
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 5
Seizure induced by tramadol injection in a female patient with epigastric pain
Muhammad Zohaib Rehman*; Muhammad Hamad Ali; Malik Shehryar; Arjun Singh
House Officer, Lady Reading Hospital, Peshawar, Pakistan.
*Corresponding Author : Muhammad Zohaib Rehman
House Officer, Lady Reading Hospital, Peshawar, Pakistan.
Email: muhammadzohaibrehman@gmail.com
Received : Sep 07, 2024
Accepted : Sep 25, 2024
Published : Oct 02, 2024
Archived : www.jcimcr.org
Copyright : © Zohaib Rehman M (2024).
Abstract
Tramadol is a weak mu (μ)-opioid receptor agonist with additional serotonin and norepinephrine reuptake inhibition properties. It undergoes extensive hepatic metabolism and is commonly used for managing moderate to moderately severe pain. However, tramadol can induce seizures, a side effect not always linked to overdose or preexisting seizure disorders. This case report describes a 35-year-old female who experienced generalized tonic-clonic seizures following a single intravenous dose of tramadol. Despite extensive diagnostic evaluations, no other cause for the seizures was identified. This report underscores the need for clinicians to be vigilant about tramadol’s potential to induce seizures, even at therapeutic doses, and highlights the importance of pharmacovigilance, especially in regions with limited monitoring capabilities.
Citation: Zohaib Rehman M, Hamad Ali M, Shehryar M, Singh A. Seizure induced by tramadol injection in a female patient with epigastric pain. J Clin Images Med Case Rep. 2024; 5(10): 3278.
Introduction
Tramadol is a weak mu (μ)-opioid receptor agonist that acts by inhibiting serotonin and norepinephrine reuptake [1]. Tramadol undergoes extensive hepatic metabolism by a number of pathways, including CYP2D6 and CYP3A4, and by conjugation with subsequent renal excretion. Tramadol is composed of a 1:1 racemic mixture of (+) -enantiomers and (-) +enantiomers.
(+) -Tramadol inhibits serotonin reuptake and (-) -tramadol inhibits norepinephrine reuptake. The major metabolite of (+) -tramadol activates the mu (μ) receptor [2]. The range of blood levels in adults is approximately 100 ng/mL to 300 ng/mL (0.1–0.2 μg/mL). The recommended dose of 400 mg/day is considered as the maximum approved dose [3]. Tramadol hydrochloride is a lipophilic substance that completely penetrates the barrier between the blood and the brain. The level of plasma besieges a peak around 1.5 h after taking, and 5 h to 6 h is the half-life of plasma exclusion. One of the complications of tramadol use is the seizure, which is most often generalized tonic–clonic [3]. Here, we are presenting a case report of a 35-year-old female patient, who had an episode of seizure following a single IV dose of tramadol. Which is a rare but significant side effect of tramadol.
Case presentation
Here is the rearranged case presentation in the specified order:
Patient’s description: An 18-year-old female presented to the emergency department at LRH Hospital, Peshawar, with chief complaints of progressive epigastric and flank pain persisting for the past 3 days. The pain was described as non-radiating and constant, accompanied by nausea but without vomiting.
Case history: Initial management included IV Toradol, Inj Risek 40mg, and Inj Nospa, which provided no relief. Subsequently, IV Tramadol was administered for pain management. Approximately 30 minutes post-Tramadol administration, the patient developed generalized tonic-clonic seizures. Immediate IV Valium was given to terminate the seizures. Post-ictally, the patient was confused, which resolved spontaneously within 30 minutes. She had no recollection of the seizure episode upon recovery.
Physical examination results: During examination, conducted in the presence of a nurse, the patient exhibited dull epigastric pain on deep palpation. The remainder of the physical examination was unremarkable.
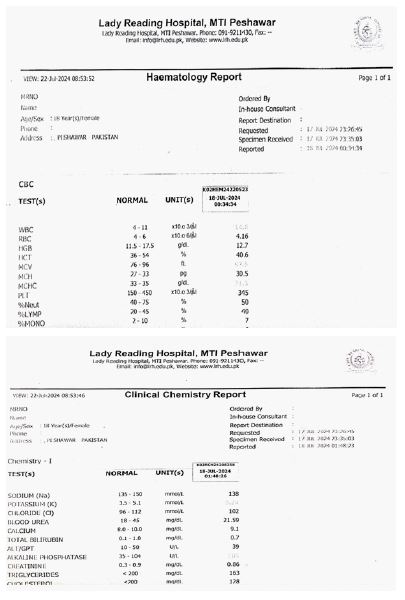
Results of pathological investigations: Blood tests including Complete Blood Count (CBC), Liver Function Tests (LFTs), Renal Function Tests (RFTs), serum electrolytes (Na, K, Cl), serum calcium, serum phosphorus, and lipid profile were all normal.
Imaging studies including ultrasound of Kidneys, Ureters, and Bladder (KUB), Electroencephalogram (EEG), and Computed Tomography (CT) of the brain also returned normal findings.
Treatment plan: The patient was discharged home following normalization of investigations and resolution of symptoms.
Discussion
Tramadol is a “bimodal” agent that possesses activity in both opioid and monoaminergic (serotonergic and noradrenergic) pathways in the Central Nervous System (CNS). Tramadol is commonly used in place of other potent opioid analgesics for the treatment of moderate to moderately severe pain associated with osteoarthritis, rheumatoid arthritis, low back pain, and neuropathic conditions [4,5]. There are controversies about the seizure-inducing effect of tramadol. Some earlier studies suggested that tramadol when given in overdose in patients with extant disorder of seizure or when used along with antidepressants, alcohol, etc., instigates seizure [6,7]. It was also disclosed from other studies that tramadol also instigates seizures when used as monotherapy in an approved dose. It has also been found that the appearance of seizures following tramadol use is not dose dependant [8]. However, in our patient, the seizure occurred at a dose of 37.5 mg oral tramadol hydrochloride. Tramadol-induced seizures have been reported to be generalized tonic–clonic in nature, without aura and focal deficit, as seen in our patient. Tramadol has very less abuse potential when compared to other opioids. So, it is prescribed very commonly in clinical practice. A recent cross-sectional study conducted by [9] in 2005 examined 106 patients with tramadol-induced seizures found that all the patients had tonic-clonic seizures within 12 h of oral intake of tramadol in supratherapeutic and recommended doses. Among those, 13% had a history of epilepsy, which was well controlled and did not recur before one year of their evaluation. Tramadol-induced seizures may be associated with agitation, tachycardia, confusion, and hypertension, leading to serotonin syndrome [10]. In the present case, the continuing tachycardia ranging from 120 to 140 bpm was found to be the only salient observation that could be accountable for low serotonergic action.
Conclusion
This case highlights the importance of considering tramadol as a potential cause of seizures, even in patients without a history of seizure disorders. Clinicians should exercise caution when prescribing tramadol, particularly in patients with risk factors for seizures or those receiving high doses. Prompt recognition and management of tramadol-induced seizures are crucial to minimize morbidity.
Tramadol has been otherwise a safe drug for many years; however, with evidence of serious reactions, like seizures even at low doses, the scientific community should consider pharmacovigilance with respect to its use, especially in developing countries where such monitoring systems are inadequate.
References
- Sansone RA, Sansone LA. Tramadol: Seizures, serotonin syndrome, and coadministered antidepressants. Psychiatry (Edgmont). 2009; 6(4): 17.
- Raffa RB, Friderichs EL, Reimann WO, Shank RP, Codd EE, et al. Complementary and synergistic antinociceptive interaction between the enantiomers of tramadol. Journal of Pharmacology and Experimental Therapeutics. 1993; 267(1): 331-40.
- Boostani R, Derakhshan S. Tramadol induced seizure: A 3-year study. Caspian journal of internal medicine. 2012; 3(3): 484.
- Duehmke RM, Derry S, Wiffen PJ, Bell RF, Aldington D, et al. Tramadol for neuropathic pain in adults. Cochrane Database of Systematic Reviews. 2017; 6.
- Cepeda MS, Camargo F, Zea C, Valencia L. Tramadol for osteoarthritis: A systematic review and metaanalysis. The Journal of rheumatology. 2007; 34(3): 543-55.
- Marquardt KA, Alsop JA, Albertson TE. Tramadol exposures reported to statewide poison control system. Annals of Pharmacotherapy. 2005; 39(6): 1039-44.
- Farajidana H, Hassanian-Moghaddam H, Zamani N, Sanaei-Zadeh H. Tramadol-induced seizures and trauma. Eur Rev Med Pharmacol Sci. 2012; 16(Suppl 1): 34-7.
- Talaie H, Panahandeh R, Fayaznouri MR, Asadi Z, Abdollahi M. Dose-independent occurrence of seizure with tramadol. Journal of medical toxicology. 2009; 5: 63-7.
- Labate A, Newton MR, Vernon GM, Berkovic SF. Tramadol and new‐onset seizures. Medical Journal of Australia. 2005; 182(1): 42-3.
- Beakley BD, Kaye AM, Kaye AD. Tramadol, pharmacology, side effects, and serotonin syndrome: A review. Pain physician. 2015; 18(4): 395.