in men. In our review of Haemophilus parainfluenza PLA reported cases, we found a mean age of 54 years, with a slight female predominance.
Liver abscesses are unilocular in approximately 70% of cases. Around 20% of cases present as microabscesses. The morphology and distribution of abscesses are often associated with their origin. Abscesses of biliary origin tend to be multilocular, while those originating from the portal system are more commonly located on the right side. In cases where the origin is arterial, abscesses may be more scattered in distribution.
The majority of pyogenic abscesses, including Clostridium abscesses, occur in patients with some degree of immunosuppression (diabetes mellitus, hemodialysis, hematologic diseases, solid organ transplantation), neoplasms (pancreas, stomach, hepatobiliary, rectum), or those who have undergone procedures (e.g., arterial chemoembolization) [17,18,20]. This pattern is consistent with our review, where only 18.5% of cases did not have identified risk factors. In our patient’s situation, no underlying immunodeficiency, recent intra-abdominal infections, invasive procedures, or trauma were identified in the preceding weeks. Furthermore, there were no imaging or laboratory findings suggestive of neoplasms. Nonetheless, it could be hypothesized that the intermittent epigastric pain and elevation of pancreatic and hepatic markers could indicate the presence of biliary microlithiasis with biliary colic, which could potentially predispose the patient to ascending/biliary infection. The presence of multiple abscesses and the identification of Haemophylus parainfluenza (commonly involved in ascendant infections) in our case could support this hypothesis, although there was no evidence of gallstones or biliary sludge during the acute event.
The analysis of the reported Clostridium perfringens PLA cases demonstrates a mortality rate of 61,1%, with an median time from diagnosis to death of 11 hours. Regarding Haemophilus parainfluenza PLA cases, no fatalities were observed, wich demonstrate the more benign course of disease, as long as timely treated.
Poly-microbial bacteremia is reported in 40-55% of cases of PLA, but we found a lower percentage in Clostridium perfringens and Haemophilus parainfluenza PLA, with only around 10% and 25% (respectively) of cases exhibiting polymicrobial infections [6,7].
Although two pathogenic bacteria were identified in blood cultures, the clinical course of our patient, marked by the rapid progression to multiorgan failure, severe metabolic acidosis, massive intravascular hemolysis, and clinical evolution, aligns with the descriptions of Clostridium perfringens PLA found in the literature. The patient’s ultrasound examination, conducted less than 24 hours before the CT scan, lacking any findings indicative of abscesses further suggests the rapid bacterial proliferation that characterizes Clostridium perfringens [20]. The intravascular hemolysis manifestations are likely associated with the production of specific toxins of Clostridium perfringens, namely phospholipase C and/or enterotoxin [8,13] and its occurrence is linked to higher mortality rates [7]. In our literature review, data to evaluate the occurrence of hemolysis was available in about three quarters of the articles, with a calculated prevalence of hemolysis in 75% of the patients. As expected, mortality rates were higher in these cases, showing a statistical association of death when hemolysys occurred (p-value 0,044 in Fisher’s Exact Test). Most of cases had Clostridium bacteriemia, with only 9% of cases identifying clostridium only in the abscess pus. The presence of bacteriemia had no significant correlation with mortality (p-value 0.353 in Fisher’s Exact Test).
From literature review, the only prognostic factors associated with survival in cases of Clostridium abscesses are source control interventions, including interventional radiology or surgery, with preference given to the former whenever feasible, particularly in cases with a small number of abscesses [17,18]. From the analysis of our review, considering also our patient, source control was attempted in 50% of patients (percutaneous drainage or surgery), and the mortality rate in this group was 33%. Among patients who did not undergo source control interventions, the mortality rate was as high as 88,9%. There was statistical association between survival and source control (p-value < 0.001 in Fisher’s Exact Test). Regarding Haemophilus parainfluenza PLA, no inference can be made as there were no fatalities reported.
In the present case, due to the rapid progression to multiorgan failure and the patient’s unstable condition, the surgical option was rejected after surgery and anesthesiology consultation. Additionally, considering the number and extent of the lesions, confluent, along with the high clinical risk and the lack of potential benefit, percutaneous drainage wasn’t performed. Lastly, there was no availability for hyperbaric oxygen therapy, as it would imply a hospital transfer, which wasn’t possible due to patient’s condition. As so, the patient died without achieving source control within less than 3 hours after admission to ICU unit.
Acknowledgments: I would like to thank my colleagues involved in the evaluation and clinical discussion of the case in the emergency department and intensive care, namely Dr Cesar Vidal, Dr Catarina Nunes and Dr Wilson Mata, physicians and surgeon at Unidade Local de Saude de Gaia/Espinho.
References
- G G Kaplan, D B Gregson, K B Laupland. Population-Based Study of the Epidemiology of and the Risk Factors for Pyogenic Liver Abscess, Clinical Gastroenterology and Hepatology. 2004. doi: 10.1053/S1542-3565(04)00459-8.
- M F Alkomos, E Estifan, G Melki, S Adib, W Baddoura. Epidemiological, Clinical, Microbiological, and Risk Factors of Pyogenic Liver Abscess: An 18-years Retrospective Single-Center Analysis, J Community Hosp Intern Med Perspect. 2021; 11(1): 42-45. doi: 10.1080/20009666.2020.1831745.
- H Akhondi, D E Sabih. Liver Abscess. Stat Pearls Publishing. 2023.
- S Ferreira, et al. Abcesso Hepático Piogénico-Casuística De 19 Anos, GE Port J Gastroenterol. 2007; 14.
- R Ono, et al. Successful treatment of hepatic gas gangrene by open drainage: A case report and review of the Japanese literature, Int J Surg Case Rep. 2018; 49: 121-125. doi: 10.1016/j.ijscr.2018.06.028.
- N J C Woittiez, et al. Toxinotype A Clostridium perfringens causing septicaemia with intravascular haemolysis: Two cases and review of the literature, International Journal of Infectious Diseases. 2022; 115: 224-228. doi: 10.1016/j.ijid.2021.12.331.
- T G Simon, J Bradley, A Jones, G Carino. Massive intravascular hemolysis from clostridium perfringens septicemia: A Review. 2014. SAGE Publications Inc. doi: 10.1177/0885066613498043.
- J Sakurai, M Nagahama, M Oda. Biochemistry of Bacterial Protein Toxins Clostridium perfringens Alpha-Toxin: Characterization and Mode of Action,” J Biochem. 2004; 136: 569-574. doi: 10.1093/jb/mvh.
- D L Stevens, K A Maier, J E Mitten, K L A Stevens, B M Maier, et al. Effect of Antibiotics on Toxin Production and Viability of Clostridium perfringens. 1987.
- F Eckel, C Lersch, W Huber, W Weiss, H Berger, et al. Case Report Multimicrobial Sepsis Including Clostridium perfringens after Chemoembolization of a Single Liver Metastasis from Common Bile Duct Cancer. 2000. www.karger.comwww.karger.com/journals/dig.
- G Rajendran, P Bothma, A Brodbeck. Intravascular haemolysis and septicaemia due to Clostridium perfringens liver abscess, Anaesth. 2010.
- T Hifumi, Y Koido, M Takahashi, A Yamamoto. Antitoxin treatment for liver abscess caused by Clostridium perfringens. 2013. doi: 10.3350/cmh.2013.19.1.97.
- A Suzaki, K Ohtani, S Komine-Aizawa, A Matsumoto, S Kamiya, et al. Pathogenic Characterization of Clostridium perfringens Strains Isolated From Patients With Massive Intravascular Hemolysis, Front Microbiol. 2021; 12. doi: 10.3389/fmicb.2021.713509.
- M C Finniss, L Ibrahim. Haemophilus parainfluenzae Pyogenic Liver Abscess Associated with Cholangiocarcinoma, Cureus. 2022. doi: 10.7759/cureus.22501.
- A Athreya, K Hrastar, F Khan. Haemophilus parainfluenzae as a rare cause of pyogenic liver abscess: A case report and literature review, Libyan Journal of Medical Sciences. 2017; 1(2): 49. doi:10.4103/ljms.ljms_18_17.
- E J Bottone, D Y Zhang. Haemophilus parainfluenzae Biliary Tract Infection: Rationale for an Ascending Route of Infection from the Gastrointestinal Tract, 1995. https://journals.asm.org/journal/jcm.
- A Suzaki, S Hayakawa. Clinical and Microbiological Features of Fulminant Haemolysis Caused by Clostridium perfringens Bacteraemia: Unknown Pathogenesis. 2023. doi: 10.3390/microorganisms11040824.
- C C Van Bunderen, M K Bomers, E Wesdorp, P Peerbooms, J Veenstra. Clostridium perfringens septicaemia with massive intravascular haemolysis: A case report and review of the literature, Neth J Med. 2010.
- J Friedl, et al. Haemophilus parainfluenzae Liver Abscess after Successful Liver Transplantation. 1998.
- R Roediger and M. Lisker-Melman, Pyogenic and Amebic Infections of the Liver. W.B. Saunders. 2020; 01. doi: 10.1016/j.gtc.2020.01.013.