
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Enigma of sudden onset seizures: Streptococcus pneumoniae and herpes simplex virus-1 central nervous system co-infection: A rare event
Arnab Choudhury1*; Satyendra Singh Rathore1; Khushdeep Shergill2; Balmik Shyamal3; Jithesh Gangadharan4; Sahil Kumar5
1Department of Medicine, Military Hospital, Mall Road, Ambala Cantt, Haryana, India.
2Department of Pathology, Military Hospital, Mall Road, Ambala Cantt, Haryana, India.
3Intern, Military Hospital, Ambala, India
4Department of Critical Care, Narayana Health, Bangalore, India.
5Department of Medicine, All India Institute of Medical Sciences, Rishikesh, Uttarkhand, India.
*Corresponding Author : Arnab Choudhury
Department of Medicine, Military Hospital, Mall Road, Ambala Cantt, Haryana 133001, India.
Tel: +91-8411041057; Email: arnab46@hotmail.com
Received : Oct 05, 2024
Accepted : Oct 28, 2024
Published : Nov 04, 2024
Archived : www.jcimcr.org
Copyright : © Choudhury A (2024).
Abstract
Herpes Simplex Virus-1 (HSV-1) encephalitis and Streptococcus pneumoniae meningitis co-infection is an exceptionally rare but clinically significant condition that raises distinct diagnostic and therapeutic issues. S. pneumoniae is the principal cause of bacterial meningitis, while HSV-1 is the most common cause of viral encephalitis in adults.Although they have different causes, co-infections can happen, commonly complicating the clinical situation and delaying diagnosis. This case report describes a patient who presented in the emergency department with two episodes of generalised tonic clonic seizures, and after further investigation, the patient was diagnosed with concurrent S. pneumoniae meningitis and HSV-1 encephalitis, the symptom overlap, diagnostic challenges and management. Another vivid feature was that for both infections there were no specific risk factors for the patient and complete recovery occurred with a combination of antibiotics and antiviral therapy focusing on the need for early identification and broad-spectrum empirical treatment of such co-infections. This case highlights the importance of additional research into the pathophysiological mechanisms of CNS co-infections and a high level of suspicion should be maintained when a patient is presenting with a febrile episode and seizures, despite it being a very unusual occurrence.
Keywords: HSV-1 Encephalitis; Streptococcus pneumonia meningitis; Co-infection; Generalised tonic-clonic seizures; Empirical therapy; CNS infections.
Citation: Choudhury A, Singh Rathore S, Shergill K, Shyamal B, Gangadharan J, et al. Enigma of sudden onset seizures: Streptococcus pneumoniae and herpes simplex virus-1 central nervous system co-Infection: A rare event. J Clin Images Med Case Rep. 2024; 5(11): 3325.
Introduction
Although they are rare, co-infections of the CNS (central nervous system) with bacterial along with viral pathogens provide significant challenges for diagnosis and treatment. The prominent reason for bacterial meningitis in developed countries is S. pneumoniae, particularly affecting vulnerable populations such as children, the elderly, and immunocompromised individuals. This disease is defined by inflammation of the meninges and can be fatal if not diagnosed and treated on time [1]. On the other hand, HSV-1 is the frequent cause of sporadic viral encephalitis, it mainly affects temporal lobes and results in significant neurological morbidity such as seizures and cognitive dysfunction [2].
Despite the fact that bacterial meningitis and viral encephalitis are usually viewed as separate clinical conditions, instances of co-infection are being reported with greater frequency, including cases of S. pneumoniae meningitis and HSV-1 encephalitis together. Co-infections may occur because of the breach of the BBB (blood-brain barrier) after bacterial infection, which allows viral invasion, or due to the reactivation of latent HSV-1 as a result of immune dysregulation caused by the bacterial infection [3]. In these cases, the clinical presentation may be more severe, and the risk of misdiagnosis is higher, leading to delays in appropriate treatment. This case report presents a patient who presented with fever and seizures leading to the diagnosis of concurrent S. pneumoniae and HSV-1 encephalitis, highlighting the challenges in diagnosing and managing this co-infection, with a focus on the need for early identification and the use of broad-spectrum empiric therapy
Case description
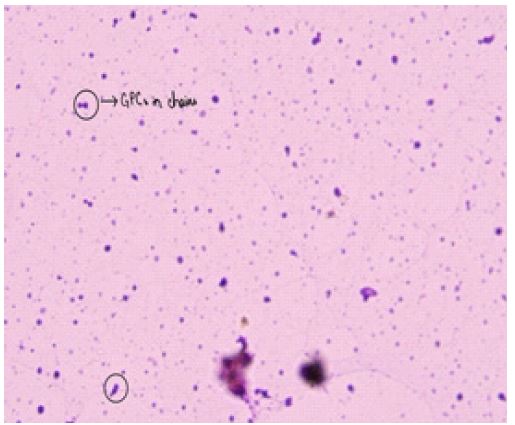
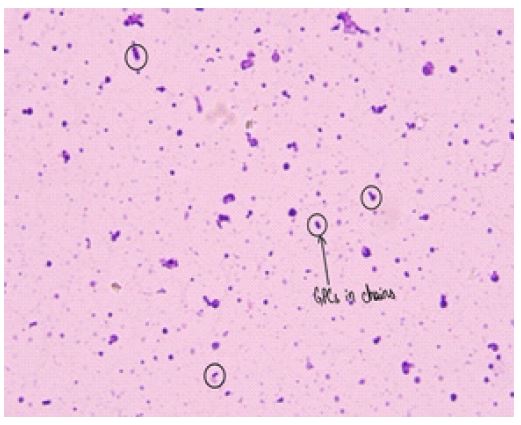
A 30-year-old young lady without any comorbidities came to the ED (Emergency Department) having a fever over the previous 8 days associated with a headache. While in the ED, she experienced two tonic-clonic seizures within ten minutes. The seizure were terminated with inj lorazepam and then she was administered a loading dose of inj Levetiracetam at a dose of 20 mg/kg bolus over 30 mins. She was then shifted to the Intensive care unit, where she was in a state of post ictal confusion. On evaluation, neurological examination revealed bilateral extensor plantars with neck rigidity and positive kernigs and brudzinski sign. She continued to have intermittent spikes of fever (maximum 102oF), with a blood pressure of 130/75 mmHg as well as a heart rate of 96 beats per min. The remainder of her physical examination was normal. However, she continued to remain drowsy with a GCS score of 9. A working diagnosis of acute meningoencephalitis was considered. Blood tests indicated leukocytosis (14×10⁹/l) with lymphocytosis (10.23×10⁹/l) along with raised C-reactive protein (26 mg/dl). Blood cultures were obtained as well and she was initiated on inj Ceftriaxone (2 g every 12 hrly), inj Vancomycin (1 g every 12 hrly) acyclovir (750 mg every 8 hourly) and inj Levetiracetam 1 g iv 2 hrly empirically. An urgent MRI Brain was performed on the same day which was normal. Cerebrospinal fluid (CSF) analysis revealed 820 cells/μl (80% lymphocytes), elevated protein (149 mg/dl), along with a glucose level of 70 mg/dl (the plasma blood glucose level was 168 mg/dl, while the blood glucose level was 101 mg/dl). The Gram stain of the CSF revealed gram-positive cocci (Figures 1 & 2).
Hence antibiotics were continued in view of pneumococcal meningitis. However, acyclovir was also continued in view of lymphocytic picture of CSF and normal CSF glucose report. Inj Dexamethasone 10 mg iv every 6 hours was also started in view of pneumococcal meningitis. On the third day, a Multiplex CSF biofirePCR (polymerase chain reaction) test returned positive results for HSV-1, & Streptococcus pneumonia confirming the diagnosis of CSF coinfection. However, the patient continued to be drowsy with pesistent febrile episodes (max 102oF). In view of fever and elevated CRP, ceftriaxone was stopped and antibiotic upgraded to inj Meropenem 2 g iv every 8 hourly (over 3 hour infusion). Blood cultures were negative. The patient responded well to the therapy, became afebrile after 2 days, with a marked reduction in her inflammatory markers and improvement in sensorium. An MRI Brain was repeated on day 5 of the illness which revealed nonspecific T2-hyperintense lesions in the right frontal and parietal lobe (Figure 3).

EEG could not be performed as it was not available at that point in time. The patient received 21 days of acyclovir as well as 14 days of meropenem treatment. Her neurological symptoms improved significantly, with full recovery. She was maintained on anticonvulsants, and no additional seizures were noted. She was discharged subsequently and advised regular followup to look for any neurological sequelae and gradual tapering off anticonvulsants. This case highlights the complexity of CNS infections and the importance of remaining vigilant when multiple pathogens may be at play. Timely swift adjustments in her treatment, this patient was able to make a full recovery from a potentially devastating condition.
Discussion
The co-infection of S. pneumoniae and HSV-1 in the CNS is exceedingly rare and can significantly complicate the clinical course. The patient presented the common signs of bacterial meningitis including neck stiffness, fever and an altered mental state. However, the fact that symptoms continued to be present and focal neurological signs appeared, such as seizures and memory impairment, led to suspicions of viral encephalitis. The diagnosis of herpes simplex encephalitis was also supported by MRI findings of temporal lobe involvement and later, CSF PCR was also positive for HSV-1 [4]. Several mechanisms could explain the development of this co-infection. Based on these facts one of the hypothesis is that because of inflammation and increased permeability of the BBB during bacterial meningitis viruses will be able to invade or reactivate [5]. The initial infection can also be a cause of immune suppression that leads to the reactivation of the HSV-1 virus. In addition, the high level of inflammatory response that is triggered by S. pneumoniae may increase the viral replication rate or inhibit the host’s capacity to contain the viral infection [6].
From a diagnostic approach, there is a lot of clinical overlap between bacterial meningitis and viral encephalitis. Both conditions may manifest with fever, headache, alteration of mental status and seizures, therefore, clinical differentiation between the two may be challenging [7]. In this case, the CSF study of the patient first provided characteristics suggestive of bacterial meningitis; the subsequent PCR test established the presence of HSV-1. Also this case was unique since initial MRI was normal and subsequent MRI Brain was suggestive of parietal and frontal T2W hyperintensities which is unusual in HSV [10]. Co-infection needs to be managed by a combination of antimicrobial and antiviral medications. The patient was started on antibiotics for S. pneumoniae, ceftriaxone, as well as empiric acyclovir for possible viral encephalitis. When co-infection was suspected, antibiotics were then given for 14 days and acyclovir for 21 days, which is typical for HSV-1 encephalitis. Steroid therapy was started because of streptococcus pneumonia with the advantage of decreasing cerebral oedema, intracranial pressure and prevent longterm neurological sequeale in severe bacterial meningitis [8]. Prognosis in CNS co-infections is variable, with outcomes largely dependent on the timing of diagnosis and initiation of treatment. In this case, the patient made a partial recovery with some residual cognitive deficits, a common long-term complication of HSV-1 encephalitis. This case highlights the importance of considering co-infections in patients with CNS symptoms that are not fully explained by a single pathogen, as early and aggressive treatment is key to reducing morbidity and mortality [9].
Conclusion
Streptococcus pneumoniae meningitis in combination with Herpes Simplex Virus-1 encephalitis is a rare but potentially fatal condition, and therefore, should be suspected and treated as soon as possible. Due to the similarity of clinical manifestations of these infections, it may take time before a definitive diagnosis is made, hence an increased level of suspicion and use of more sophisticated diagnostic techniques like CSF PCR and neuroimaging. When co-infection is considered, the initial empirical management for the patient should include both antibiotics and antiviral agents. Even though such co-infections have a worse prognosis, adequate and timely treatment will help to enhance the outcomes of the disease. This case highlights the current areas of deficiency in our understanding of the pathophysiology of CNS co-infections and the best management of these patients.
Highlights of the case
Both these processes together are rare with only a few case reports available in the world literature of HSV reactivation in CNS along with Pneumococcal infection of CNS.
The initial MRI Brain was normal which was rare and observed in only 10% of patients with HSV encephalitis [11].
Increased temporal activity in HSV encephalitis once more was not very commonly seen in MRI in our case. Few reported cases in worldwide literature.
No classical risk factors were present in this patient.
Declarations
Financial Support: Nil.
Conflict of Interest: None.
Acknowledgements: Nil
References
- Thigpen MC, Whitney CG, Messonnier NE, Zell ER, Lynfield R, et al. Bacterial meningitis in the United States, 1998–2007. New England Journal of Medicine. 2011; 364(21): 2016-2025.
- Whitley RJ, Roizman B. Herpes simplex virus infections. The Lancet. 2001; 357(9267): 1513-1518.
- Weisfelt M, Beek D van de, L Spanjaard, J de Gans. Bacterial meningitis. Journal of Neurology. Neurosurgery & Psychiatry. 2006; 77(12): 1283-1284.
- Granerod J, Ambrose HE, Davies NW, Clewley PJ, Walsh LA, et al. The epidemiology of acute encephalitis in England: A multicentre, population-based prospective study. The Lancet Infectious Diseases. 2010; 10(12): 835-844.
- Koedel U, Scheld WM, Pfister HW. Pathogenesis and pathophysiology of pneumococcal meningitis. The Lancet Infectious Diseases. 2002; 2(12): 721-736.
- Almirall J, et al. The role of viruses in the aetiology of community-acquired pneumonia in adults. The Lancet. 2000; 355(9205): 1929-1933.
- Vandertop WP, Heins WH. Bacterial meningitis in adults. Acta Neurochirurgica. 2004; 146(6): 557-558.
- De Gans J, Van de Beek D. Dexamethasone in adults with bacterial meningitis. The New England Journal of Medicine. 2002; 347(20): 1549-1556.
- Tunkel AR, Barry HJ, Sheldon KL, Kaufman BA, Roos KL, et al. Practice guidelines for the management of bacterial meningitis. Clinical Infectious Diseases. 2017; 39(9): 1267-1284.
- Harrisons Principles of Internal Medicine, 22nd edition, Chapter. 1949; 137: 1096.