
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 5
The impact of cumulative smoking volume and length of smoking cessation on brachial artery reactivity
Kim L Lavoie1,2*; Nicola J Paine3; Andre Arsenault2; Bernard Meloche NMT2; Catherine Laurin2; Jennifer Gordon4; Simon L Bacon2,5
1Department of Psychology, University of Quebec at Montreal (UQAM), CP 8888, Succursale Centre- Ville, Montréal, Québec, Canada.
2Montréal Behavioural Medicine Centre, CIUSSS-NIM, Montreal Sacred Heart Hospital, 5400 Boulevard Gouin Ouest, Montréal, Québec, Canada.
3Department of Sport, Exercise and Health Sciences, Loughborough University, Epinal Way, Loughborough LE11 3TU, UK.
4Department of Psychology, University of Regina, Regina, SK, Canada.
5Department of Health, Kinesiology and Applied Physiology, Concordia University, 7141 Sherbrooke Street West, Montréal, Québec, Canada.
*Corresponding Author : Kim L Lavoie
Department of Psychology, University of Quebec at Montreal (UQAM), CP 8888, Succursale Centre-Ville, Montréal, Québec, Canada.
Email: Lavoie.kim@uqam.ca
Received : Sep 02, 2024
Accepted : Oct 21, 2024
Published : Oct 28, 2024
Archived : www.jcimcr.org
Copyright : © Lavoie KL (2024).
Abstract
Background: Cigarette smoking has been shown to cause endothelial abnormalities. Though the endothelium has shown the ability to recover function after smoking cessation, it is unclear how the intensity of lifetime cigarette consumption and the length of smoking cessation influence this recovery.
Methods: A total of 294 patients referred for a myocardial perfusion stress test participated in the study. On the day of the exercise stress test, patients completed a sociodemographic and medical history questionnaire, including detailed information on smoking history. The following day, patients underwent a nuclear medicine-based forearm hyperaemic reactivity challenge that assessed brachial artery reactivity via the Rate of Uptake Ratio (RUR) between the hyperaemic and the non-hyperaemic arms.
Results: Current and previous smokers had worsened RUR than non-smokers (F=3.36, p=.036). There was a trend for greater RUR’s to be associated with years of smoking cessation (β=.0211±.0122, p=.086), but no relationship to smoking volume (β=-.0074±.0051, p=.151). In addition, there was a significant interaction between length of cessation and smoking volume (β=-.0016±.0007, p=.019), indicating that there was a reduced benefit associated with the length of smoking cessation in patients who had smoked the highest volumes.
Conclusion: The results of this study suggest that there may be a threshold of smoking volume after which smoking cessation has minimal benefit for brachial artery reactivity.
Keywords: Smoking; Smoking cessation; Smoking volume; Brachial artery reactivity; Endothelial function.
Citation: Lavoie KL, Paine NJ, Arsenault A, Meloche NMTB, Laurin C, et al. The impact of cumulative smoking volume and length of smoking cessation on brachial artery reactivity. J Clin Images Med Case Rep. 2024; 5(10): 3315.
Introduction
Annually, nearly 6 million deaths worldwide are attributable to tobacco use, with the number of deaths expected to rise to nearly 8 million by 2030. Cigarette smoking is the most important modifiable risk factor for Cardiovascular Disease (CVD) [1], accounting for 35% of all CVD deaths annually in the United States [5] and 22% of all-cause mortality in Canada [2-5]. One of the mechanisms by which cigarette smoking could be responsible for CVD is by damaging the endothelium [6]. The endothelium plays a critical role in the regulation of vascular tone, platelet aggregation, thrombus formation, and inflammation. Endothelial dysfunction is an early feature of atherogenesis [7-8] and a precursor of early vascular damage. Acute and chronic smoking has been shown to impair endothelial function and damage vascular endothelial cells [10], even in healthy individuals [8-13]. and those exposed to secondhand smoke [14]. In general, smoking cessation in patients with CVD has been shown to significantly reduce the risk of mortality and CVD events, such as Myocardial Infarction (MI) and stroke. However, there are inconsistencies in the amount of benefit reported from smoking cessation that range from ex-smokers having a comparable CVD mortality risk as never smokers [15], to having a minimal reduction in CVD mortality (even after 20 years of cessation) [16], to having no CVD risk reduction at all [15]. Like CVD risk, the endothelium has been shown to have the ability to recover function after smoking cessation [17]. However, previous studies to date have only demonstrated partial recovery in Endothelial Function (EF) and none have considered the influence of smoking volume (i.e., cumulative pack years) on this improvement [8-19]. As such, it is unclear how both the cumulative volume of cigarette consumption and the duration of smoking cessation affect endothelial recovery. The goal of the present study was to assess the relationships between smoking volume (i.e., smoking pack years), time since smoking cessation, and brachial artery reactivity (as a proxy of EF) in a cohort of patients with and without established CVD undergoing exercise stress testing. We hypothesized a negative relationship between smoking volume and brachial artery reactivity and a positive relationship between time since smoking cessation and brachial artery reactivity. In addition, we wanted to explore the interaction between smoking volume and length of smoking cessation on brachial artery reactivity.
Material and methods
Participants: The current study was a sub-analysis of the Mechanisms and Outcomes of Silent Myocardial Ischemia (MOSMI) study [20,21]. MOSMI is a longitudinal study evaluating risk factors for silent ischemia, as well as the effects of silent ischemia on cardiovascular outcomes. For the MOSMI study, 905 consecutive stable outpatients that were originally referred for Single Photon Emission Computed Tomography (SPECT) exercise stress tests between July 2005 and December 2006 in the Nuclear Medicine Service of the Montreal Heart Institute were recruited. Eligibility for the MOSMI study included undergoing a current SPECT exercise stress testing, over the age of 18 years, and English or French as a spoken language. Patients were excluded if they had a documented cardiac event (e.g., myocardial infarction) within the last 4 weeks, if they had a potentially confounding medical condition that was considered to be more severe than CVD (e.g., cancer, chronic obstructive pulmonary disease), or if they were pregnant or nursing. Of the patients recruited for the MOSMI study, a total of 295 randomly selected patients underwent forearm Hyperaemic Reactivity (FHR) testing (due to limited gamma camera availability). Patients were not tested if they had eaten within four hours prior to the FHR test. Participants who were included in this study did not differ by age, sex, or medical status compared to those excluded. The study was approved by the Human Ethics Committee of the Montreal Heart Institute and written informed consent was obtained from all participants.
Procedure: Details of the study procedure have been previously reported. On the day that patients presented for their exercise stress test [20,21], they were invited to participate in the MOSMI study [22]. Consenting patients underwent a socio-demographic and medical history interview, during which detailed information on smoking history was collected. As part of the SPECT protocol, patients returned the following day to obtain resting images. Prior to the rest test, participants completed the FHR test. They were asked to maintain their usual medication regimen, but were asked to refrain from taking beta-blockers prior to the exercise and rest SPECT studies [23]. Brachial artery reactivity was assessed using the forearm Hyperaemic Reactivity (FHR) technique, which has been described in detail previously. In brief, the assessment consists of a patient being seated with both arms over the top of a standard large field-of-view gamma camera with a low energy high-resolution collimator (Scintronix, London, UK) hands prone [20-23]. Thirty seconds following ischemic challenge (cuff inflation of 50 mmHg above systolic blood pressure for 5 minutes on the right arm) 0.42 mCi/kg of the radioactive tracer Tc-99m-tetrofosmin (Myoview, Amersham Health, Princeton, NJ) was injected into the patient’s arm using a small catheter placed in the bend of the left arm. For the following 10 minutes, dynamic image acquisitions were performed using 128 x 128 matrices at a sampling rate one frame per second. From this procedure, the ratio between the rate of blood flow into the right (the challenge arm) and left (the control arm) arms, the Relative Uptake Ratio (RUR), was calculated using custom-made software (Sygesa, Montreal, Canada). A higher RUR symbolizes a better response of the endothelial tissue to the hyperaemic response, indicating better brachial artery reactivity, with scores less than 3.55 indicative of CVD. This technique [23], which is similar to other reported techniques [24] has good reproducibility [25] and good inter- and intra-rater reliability. Though one of the co-authors (AA) has a patent for the software used to calculate RUR, he was not involved in data collection (this was done by a nuclear medicine technician) [26], nor was he involved in data analysis.
Cigarette smoking: Detailed information on smoking history was collected, including current smoking status (never smoker, past smoker, current smoker), the age of starting and stopping, lifetime consumption (calculated in pack-years, which represents the multiplication of the average number of packs smoked per day [@20 cigarettes/pack] by the number of years smoked [27], and for current smokers, average number of cigarettes smoked per day. Never-smokers were those who reported to have never smoked in their life, and past-smokers were those who were reported to have smoked in the past, but were abstinent for at least six months prior to study entry. Current smokers corresponded to those who reported being active smokers (smoking at least 1 cigarette per day) as per Health Canada definitions [28].
Statistical analysis: A general linear model was used to assess the relationship between length of smoking cessation (independent variable), pack-years (independent variable), and RUR (dependent variable). All analyses included age, sex, diabetes, hypertension, hyperlipidemia, history of cvd, and prescriptions for ACE-inhibitors and statins as a-priori defined covariates based on previously demonstrated associations with the primary variables of interest [29,30]. Analyses were conducted using continuous variables; however, to aid interpretation figures are presented using data split into quartiles. Analyses were conducted using SAS v9.3 (SAS Inc, NC) with significance set at p<.05.
Results
Participants: The mean RUR for the entire sample was 4.1 ± 1.7 and 145 patients (44%) had a RUR indicative of endothelial dysfunction (i.e., RUR<3.55). Sociodemographic [23], clinical, and medical status by smoking status are presented in (Table 1). In total, 225 (76%) participants were current or previous smokers and provided a value of smoking volume (pack-years) and time since smoking cessation. Current smokers were significantly younger (54 ± 9 years) and were more likely to live alone than previous or never-smokers. Previous smokers were also significantly more likely to have a history of coronary artery disease than current or never-smokers. On average, patients smoked for 25 years ± 12 (SD) years, ranging from 1 to 55 years of smoking and smoked 16 pack-years ± 20 (SD). In terms of smoking patterns, current smokers smoked significantly longer (35 ± 10 years) and consumed a higher number of pack-years (32 ± 19) compared to previous smokers (23 ± 11 and 23 ± 20 respectively). For previous smokers, the average amount of years since they had their last cigarette was 19 ± 11.
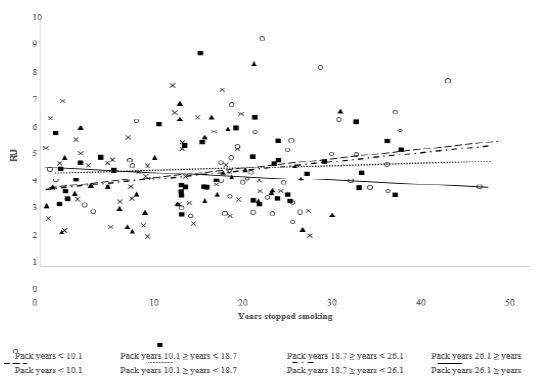
Brachial artery reactivity and smoking status, smoking volume, and length of cessation. As presented in (Figure 1), there was a main effect of smoking status on RUR (F=3.36, p=.036). Adjusting for covariates, participants who had never smoked had a significantly higher RUR (Mean ± SD = 4.47 ± 1.93) than those who were previous smokers (Mean ± SD = 3.85 ± 1.55) (p=.01). However, when current smokers were compared with the other two groups, no significant difference was detected (p=.39). In terms of intensity, smoking volume (i.e., the number of pack-years smoked) was negatively correlated with RUR (β=-.0099±.0050, F=3.95, p=.048). However, when adjusting for sex, age, history of CVD, hypertension, hyperlipidemia, and medications, this relationship was no longer statistically significant (β=-.0074±.0051, F=2.07, p=.151). With respect to length of cessation, there was a trend for greater RUR’s to be associated with years of smoking cessation (β=.0198±.011, F=3.25, p=.0733; adjusting for covariates: β=.0211±.0122, F=2.99, p=.086). Interaction between smoking volume and length of smoking cessation on brachial artery reactivity. There was a significant interaction between smoking volume (i.e., the number of pack-years) and years of smoking cessation (β=-.0016±.0007, F=5.65, p=.019), adjusting for covariates. As depicted in (Figure 2), for those that consumed a lower volume (i.e., fewer pack years) of cigarettes, RUR increased with number of years since quitting smoking. However, for higher volume (i.e., greater pack year) smokers, this relationship did not exist. These results indicate that in those patients who consumed a higher volume of cigarettes, there was no benefit of smoking cessation on brachial artery reactivity (RUR). The exact point at which smoking cessation appears to yield no benefit in patients who have smoked large volumes can be determined using the following equations relative to time (top equation) and volume (bottom):
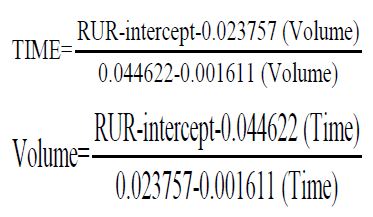
Table 1: Sample characteristics as a function of smoking status.
| Characteristics | Never smoked N=99(34%) |
Previous smokers N=165(56%) |
Current smokers N=30(10%) |
p |
|---|---|---|---|---|
| Age (years) | 59 ± 10 | 61 ± 9 | 54 ± 9 | <.001 |
| Sex (Women) | 35(35) | 30(18) | 10(33) | .007 |
| Ethnicity (Caucasian) | 96(97) | 96(97) | 96(97) | .877 |
| BMI (kg/m²) | 28 ± 4 | 28 ± 4 | 27 ± 6 | .805 |
| Cohabitating | 75(76) | 135(82) | 15(50) | <.001 |
| Education (>12 years) | 63(64) | 109(66) | 22(73) | .620 |
| Pack-years (average packs per day X years smoked) | 0 | 23 ± 20 | 32 ± 19 | <.0001 |
| Average number of years smoked | --- | 23 ± 11 | 35 ± 10 | <.0001 |
| Average years since stopped smoking | --- | 19 ± 11 | --- | --- |
| Average age of first cigarette | --- | 20 ± 7 | 19 ± 7 | .653 |
| History of CVD | 30(30) | 78(47) | 12(40) | .032 |
| Previous MI | 15(15) | 43(26) | 10(33) | .054 |
| Hyperlipidemia | 55(56) | 107(65) | 19(63) | .319 |
| Diabetes (either type 1 or 2) | 18(18) | 23(14) | 3(10) | .470 |
| Hypertension | 57(58) | 106(64) | 17(57) | .487 |
| Medication | ||||
| ACE-inhibitors | 24(24) | 45(27) | 7(23) | .873 |
| Beta-blocker | 24(24) | 51(31) | 10(33) | .440 |
| Statins | 40(40) | 91(55) | 15(50) | .084 |
Presented as either N (%) or Mean □ SD. Note: BMI = Body Mass Index; CAD = Cardiovascular Disease, MI = Myocardial Infarction.

Discussion
The goal of this MOSMI sub-study was to assess the relationships between smoking volume (pack-years), length of smoking cessation, and brachial artery reactivity in a cohort of cardiac outpatients undergoing exercise stress testing. To our knowledge, this is the first study to evaluate the interaction between the length of smoking cessation and smoking volume on brachial artery function, and the results show that as total smoking volume (pack-years) increased, less improvement in RUR was seen after having quit. Therefore, there was a reduced benefit associated with smoking cessation in patients who had smoked the highest volumes, suggesting that after reaching a certain threshold of cumulative smoking, cessation (regardless of the time since cessation) may have less benefit for endothelial recovery. Our study showed that smoking cessation led to an improvement in endothelial function, and that in patients who had the greatest length of smoking cessation (i.e., stopped smoking the earliest) also had the best endothelial function. This is consistent with other studies showing that smoking cessation leads to prolonged improvements in endothelial function. In terms of smoking volume, our study showed that patients who smoked the most (measured in cumulative pack-years) had worse brachial artery function [19-31]. However, this relationship was no longer statistically significant when adjusted for other covariates, which would indicate that smoking volume alone is not a key determinant of worsened vascular function. While this is consistent with other studies that have demonstrated that FMD is generally lower in smoker’s vs non-smokers, [32,33] there are consistencies within the literature that examines the role of smoking volume. Some have found a significant inverse relationship between endothelial impairment and number of pack-years smoked; [8] however, others have shown that non-smokers have better endothelial function compared to smokers. Overall [32], the literature supports our data which appears to indicate that lower smoking volume alone does not influence endothelial function, but that its interaction with length of smoking cessation is key to improving endothelial function. We also found, as noted by previous work, [8-13] that past smokers have worse brachial artery reactivity than those who have never smoked. However, unlike previous studies in healthy participants, [8-35] current smokers did not show a significant difference in their RUR from non-smokers or previous smokers. One speculative explanation for this finding is that there was an underestimation of the difference between current and previous smoker groups due to the self-reported nature of smoking data. As such, an unknown proportion of previous smokers may still smoke occasionally without mentioning it or they may be exposed to second hand smoke (not assessed), hence reducing the overall benefits of smoking cesstion. Alternatively, there may be another factor which is a stronger predictor of RUR than smoking that differs significantly between groups, for example, current smokers were younger than previous smokers. Although we adjusted for this variable, it highlights the possible influence of another mediating factor. Though the present study was not designed to assess the mechanisms by which quitting smoking or smoking volume impacts the endothelium, it is likely that this occurs through complex bio- physiological pathways. Studies have demonstrated that through the increase in free radical-derived oxidative stress, tobacco smoke leads to an impaired endothelium by damaging vascular endothelial cells36 and reducing the bioavailability of Nitric Oxide (NO), the main vasodilator of the endothelium [30-38]. Fortunately, this process has been shown to be reversible following smoking cessation. For example, studies have shown that the arteries can recover their ability to produce NO after cessation of passive smoking, [39] and that the coronary vasomotor abnormality can recover within one month of smoking cessation in young smokers [40]. However, this reversibility may only be partial, as previously shown [8]. Extending this theory, it is possible that the reversibility of the endothelial dysfunction or the recovery of the arteries’ ability to produce NO is abolished after a certain number of cigarettes are smoked, independent of smoking cessation. Although speculative, this irreversibility may coincide with the loss of vascular tone and the progression of atherogenesis [30].
Study limitations: It is important to note a few limitations of this study. First, this study was cross-sectional, therefore it is difficult to make causal inferences on whether smoking is the true cause of reduced brachial artery function or not. Another limitation is that the data on smoking status, intensity, and time of cessation was self-reported and not recorded by biological markers (e.g., cotinine or thiocyanate concentrations). However, we had a large sample, which should reduce the impact of any such biases. Finally, the fact that the study included mostly male patients who either had confirmed CVD or were under investigation for CVD, could limit the generalizability of the results. However, our sample demographics are consistent with those of patients referred for exercise stress testing.
Conclusion
This study showed that the length of smoking cessation was proportional and smoking volume inversely proportional to brachial artery reactivity. In addition, we found that brachial artery reactivity improved with the length of smoking cessation as a function of the amount smoked, thus suggesting that there appears to be a critical smoking volume, after which smoking-induced endothelial dysfunction cannot recover. This finding is of importance to health care professionals, as they should consider the limits of brachial artery function reversibility in treating patients who currently smoke or have previously smoked. Further studies are needed to better understand the impacts of smoking volume and cessation on endothelial health in order to develop optimal prevention and intervention strategies for CVD.
Abbreviations: BAR: Brachial artery reactivity; CVD: Cardiovascular disease; FHR: Forearm hyperaemic reactivity; MI: Myocardial infarction; MOSMI: Mechanisms and Outcomes of Silent Myocardial Ischemia; RUR: Relative uptake ratio; SPECT: Single photon emission computed tomography.
Declarations
Acknowledgements: The authors would like to thank Bernard Meloche (NMT) and Lynn Jolicoeur (NMT) for their invaluable assistance with data collection. We would also like to thanks all of our participants for volunteering their time to contribute to research.
Funding sources: Funding for data collection was provided by an operating grant from the Heart and Stroke Foundation of Quebec (HSFQ) and the Canadian Institutes of Health Research (MOP 79445 & 89965). Salary support was provided by the Fonds de la recherche en santé du Québec (FRSQ) (KLL & SLB), a CIHR Vanier PhD fellowship (JG), a GENESIS-Praxy CIHR post-doctoral fellowship (CL), and a CIHR/FRQS post-doctoral fellowship (NJP).
Conflict of interest statement: André Arsenault (now deceased since March 2022) owns the patent rights for the fhr procedure (non-invasive detection of endothelial dysfunction by blood flow measurement in opposed limb, Canadian Patent # CA 21413353; US Patent # 6445945 B1) and also owns 100% of SyGeSa Ltd who owns the rights for the proprietary software used in the calculation of RUR. No other author has any other conflicts of interest.
References
- Organization WH. WHO Reports on the Global Tobacco Epidemic. Geneva: World Health Organization. 2011.
- Anderson KM, Wilson PW, Odell PM, Kannel WD. An updated coronary risk profile: A statement for health professionals. Circulation. 1991; 83: 356-362.
- Yusuf S, Hawken S, Ôunpuu S, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-control study. Lancet. 2004; 364: 937-952.
- Ambrose JA, Barua RS. The pathophysiology of cigarette smoking and cardiovascular disease: An update. Journal of american college of cardiology. 2004; 43(10): 1731-1737.
- Services USDoHaH. The Health Consequences of Smoking-50 Years of Progress. A Report of the Surgeon General. Atlanta: US: Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health. 2014.
- Canada H. Canadian Tobacco Use Monitoring Survey. 2012.
- Quyyumi AA. Prognostic value of endothelial function. Am J Cardiol. 2003; 91(12-1): 19-24.
- Celermajer DS, Sorensen KE, Georgakopoulos D, et al. Cigarette smoking is associated with dose- related and potentially reversible impairment of endothelium-dependent dilation in healthy young adults. Circulation. 1993; 88(5): 2149-2155.
- Messner B, Bernhard D. Smoking and Cardiovascular Disease: Mechanisms of Endothelial Dysfunction and Early Atherogenesis. Arterioscler. Thromb. Vasc. Biol. 2014; 34(3): 509-515.
- Gimbrone MA, García-Cardeña G. Endothelial Cell Dysfunction and the Pathobiology of Atherosclerosis. Circ. 2016; 118(4): 620.
- Lekakis J, Papamichael C, Vemmos C, Stamatelopoulos K, Voutsas A, et al. Effects of Acute Cigarette Smoking on Endothelium-Dependent Arterial Dilatation in Normal Subjects. The American Journal of Cardiology. 1998; 81(10): 1225-1228.
- Papamichael CM, Aznaouridis KA, Stamatelopoulos KS, et al. Endothelial dysfunction and type of cigarette smoked: The impact of ‘light’ versus regular cigarette smoking. Vascular Medicine. 2004; 9(2): 103-105.
- Davis JW, Shelton L, Eigenberg DA, Hignite CE, Watanabe IS. Effects of tobacco and non-tobacco cigarette smoking on endothelium and platelets. Clin. Pharmacol. Ther. 1985; 37: 529-533.
- Otsuka R, Watanabe H, Hirata K, et al. Acute effects of passive smoking on the coronary circulation in healthy young adults. JAMA. 2001; 286(4): 436-441.
- Critchley JA, Capewell S. Mortality Risk Reduction Associated with Smoking Cessation in Patients with Coronary Heart Disease: A Systematic Review. JAMA. 2003; 290(1): 86-97.
- Gordon T, Kannel WD, McGee D, Dawber TR. Death and coronary attacks in men after giving up cigarette smoking: A report from the Framingham Study. Lancet. 1974; (2): 1345-1348.
- Cook DG, Shaper AG, Pocock SJ, Kussick SJ. Giving up smoking and the risk of heart attacks: a report from the British Regional Heart Study. Lancet. 1986; 2: 1376-1380.
- Raitakari OT, Adams MR, McCredie RJ, Griffiths KA, Celermajer DS. Arterial Endothelial Dysfunction Related to Passive Smoking Is Potentially Reversible in Healthy Young Adults. Ann. Intern. Med. 1999; 130(7): 578-581.
- Hosokawa S, Hiasa Y, Miyazaki S, et al. Effects of smoking cessation on coronary endothelial function in patients with recent myocardial infarction. Int. J. Cardiol. 2008; 128(1): 48-52.
- Mercer DA, Lavoie KL, Ditto B, et al. The interaction between anxiety and depressive symptoms on brachial artery reactivity in cardiac patients. Biol. Psychol. 2014; 102: 44-50.
- Pelletier R, Lavoie KL, Gordon J, Arsenault A, Campbell TS, et al. The Role of Mood Disorders in Exercise-Induced Cardiovascular Reactivity. Psychosom. Med. 2009; 71(3): 301-307.
- Anagnostopoulos C, Harbinson M, Kelion A, et al. Procedure guidelines for radionuclide myocardial perfusion imaging. Heart. 2004; 90: 1-10.
- Dupuis J, Arsenault A, Meloche B, Harel F, Staniloae C, et al. Quantitative hyperemic reactivity in opposed limbs during myocardial perfusion imaging: A new marker of coronary artery disease. J. Am. Coll. Cardiol. 2004; 44(7): 1473-1477.
- Karacalioglu AO, Demirkol S, Emer O, et al. Scintigraphic Imaging of Endothelium-Dependent Vasodilation in the Forearm. A Preliminary Report. Circulation. 2006; 70: 311-315.
- Meloche B, Arsenault A, Lavoie KL, Bacon SL. Test-retest reliability of a new method to measure endothelial function. Psychosom. Med. 2005; 67: 54.
- Veldhuijzen van Zanten J, Meloche B, Bacon SL, Stébenne PR, Arsenault A, et al. Inter-observer reliability of a new method to measure endothelial function. Psychosom. Med. 2006; 68: 36.
- Bernaards CM, Twisk JWR, Snel J, Van Mechelen W, Kemper HCG. Is calculating pack-years retrospectively a valid method to estimate life-time tobacco smoking? A comparison between prospectively calculated pack-years and retrospectively calculated pack-years. Addiction. 2001; 96(11): 1653-1661.
- Health Canada. 2015. http://www.hc-sc.gc.ca/hl-vs/tobac-tabac/research-recherche/stat/ctums-esutc_2006-eng.php.
- Celermajer DS. Endothelial Dysfunction: Does It Matter? Is It Reversible? J. Am. Coll. Cardiol. 1997; 30(2): 325-333.
- Puranik R, Celermajer DS. Smoking and endothelial function. Prog. Cardiovasc. Dis. 2003; 45(6): 443- 458.
- Johnson HM, Gossett LK, Piper ME, et al. Effects of smoking and smoking cessation on endothelial function: 1-year outcomes from a randomized clinical trial. J. Am. Coll. Cardiol. 2010; 55(18): 1988-1995.
- Amato M, Frigerio B, Castelnuovo S, et al. Effects of smoking regular or light cigarettes on brachial artery flow-mediated dilation. Atherosclerosis. 2013; 228(1): 153-160.
- Ozaki K, Hori T, Ishibashi T, Nishio M, Aizawa Y. Effects of chronic cigarette smoking on endothelial function in young men. J. Cardiol. 2010; 56(3): 307-313.
- Karatzi K, Papamichael C, Karatzis E, et al. Acute smoke-induced endothelial dysfunction is more prolonged in smokers than in non-smokers. International Journal of Cardiology. 2007; 120(3): 404-406.
- Esen AM, Barutcu I, Acar M, et al. Effect of Smoking on Endothelial Function and Wall Thickness of Brachial Artery. Circulation Journal. 2004; 68: 1123-1126.
- Hoshino S, Yoshida M, Inoue K, et al. Cigarette smoke extract induces endothelial cell injury via JNK pathway. Biochemical and Biophysical Research Communications. 2005; 329(1): 58-63.
- Napoli C, Ignarro LJ. Nitric oxide and atherosclerosis. Nitric Oxide. 2001; 5: 88-97.
- Barua RS, Ambrose JA, Eales-Reynolds L-J, DeVoe MC, Zervas JG, et al. Dysfunctional Endothelial Nitric Oxide Biosynthesis in Healthy Smokers with Impaired Endothelium-Dependent Vasodilatation. Circulation. 2001; 104(16): 1905-1910.
- Joannides R, Haefeli WE, Linder L, et al. Nitric Oxide Is Responsible for Flow-Dependent Dilatation of Human Peripheral Conduit Arteries in Vivo. Circulation. 1995; 91(5): 1314-1319.
- Morita K, Tsukamoto T, Naya M, et al. Smoking Cessation Normalizes Coronary Endothelial Vasomotor Response Assessed with 15O-Water and PET in Healthy Young Smokers. J. Nucl. Med. 2006; 47(12): 1914-1920.