
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Intracranial solitary fibrous tumor: A rare case report and literature review
Shivani Malik1*; Arun Yadav2; Gaurav Dhakre3; Mayank Aggarwal3; Roopali1; Ashok Kumar Arya3
1Junior Resident, Radiation Oncology Department, Sarojini Naidu Medical College, Agra, Uttar Pradesh 282002, India.
2Assistant Professor, Radiation Oncology Department, S N, Medical College, Agra, India.
3Associate Professor, Neurosurgery Department, S N, Medical College, Agra, India.
*Corresponding Author : Shivani Malik
Junior Resident, Radiation Oncology Department, Sarojini Naidu Medical College, Agra, Uttar Pradesh 282002, India.
Tel: 917082151383;
Email: shivanimalik600@gmail.com
Received : Sep 18, 2024
Accepted : Oct 17, 2024
Published : Oct 24, 2024
Archived : www.jcimcr.org
Copyright : © Malik S (2024).
Abstract
Solitary Fibrous Tumors (SFT) are very rare, particularly those of the Central Nervous System (CNS), and they have mesenchymal origin. Here, we present the case of a 46-year-old man who, a year after suffering a head injury, lost consciousness for an hour. He had therapy after developing paralysis in his left arm and left foot after three months. A month and a half earlier, he had a bad headache, which triggered an examination. The right temporal frontal lesion on magnetic resonance imaging seems to be a sizable, well-defined extra-axial solid lesion with lobulated edges, predominantly isointense to the white matter with dispersed patches of hypointensity hole on T1WI. The lesion is isointense to the gray matter on T2WI, with sporadic hypointensities. Along the right anterior eminence with the bulk medially, thick, smooth dura mater is seen. A rise in the choline peak was seen in the MRI spectra. The right frontal lobe’s white matter showed a little hyperintensity but no signs of angioedema-related diffusion limitation. The pathological diagnostic of the tumor was a grade 3 solitary fibrous tumor after it was surgically excised during a right frontal craniotomy with nearly an entire resection. S100, CD34, STAT Positivity for 6, CK, and KI67 were found during an immunohistochemistry study, and it was done since SFT is challenging to differentially detect through imaging. The patient had extra adjuvant therapy in the form of whole-brain external beam radiation (54 Gy/30#@1.8Gy/#@5#/week) due to the tumor’s grade 3 status. Additional research and observation are needed for the prognosis.
Key clinical message: Central nervous system Solitary Fibrous Tumors (SFT) are rare, mesenchymal-origin tumors presenting challenges in diagnosis and management. This case highlights a grade 3 SFT causing focal neurological deficits, necessitating aggressive treatment with surgery and adjuvant radiotherapy for optimal management and prognosis assessment.
Keywords: Solitary fibrous tumor; Central nervous system; Magnetic resonance imaging; Immunohistochemistry; CD34; STAT 6.
Citation: Malik S, Yadav A, Dhakre G, Aggarwal M, Roopali, et al. Intracranial solitary fibrous tumor: A rare case report and literature review. J Clin Images Med Case Rep. 2024; 5(10): 3310.
Introduction
Solitary Fibrous Tumors (SFT) contribute up to less than 2% of all soft tissue masses. They are uncommon, collagen-rich, spindle cell tumors belonging to mesenchymal origin. It was initially described by Wagner in 1870. Pleural SFT was initially described by Klempere and Rabin in 1931 [1]. The pericardium, peritoneum, lung, liver, upper respiratory tract, mediastinum, thyroid, parotid gland, sinuses, orbits, and systemic circulation are among the pleural and extrapleural locations where instances have been described [1,7]. As there is no real connective tissue component in the CNS, extrapleural SFTs, particularly CNS SFTs, are uncommon. One percent of all primary CNS tumors are this kind [3]. Cerebellopontine angle, spinal dura mater, parasagittal region, meninges, and ventral tegmental area SFTs have all been documented [1]. The disease often affects individuals between the ages of 20 and 70, and both men and women have equal chances of contracting it [4]. SFTs must be distinguished from certain cancers, including fibrous meningiomas and hemangiopericytomas, as well as myxoid forms, including meningiomas, myxochordoid tumors, and myxoid peripheral nerve sheath tumors. Rare mesenchymal tumors called Hemangiopericytomas (HPC) have SFT’s clinical, radiological, and pathological characteristics [5].
NGFI-A binding protein (NAB2) and signal transducer and activator of transcription 6 (STAT6) gene fusions are driver mutations of SFT [1,6]. The World Health Organization (WHO) classified SFT and HPC as a new combined entity in 2016 [2,7] as a result of previous pathology results showing that these tumor types share the same genetic defects. Three levels of SFT/HPC, specifically levels I, II and III, are described by this classification. It should be underlined that while there is a clear clinical and histological overlap, the difference between the two is no longer clinically meaningful. The term “perivascular hemangioma” was eliminated from the 2021 WHO classification of CNS malignancies and replaced with SFT [8].
Reported herein is a 46-year-old male patient who had CNS Solitary Fibrous Tumor.
Case presentation
History: A 46-year-old male patient presented to the hospital 5.5 months ago with a severe headache for 2 days. He had a history of trauma to the right side of his head from 1 year ago, following which he had lost consciousness for 1 hour. Then he recovered spontaneously. Three months later, he suffered from hemiparesis of the left hand and left foot, for which he had been taking treatment for six months in the form of oral medications. He did not have any significant past illnesses or family history. Then the patient underwent surgery in the form of a right frontotemporal parietal craniotomy with near total excision of the space-occupying lesion, and the tissue was sent for histopathological examination, in which it came out to be a solitary fibrous tumor of grade 3. Just after surgery, the patient starts developing a bullous lesion on the bilateral foot at the Achilles tendon, which gradually increases in size and bursts after 3 days, following which the patient has had a chronic ulcer on b/l foot for 1 month .
Examination: Neurological examination was normal i.e. higher mental functions were intact, sensory and motor examination were also normal when the patient presented to the radiation oncology department.
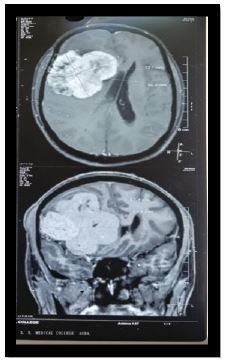
Investigations: The patient was investigated, and a brain MRI was performed. The contrast-enhanced MRI brain study suggested a large, well-defined extra-axial solid region with lobulated margins in the right fronto-temporal region, which appeared predominantly isointense to white matter with patchy areas of hypointensity on T1WI (Figure 1). On T2WI, the lesion is isointense to gray matter with patchy areas of hypointensity. Patchy areas of diffusion restriction noted on DWI correspond to a low value on ADC. In the post-contrast study, the lesion shows a tense homogenous enhancement. On MRS, an increase in choline peak is seen, and a few small cystic areas are also seen within the lesion. Smooth dural thickening is seen along the right frontal convexity. Medially, the lesion is causing a mass effect, as evidenced by the buckling of the right fronto-temporal lobes, effacement of the sulci of the right frontal and anterior temporal lobes, the ipsilateral sylvian cistern, the body, atria, and temporal horn of the right lateral ventricle, the third ventricle, the ipsilateral crural cistern, the ventral midline shift of 6.5 mm to the contralateral side, and subfalcine herniation. T2/FLAIR hyperintensity was noticed in the white matter of the right frontal lobe, showing no diffusion restriction suggestive of vasogenic edema. Features were suggestive of atypical meningioma.
On post-op NCCT head, an ill-defined hypodense area with blood attenuating density interspersed multiple extra-axial and intra-axial foci in the right lateral ventricle along with mild surrounding edema, resulting in a mass effect in the form of an effacement of nearby sulcal spaces and the right lateral ventricle. A contralateral midline shift of 13.6 mm was also seen. Subsequent adjuvant therapy in the form of whole-brain external beam radiotherapy (54Gy/30#@1.8Gy/#@5#/wk) was given to the patient.
On the Doppler of the bilateral lower limb, a few enlarged necrotic lymph nodes are seen in the left inguinal region, with the largest measuring approximately 2.5 x 2 cm in size. Arterial systems, venous systems, superficial venous systems, and perforators seem to be completely normal. The patient did not complain of inguinal lymph nodes. On USG-guided Fnac, it was cited that previous inguinal lymph nodes were likely reactive.
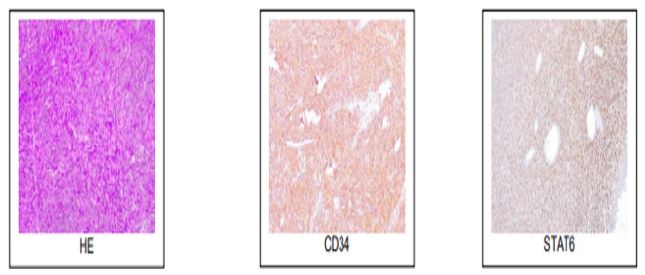
The right FTP mass excision biopsy specimen underwent immunohistochemistry analysis since SFT is challenging to properly identify using imaging. Lesional cells exhibited immunoreactivity for S100 with a score of 1+, CD34 with a score of 3+, and STAT 6 with a score of 3+ (Figure 2). In the cells of the lesions, there was immunoreactive patchy positivity for CK. In 6-7% of the lesional cells with INI-1 retention, KI67 was increased. SMA, DESMIN, EMA, SOX 10, or TLE-1 were not reactive.
Differential diagnosis: Atypical or Fibrous Meningioma, Hemangiopericytoma, Myxoid variants like myxochordoid meningioma and myxoid peripheral nerve sheath tumor.
Treatment: The patient had a right frontotemporal parietal craniotomy with near total excision of the space-occupying lesion followed by extra adjuvant therapy in the form of whole-brain external beam radiation (54 Gy/30#@1.8Gy/#@5#/week) due to the tumor’s grade 3 status.Time period between surgery and RT was 1.5 months.
Outcome and follow up: Patient is currently on follow up with us since 3 months. He is completely fine till date with no fresh complaints and completely normal physical and neurological examination. No lesion seen on MRI done 1 month post RT. As the patient is not affordable for angiogenesis therapy, he denied for that in written. His ulceration over feet has also healed up folloeing surgical intervention in form of debridement and local dressing.
Discussion
The parasagittal sinus and spinal canal are the most prevalent locations for the bulk of intracranial SFTs, which are dural masses made up mostly of very thick collagen bands that are produced by fibroblasts. This patient exhibited SFT coming from the right frontal lobe of the brain.
SFT symptoms can vary, and patients may have a variety of nonspecific symptoms linked to raised intracranial pressure or the tumor site. There can be hemiplegia, hearing loss, headaches, nausea, vomiting, disorientation, and memory issues [9].
An 86-year-old man with SFT, localized to the parietal lobe of the right side and infiltrating the parietal bone, was described by [10]. As presenting for 1 month with increasing and persistent motor impairment in the left lower extremities.
In another study, a 30-year-old man was diagnosed with SFT that was close to the temporal lobe of the right side and thickened the temporal bone next to it. The patient also exhibited dysarthria and left facial nerve palsy, as well as lessened muscle power in his left upper and lower limbs [1,3]. This patient experienced hemiparesis of the left arm and left foot in addition to a significant headache, and the SFT was found to be in the right frontal region. The main cause of headaches and vertigo is elevated intracranial pressure. Patients in this trial did not exhibit dysarthria, impaired vision, or symptoms of paralysis of the facial nerve.
For SFT diagnosis, MRI and CT imaging are crucial. Due to MRI’s fluctuating signal intensity, differential diagnosis of SFT is challenging. It’s crucial to distinguish between lymphoma, metastases, neurofibromas, meningiomas, and schwannomas. Important imaging methods for diagnosing SFT include CT and MRI.
Intracranial SFTs imaging exhibits a variety of characteristics, and earlier images have shown that intracranial SFTs are most likely to develop in or around the venous sinuses, the base of the skull, the sagittal sinus, the falx cerebri, and the peritentorium cerebelli. Extraaxial tumors with lobulated or irregular shapes, some of which are oval or dumbbell-shaped, further identify intracranial SFTs [11]. When compared to gray matter, the SFT generally has isointensity to slight hyperintensity on T1WI and isointensity on T2WI. In cystic degeneration and necrosis, T1WI exhibits an isointense mixed signal and an isointense signal with modest hyperintensity [10]. Additionally, in situations of necrotic areas and cystic degeneration, T2WI exhibits slight hyperintensity or mixed signals of isointensity [10].
The tumor looked markedly increased after enhanced MRI, and those who had cystic degeneration had heterogeneous enhancement [12]. Peritumoral edema is often not harmful.
SFT and meningiomas have comparable imaging characteristics; SFT may be distinguished from meningiomas using MRS. In SFT, compared to meningiomas, the relative amounts of choline and myo-inositol are higher. In addition, [13] demonstrated that SFT/HPC could be distinguished from meningiomas using the normalized ratio of apparent diffusion coefficient and sensitive signal intensity in the tumor. The right fronto-temporal area of the brain experienced SFT in the currently reported instance, along with signal hyperintensity, dural thickening, and mass effect as previously documented with an elevated choline peak on MRI spectroscopy.
SFT is mostly diagnosed by pathological investigation. The tumor tissue had a high concentration of spindle or polygonal cells, as seen by histological staining. Typically, there are many blood vessels and collagen fibers that resemble antlers. Around blood vessels, tumor cells are organized in concentric rings and can either form depleted or rich areas [14]. IHC revealed that CD34, vimentin, and STAT6 were positive for SFT tissues. However, the prognosis of a patient is frequently predicted by the Ki-67 proliferation index. In the prognosis assessment of CNS SFT, it has been suggested by several studies that elevated Ki-67 levels (>5%) lead to adverse prognoses.
Currently, CD34 is thought to be the best marker for SFT. Positive staining has been observed in 95-100% of patients, yet this tumor can still exist without CD34. Most individuals with intracranial SFT have positive STAT6. Due to a rearrangement on chromosome 12q, STAT6 could be connected to the NAB2-STAT6 gene fusion. Therefore, it is advised that intracranial SFT be diagnosed by looking for the STAT6 or NAB2-STAT6 fusion gene [1]. On the long arm of chromosome 12, NAB2 and STAT6 are adjacent genes that are transcribed in opposing ways [9]. In SFT, an intrachromosomal inversion aligns the genes so that they are transcribed from the NAB2 promoter in the same direction [5], resulting in nuclear expression of STAT6 that can be seen by IHC [15].
IHC labeling was used to identify STAT6 expression in cerebral SFT tissue, and the NAB2-STAT6 fusion gene was successfully identified to be excellently specific and sensitive. Nuclear STAT6’s have 100% specificity and 96.6% sensitivity, making STAT6 IHC a highly sensitive and specific alternative for the NAB2-STAT6 fusion gene.
In the current work, lesional cells showed STAT6 expression. Clinical pathology and prognosis may be related to various NAB2-STAT6 fusion mutations. The patient profiled in this study’s SFT tissue was discovered to be STAT6, CD34, S100, and CK positive, with a KI 67 INDEX of 6-7%. After surgery, the patient’s tumor did not return.
A high incidence of extracranial and local metastases is a feature of SFT [15]. Previous research has shown that there is a risk of recurrence in people with long-term SFT, even ten years after the first resection. As a result, SFT patients need careful care and continuous observation. The prognosis and therapy of the tumor presented in this article need more research because it is an uncommon malignancy.
Retrospective research was conducted on patients who got SFT of the brain between January 2009 and June 2019 by [15]. According to their findings, the WHO classification was lowered, and patients who received complete resection along with adjuvant therapies such as Gamma Knife surgery had longer Progression-Free Survival (PFS). It should be emphasized that the prior study, which was previously stated, was done retrospectively, had a limited sample size, and that its conclusions were skewed due to selection bias. According to the findings of a multicenter study, postoperative radiotherapy, such as 2D conventional radiotherapy, 3D conformal radiotherapy, and intensity modulated radiotherapy, can increase the PFS of patients with SFT very significantly, regardless of the extent of surgery [15].
Malignant intracranial SFT cannot be treated with surgical excision or postoperative radiation. Tumor angiogenesis and proliferation are inhibited by Anlotinib, a new multitargeted tyrosine kinase inhibitor with anticancer and antiangiogenic action [1]. SFT may benefit from anti-angiogenesis as a possible therapy. Malignant intracranial SFT can be effectively treated with surgery, radiation, and anlotinib alone [6]. The current work only covers one instance; thus, more investigation and bigger RCTs are required to confirm its findings. Advanced renal carcinoma and a few subtypes of advanced sarcomas of soft tissue are both approved to be treated with Pazopanib, which is a strong inhibitor of tyrosine kinase [17]. It should be noted that patients with metastatic or unresectable SFT are successfully treated with pazopanib.
Conclusion
SFT is an uncommon tumor. As it is rare but very similar to other common brain tumors, SFT has a heavy chance of misdiagnosis after imaging. It should be noted that histopathological examination is essential to differentiate SFT from other diseases of the CNS. Furthermore, resection of the complete tumor is the preferred treatment modality for SFT. Postoperative adjuvant treatment indications have not yet been clarified. Because of the risk of recurrence, careful follow-up for the long term, including periodic imaging along with surveillance, is recommended.
Results
The results of the current study revealed that surgical resection is the best option for treating SFT and that postoperative radiation can considerably increase patient PFS. For aggressive, incurable, or metastatic SFT, molecule-targeting therapies like the tyrosine kinase inhibitors anlotinib and pazopanib are potential options. It should be emphasized that the current study did not look at how various radiotherapy procedures affected SFT. Currently, no accepted treatment standards exist for malignant intracranial SFT.
Declarations
Ethical approval: All procedures performed were according to the ethical standards of the institutional and/or national research committee and the 1964 Helsinki Declaration, along alongwith its later amendments or comparable ethical standards.
Patient consent for publication: Written Informed consent was obtained from the patient for publication of the present manuscript, including all data and accompanying images in accordance with the patient consent policy of journal.
Conflicts of interests: The authors declare that they have no conflicts of interest.
Funding information: None.
Acknowledgement: This manuscript is preprinted in authorea. DOI: 10.22541/au.169866078.87626155/v1
Preprinted on October 30, 2023. S.M. contributed to the concept, design, definition of intellectual content, literature search, data acquisition, data analysis, statistical analysis, manuscript preparation, and manuscript review. A.K.Y. was involved in concept, design, definition of intellectual content, data analysis, manuscript preparation, and manuscript editing. G.D., M.A., A.K.A., R. helped in the definition of intellectual content, and manuscript review.
References
- Klemperer P, Rabin CB. Primary neoplasms of the pleura a report of five cases Arch Pathol. 1931; 11: 385-412.
- Goodlad JR, Fletcher CD. Solitary fibrous tumors arising at unusual sites: Analysis of a series Histopathology. 1991; 19: 515-522.
- Lin Q, Zhu J, Zhang X. Solitary fibrous tumor of the central nervous system invading and penetrating the skull: a case report. 2023; 10. https://doi.org/10.3892/ol.2023.13667.
- Thway K, Ng W, Noujaim J, Jones RL, Fisher C. The current status of solitary fibrous tumors: diagnostic features, variants, and genetics. Int J Surg Pathol. 2016; 24: 281-292.
- Zeng L, Wang Y, Wang Y, Han L, Niu H, et al. Analyses of prognosis-related factors of intracranial solitary fibrous tumors and hemangiopericytomas help understand the relationship between the two sorts of tumors. J Neurooncol. 2017; 131: 153-161.
- Zhang DY, Su L, Wang YW. Malignant solitary fibrous tumor in the central nervous system treated with surgery, radiotherapy, and anlotinib: A case report. World J Clin Cases. 2022; 10: 631-642.
- Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, et al. The World Health Organization classification of tumors of the central nervous system: A summary. Acta Neuropathol. 2016; 131: 803-820.
- Wang XQ, Zhou Q, Li ST, Liao CL, Zhang H, et al. Solitary fibrous tumors of the central nervous system: clinical features and imaging findings in 22 patients. J Comput Assist Tomogr. 2013; 37: 658-665.
- Sugiyama H, Tsutsumi S, Hashizume A, Inaba T, Ishii H. Are bone erosion and peripheral feeding vessels hallmarks of intracranial solitary fibrous tumor/hemangiopericytoma? Radiol Case Rep. 2022; 17: 2702-2707.
- Peng Z, Wang Y, Wang Y, Li Q, Fang Y, et al. Hemangiopericytoma/solitary fibrous tumor of the cranial base: A case series and literature review. BMC Surg. 2022; 22: 289.
- Bai LC, Luo TY, Zhu H, Xu R. MRI features of intracranial anaplastic hemangiopericytoma. Oncol Lett. 2017; 13: 2945-2948.
- Chen T, Jiang B, Zheng Y, She D, Zhang H, et al. Differentiating intracranial solitary fibrous tumor/hemangiopericytoma from meningioma using diffusion-weighted imaging and susceptibility-weighted imaging. Neuroradiology. 2020; 62: 175-184.
- Sun LJ, Dong J, Gao F, Chen DM, Li K, Liu J, Zhang C, Tohti M, and Yang XP: Intracranial solitary fibrous tumor: Report of two cases. Medicine (Baltimore). 2019; 201(98): e15327.
- Lee JH, Jeon SH, Park CK, Park SH, Yoon HI, et al. The role of postoperative radiotherapy in intracranial solitary fibrous tumor/hemangiopericytoma: A multi-institutional retrospective study (KROG 18-11). Cancer Res Treat. 2022; 54: 65-74.
- Yu Y, Hu Y, Lv L, Chen C, Yin S, et al. Clinical outcomes in central nervous system solitary-fibrous tumor/hemangiopericytoma: A STROBE-compliant single-center analysis. World J Surg Oncol. 2022; 20: 149.
- Schutz FA, Choueiri TK, Sternberg CN. Pazopanib: Clinical Development of a Potent Anti-Angiogenic Drug Crit Rev Oncol Hematol. 2011; 77: 163-171.
- Martin-Broto J, Cruz J, Penel N, Le Cesne A, Hindi N, et al. Pazopanib for treatment of typical solitary fibrous tumors: A multicentre, single-arm, phase 2 trial Lancet Oncol. 2020; 21: 456-466.