
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 5
“Release and Revive”! Optimizing pediatric tongue tie care with oromyofunctional therapy: A case series
Srushti Akulwar1*; Ayisha Beevi TP1; Rajeev Kumar Singh2; Abhilasha Agarwal3; Anjali Anand1
1Junior Resident, Department of Paediatric and Preventive Dentistry, Faculty of Dental Sciences, King George’s Medical University, UP, Lucknow, India.
2Professor and Head, Department of Paediatric and Preventive Dentistry, Faculty of Dental Sciences, King George’s Medical University, UP, Lucknow, India.
3Senior Resident, Department of Paediatric and Preventive Dentistry, Faculty of Dental Sciences, King George’s Medical University, UP, Lucknow, India.
*Corresponding Author : Srushti Akulwar
Junior Resident, Department of Paediatric and Preventive Dentistry, Faculty of Dental Sciences, King George’s Medical University, UP, Lucknow, India.
Email: akulwarsrushti@gmail.com
Received : Sep 02, 2024
Accepted : Sep 26, 2024
Published : Oct 03, 2024
Archived : www.jcimcr.org
Copyright : © Akulwar S (2024).
Abstract
Ankyloglossia, commonly known as tongue-tie, whether partial or complete, can cause significant issues such as speech abnormalities, malocclusion, and swallowing difficulties, impacting daily routine activities. Various techniques, including scalpel, laser, electro-surgery. This novel research has shown that the atmospheric plasma is a minimally invasive method, successfully used for frenectomy, without important or fibrotic complications and with very low recurrence rates have been employed over the past few decades to treat tongue-tie. Every approach aims to improve tongue mobility by releasing tight muscle attachment, yet each has benefits and drawbacks. Oromyofunctional therapy (OMFT) used after treatment can significantly enhance oral health and tongue function substantially. This series presents three cases of partial ankyloglossia, each exhibiting speech difficulties and restricted tongue movements, necessitating definitive treatment to correct the deformity. The main objective of releasing the tongue tie was accomplished in all the cases, as the results demonstrated adequate healing and increased tongue mobility above pre-operative circumstances. Post-operative OMFT was implemented to further improve tongue movements and function substantially. The clinical outcomes following surgical tongue-tie release in the cases demonstrated better healing and improved tongue movements. This suggests that surgical treatment complemented by OMFT, is a reliable technique for treating ankyloglossia. Post-operative OMFT is crucial in enhancing the results by improving muscle strength and coordination, leading to optimal tongue function and overall oral health.
Keywords: Ankyloglossia; Frenectomy; Frenotomy; Speech Disorder; Tongue-Tie.
Citation: Akulwar S, Beevi A, Kumar Singh R, Agarwal A, Anand A. “Release and Revive”! Optimizing pediatric tongue tie care with oromyofunctional therapy: A case series. J Clin Images Med Case Rep. 2024; 5(10): 3280.
Introduction
Ankyloglossia, commonly known as tongue-tie, has been described as restricted tongue mobility due to a tight lingual frenulum. However, other overlooked factors such as airway obstruction, lack of general practice in tongue movement, insufficient tongue space, and extraoral fascial restrictions can contribute to the impaired tongue [1]. According to Meissner’s study, 71% of young children with ankyloglossia had speech abnormalities related to restricted tongue mobility. The correlation between ankyloglossia and speech disorders, however, remains controversial.
Only 23% of pediatricians have identified this association [2]. Treatment of choice for ankyloglossia includes various surgical techniques like frenectomy, frenuloplasty, and frenotomy. In recent years, the oromyofunctional therapy (OMFT) has emerged as a complement to surgical intervention. OMFT along with surgical intervention has given better results compared to surgery alone [1,3].
Though there is substantial literature on the various treatment modalities for tongue tie, there is a lack of evidence regarding the management of tongue tie using both surgery and OMFT. Therefore, we present this case series reporting treatment that combines excision and OMFT.
Case presentations
Case 1
A pre-schooler male patient reported to the Department of Paediatric and Preventive Dentistry, with the chief complaint of restricted tongue mobility, leading to speech difficulty in pronouncing certain words. On intraoral examination, the tongue exhibited limited movements due to high frenal attachment to the floor of the mouth, leading to inability to protrude and perform lateral movements of tongue. Characteristic V shaped notch was seen at the tip of the tongue showing heart shaped tongue on protrusion. It was diagnosed as Kotlow’s Class III ankyloglossia4 and grade 4 according to tongue range of motion ratio (TRMR) [1] (Figure 1).
Case 2
A school going boy reported to the Department of Paediatric and Preventive Dentistry, with the chief complaint of speech difficulties. On intra-oral examination, the tongue exhibited limited movements due to high frenal attachment to the floor of the mouth. Kotlows free tongue measurement was 16mm, suggestive of class I classification. Even though it was mild ankyloglossia patient showed limited tongue movement, we assessed anterior and posterior tongue mobility, it was diagnosed as grade 4 TRMR (Figure 2).
Case 3
A schooler reported to Department of Paediatric and Preventive Dentistry, with the chief complaint of speech difficulties. On intra-oral examination we confirmed that low tongue posture was the possible reason for maxillary hypoplasia. Additionally, an anterior crossbite was noticed on examination. Patient was diagnosed with class 2 Kotlow’s and grade 2 TRMR (Figure 3).
Treatment
After obtaining informed consent, preoperative OMT5 (Table 1) in 3 cycles/day with each exercise repeated 10 times was introduced through self-structured animated videos, a month before the surgical procedure for all the patients. A self-structured video consists of 8 exercises, in which different animated animal characters are shown after each exercise. Animals did a similar activity for each exercise to make it more interesting and encouraging for the patients. Also, the video of the same exercise performed by the patients was shown.
In the first case, under local anesthesia (2% Lidocaine with 1:200000 adrenaline), a bilateral lingual infiltration was given, with the tongue sutured at its tip using 3-0 silk suture material to hold or retract the tongue conveniently. The tongue tie was released using electrocautery.
In the second case, under local anaesthesia, bilateral lingual nerve block was given, tongue was sutured at its tip for retraction during surgery. Frenum excision was done using scalpel. Suture was placed.
In the third case, under local anaesthesia, bilateral lingual nerve block was given, with the tongue sutured at its tip for retraction. The tongue tie was released using electrocautery. Post-operative instructions were given in all the cases following surgery.
After 1 week following surgery, suture removal was done in the case were frenectomy was performed using scalpel. Postoperative OMT began immediately after surgery and was continued for 3 months for all the cases.
Outcome and follow-up
The patient was periodically followed up till 3 months. After three months, all patients showed excellent healing, improved tongue movements, speech, mastication, and crossbite correction in the third case.
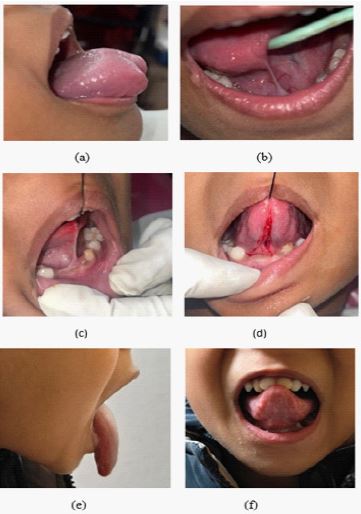
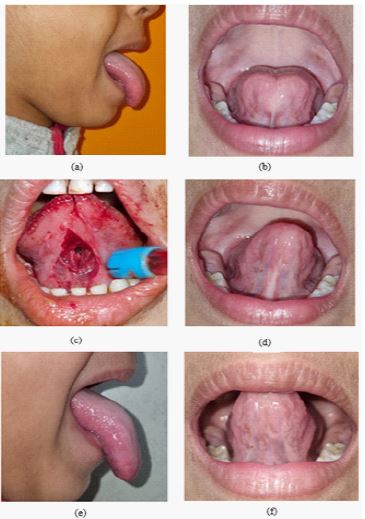
Table 1: Pre and Post Oral Myofunctional Therapy (OMT) [5].
| Exercise 1 | Licking bear | In this patient was asked to close his mouth place the tongue between lip and teeth and move it in a circular motion. |
| Exercise 2 | Open and close as tiger | Patient was asked to touch the spot with the tip of his tongue and then open and close the mouth. |
| Exercise 3 | Jump as high as fish | Patient touch the spot with his tongue tip then close his mouth and hold the position for 10 secs. |
| Exercise 4 | Tickling tortoise | In this exercise patient placed the tongue on the spot then roll his tongue backwards and forward onto the spot. |
| Exercise 5 | Open your mouth as wide as crocodile | Patient touched the spot with his tongue and then was asked to open his mouth as wide as he can. |
| Exercise 6 | Tongue out as dog | Patient was asked to stick out his tongue as long as he can. |
| Exercise 7 | Jumping Frog | Patient stretch out his tongue upward toward the nose and then downwards toward the chin likewise on the right and left cheek. |
| Exercise 8 | Teasing Monkey | In this exercise patient was asked to touch the palate behind the spot then suck the air slightly open his mouth hold it for 5 seus then detach the tongue from the palate making a chuck sound. |