
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Gastric outlet obstruction secondary to giant traumatic pancreatic pseudocyst
Muhammad Zakwan Bin Yahya1*; Kew Thean Yean2; Malinda Abd Majid3; Tan Tiong Keat4
1International Islamic University of Malaysia (IIUM), Malaysia.
2Hospital Censalor Tunku Mukhriz (HCTM), Malaysia.
3Hospital Kuala Lumpur (HKL), Malaysia.
4Hospital Sultan Abdul Halim, Sungai Petani, Malaysia.
*Corresponding Author : Zakwan Bin Yahya M
International Islamic University of Malaysia (IIUM), Malaysia.
Email: zakwanyahya@iium.edu.my
Received : Sep 13, 2024
Accepted : Oct 09, 2024
Published : Oct 16, 2024
Archived : www.jcimcr.org
Copyright : © Yahya MZB (2024).
Abstract
Traumatic pancreatic injury is rare due to its retroperitoneal location and relative protection to the organ. Pancreatic pseudocyst formation may occur following pancreatic trauma, but giant pseudocyst rarely develops. Early management is recommended for giant pancreatic pseudocysts before clinical deterioration. We presented a case report with gastric outlet obstruction symptoms in the casualty department. Imaging investigations Computed Tomography (CT) confirmed the presence of pancreatic transection with giant pseudocyst formation. He underwent endoscopic cystogastrostomy with immediate resolution of the symptoms. Imaging is essential for earlier detection and severity of the pancreatic injury and its complication like pancreatic pseudocyst formation. Imaging follows up are needed to monitor disease recurrence or suspected pancreatic duct injury and assess pancreatic ductal integrity before transluminal stent removal.
Keywords: Pancreatic pseudocyst; Gastric outlet obstruction; Pancreatic transection.
Citation: Yahya MZB, Yean KT, Majid MA, Keat TT. Gastric outlet obstruction secondary to giant traumatic pancreatic pseudocyst. J Clin Images Med Case Rep. 2024; 5(10): 3298.
Introduction
Pancreatic injuries are uncommon due to their retroperitoneal location, which protects the organ. It accounts for less than 2% of blunt abdominal trauma injuries [1]. It is associated with significant morbidity and mortality, with a mortality rate as high as 34% [2]. Common blunt traumatic pancreatic injury complications include traumatic pancreatitis, pseudocyst formation and fistula, and less commonly causing gastrointestinal bleeding and splenic vein thrombosis [1]. Traumatic transection resulting in complete pancreatic rupture commonly occurs in the line of the superior mesenteric vein at the neck of the gland [3]. The reported incidence of pancreatic pseudocyst following trauma varies and may reach 30% of pancreatic trauma cases [4]. Pancreatic pseudocysts are defined as fluid collection rich with pancreatic enzymes like amylase and surrounded by fibrous tissue wall rather than the true epithelial lining. The pseudocyst has direct or indirect communication with the ductal system, which is caused by pancreatic ductal disruption following inflammation, trauma or obstruction [5]. Giant pancreatic pseudocysts are rare, where the major diameter of the cyst measures 10 cm and above [6]. Local compression onto the duodenum can cause gastric outlet obstruction, where early satiety, nausea, vomiting and weight loss are manifestations of this complication [7].
We reported a 33-year-old male with a giant pancreatic pseudocyst following blunt abdominal trauma, which presented with gastric outlet obstruction symptoms as the initial presentation.
Case presentation
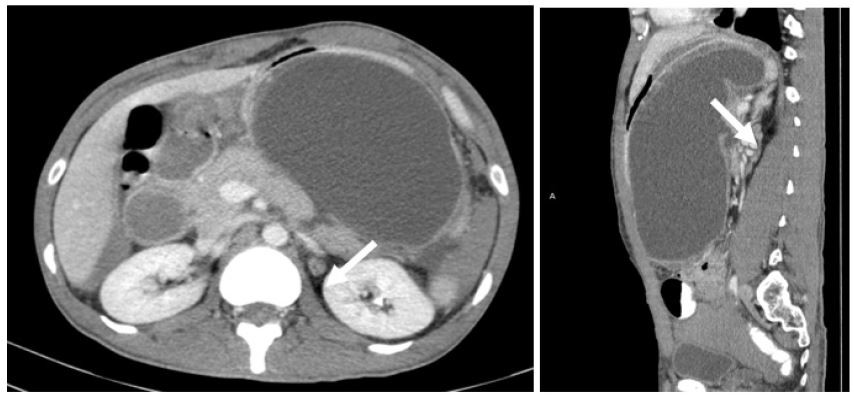
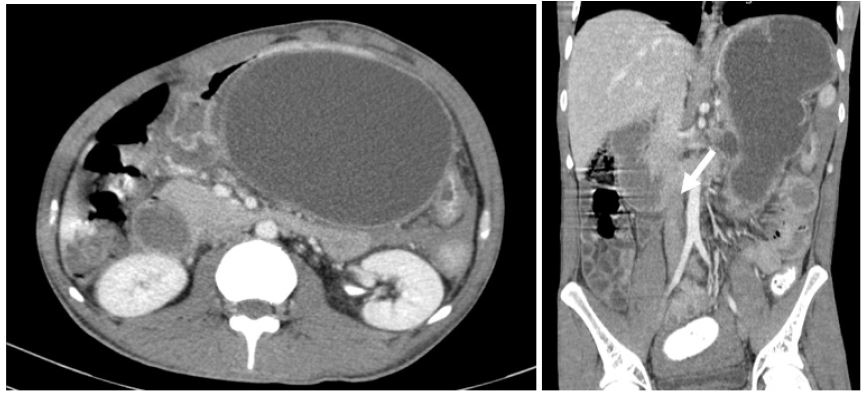
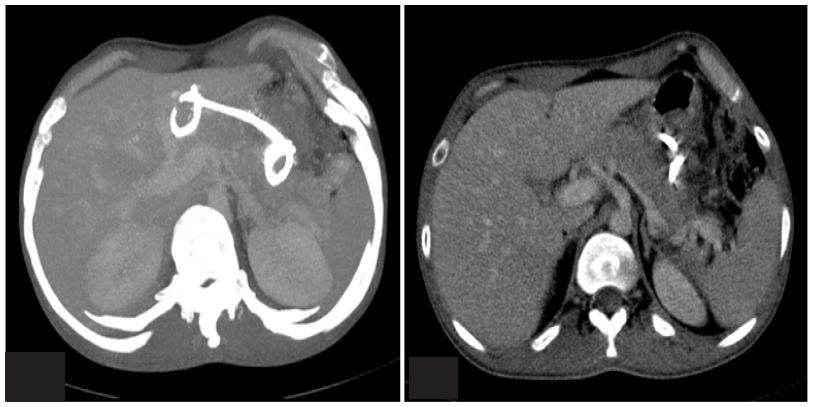
A 33-year-old male with underlying schizophrenia presented to a district hospital with a complaint of persistent vomiting for the past two weeks, three to four times a day, primarily fluid content. Associated with diarrhoea, abdominal pain, lethargy and unable to tolerate orally for two weeks. Clinical examination revelaed mass over left-sided abdomen extending to the right paraumbilical region, firm in consistency. Otherwise, the vital signs are all normal. Serum amylase was elevated 386 U/L (normal value: 40-140 U/L). Contrast-Enhanced Computed Tomography (CECT) abdomen and pelvis were performed and shows pancreatic transection with pseudocyst causing gastric outlet obstruction.
Table 1: American Association for the Surgery of Trauma – Organ Injury Scale (ASST - OIS) [1].
| Grade | Injury | Description of the pancreatic injury |
|---|---|---|
| I | Hematoma | Minor contusion without ductal injury |
| Laceration | Superficial laceration without ductal injury | |
| II | Hematoma | Major contusion without ductal injury or tissue loss |
| Laceration | Major laceration without ductal injury or tissue loss | |
| III | Laceration | Distal transection or pancreatic parenchymal injury with ductal injury |
| IV | Laceration | Proximal transection or pancreatic parenchymal injury involving the ampulla |
| V | Laceration | Massive disruption of the pancreatic head |