
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Redefining clinical expectations: A rare case report of toxic epidermal necrolysis in a glioblastoma patient undergoing concurrent temozolomide and cranial irradiation
Tabassum Samani*; Kirtika Verma; Deepanshi Jain; Utkarsha Singh; Avula Vineetha
Department of Radiation Oncology, SN Medical College, Agra, UP, India.
*Corresponding Author : Tabassum Samani
Department of Radiation Oncology, SN Medical College, Agra, UP, India.
Tel: +91-991-700-0857;
Email: tabassumsamani@yahoo.co.in
Received : Oct 05, 2024
Accepted : Oct 29, 2024
Published : Nov 05, 2024
Archived : www.jcimcr.org
Copyright : © Samani T (2024).
Abstract
Temozolomide (TMZ), an alkylating agent derived from dacarbazine, is approved for treating Glioblastoma Multiforme (GBM), an aggressive Central Nervous System (CNS) tumour. It is usually administered with radiation therapy after tumour surgery or as adjuvant chemotherapy. While TMZ demonstrates significant clinical efficacy, it is associated with its own toxicity profile and side effects, including leukopenia, thrombocytopenia, hepatotoxicity, nausea, constipation, and fatigue. A rare but reported adverse effect of concurrent TMZ treatment is Stevens-Johnson Syndrome (SJS), which can quickly progress to Toxic Epidermal Necrolysis (TEN). Very few cases of the same have been reported in the literature to date. We present our experience with the same- the case of a 40-year-old woman with GBM who developed sudden and rapidly progressing TEN during concurrent Chemoradiotherapy (CRT) involving TMZ administration with cranial irradiation. Ten days into treatment, she experienced a widespread maculopapular rash that started on her head, face, and eyes, and quickly spread across her body. The rash included erythematous, annular, targetoid, and purpuric macules, along with severe skin peeling, flaccid bullae and painful erosions covering over 70% of her body, with Nikolsky sign positive. Despite discontinuing both radiotherapy and temozolomide on day twelve, her condition worsened for several more days. She had been taking phenytoin and levetiracetam for seizure prevention before CRT, and these medications were also stopped when TEN developed. After intensive care and multidisciplinary treatment, her condition stabilized, and she fully recovered within two weeks. A significant aspect of this case was the extensive skin loss, which not only affected areas around the cranial radiotherapy sites but also spread across the entire body. After thoroughly assessing the onset, progression, and recovery of the disease in relation to the administration and discontinuation of various medications, it was determined that TMZ, either alone or in combination with radiotherapy, was most likely the trigger for his condition. Given that TEN is a systemic condition, the adverse reaction was more strongly linked to TMZ as the causative factor. Although TEN is an extremely rare side effect of TMZ, oncologists should be aware of this potential risk and closely monitor patients. TEN, if it develops, should be treated aggressively as it can be life-threatening. Patients should also be advised to report any unusual symptoms after starting TMZ.
Keywords: Temozolomide; Stevens Johnsons syndrome; Toxic epidermal necrolysis; Glioblastoma multiforme; Cranial radiotherapy; Drug hypersensitivity; Adverse effect.
Citation: Samani T, Verma K, Jain D, Singh U, Vineetha A. Redefining clinical expectations: A rare case report of toxic epidermal necrolysis in a glioblastoma patient undergoing Concurrent Temozolomide and Cranial Irradiation. J Clin Images Med Case Rep. 2024; 5(11): 3326.
Introduction
In clinical practice, Temozolomide (TMZ) is widely administered for treating gliomas, non-small cell lung cancer, leukemia, melanoma, lymphoma, and various solid tumours. Compared to other chemotherapy drugs, TMZ is the most effective in combating glioblastoma. Adjuvant treatment with TMZ begins 4 weeks after radiotherapy and continues for 6 cycles, with 5 consecutive days of treatment in each 28-day cycle [1]. Common adverse effects of TMZ include nausea, vomiting, anorexia, constipation, diarrhea, headache, and fatigue. Hematologic toxicities include neutropenia, leukopenia, thrombocytopenia, anemia and elevated liver enzymes [2]. Non-hematologic toxicities included dizziness, increased urine frequency, alopecia, pruritus/itching, skin rash, fever and lung infection. Rarely, SJS and TEN have been reported in a few cases linked to TMZ [3]. Stevens-Johnson Syndrome (SJS) is an uncommon, acute, and potentially life-threatening skin reaction characterized by extensive loss of skin and mucous membranes, often accompanied by systemic symptoms, which can rapidly progress to Toxic Epidermal Necrolysis (TEN). Medications are responsible for over 80% of cases. The classification of SJS/TEN is based on the percentage of body surface area affected: SJS: <10%; SJS/TEN overlap: 10-30% and TEN: >30%. Medications frequently associated with SJS and TEN include anticonvulsants like carbamazepine [4], lamotrigine, and phenytoin; sulfonamides such as cotrimoxazole and sulfasalazine; antibiotics like penicillins and cephalosporins; acetaminophen; NSAIDs like piroxicam [4]; contrast agents like iodinated contrast [5] and TMZ in a limited number of cases. Glioblastoma Multiforme (GBM) represents the most aggressive and widespread form of glioma [6,7]. It is the most prevalent primary brain tumour in adults, making up 45.2% of all primary malignant tumours in the brain and central nervous system (CNS) [8]. In GBM, TMZ is administered orally each day during radiation therapy. Data indicates that MGMT (O6-methylguanine-DNA methyltransferase) activity is linked to resistance to TMZ, with MGMT promoter hypomethylation and protein expression potentially serving as prognostic markers. However, neither MGMT protein levels nor promoter methylation status reliably predicts TMZ responsiveness, making it difficult to determine in advance whether a patient should undergo TMZ-based treatment [9]. Nevertheless, most patients these days are administered TMZ along with cranial irradiation because of its known benefits. Although TEN is an uncommon side effect of TMZ, some cases have been reported globally. Given its rarity, we aim to provide insight into this potentially severe adverse reaction that developed in our patient undergoing TMZ chemotherapy with whole-brain radiotherapy.
Case presentation
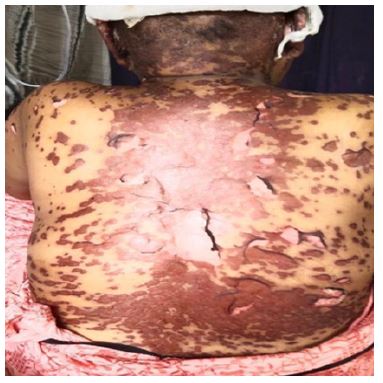
We present a case of a 48-year-old woman from an urban area in North India who sought care at the outpatient department, with complaints of headaches and intermittent weakness and numbness in her right upper and lower limbs for the past two months. She had a history of occasional tobacco use in the form of chewing and manjan, and she followed a non-vegetarian diet. Besides that, she had no other substance abuse history. Her bladder, bowel, and dietary habits were normal, and no significant past medical, drug, allergen, or family histories were noted. An initial MRI revealed a large solid-cystic mass lesion measuring 6.1 x 4.3 x 5.6 cm in the left high parietal brain parenchyma. The lesion displayed eccentric heterogeneous intensity, primarily consisting of central and eccentric cystic/necrotic components and moderate surrounding white matter oedema. It exerted a mass effect characterized by compression of the ipsilateral lateral ventricle, effacement of the ipsilateral sulcus spaces, an 11.5 mm midline shift toward the right side, and compression of the midbrain and thalami. Additionally, there was dilation of the contralateral lateral ventricle. Eccentric multiple foci of blooming were observed, suggesting haemorrhage. These findings were indicative of an intracranial space occupying lesion, probably a high-grade glioma. The patient was referred to a neurosurgeon, where she underwent a left temporoparietal craniotomy for near-total excision of the space-occupying lesion, accompanied by augmented duroplasty using a pericranial patch, under general anaesthesia. After the surgery, she was also started on seizure prophylaxis medications by the neurologist, namely phenytoin 100 mg three times daily and levetiracetam 500 mg twice daily. The histopathological report of the postoperative specimen revealed multiple soft tissue fragments that were grey-brown to light brown, measuring 1.7 x 1.5 x 0.5 cm. Microscopic examination revealed a cellular glial tumour made up of neoplastic astrocytes organized in sheets within a coarse fibrillary background. The tumour cells exhibited moderately pleomorphic nuclei, with areas of microvascular proliferation and necrosis interspersed throughout. Numerous mitotic figures (12-15 per 10 high-power fields) were also observed. These characteristics indicated a high-grade glioma consistent with glioblastoma, WHO grade IV. Two weeks post-surgery the patient reported to us for further treatment. The patient complained of numbness over the right upper and lower limbs post-surgery. On examination, all cranial nerve functions were intact. All sensory and motor functions were intact. The patient was slow to respond to voice commands and was slightly forgetful about some details of the family members. There was a healthy post-op scar mark present over the scalp. The post-op NCCT head revealed an ill-defined hypodense mass lesion measuring 2.4 x 2.2 cm in the left parietal lobe with perilesional oedema causing effacement of adjacent sulcal space likely residual lesion. Along with this craniotomy defect in the left parietal lobe and soft tissue swelling were noted along the left parietal aspect of the scalp and multiple air foci were seen in the right parietal lobe (postoperative changes). She was scheduled for whole brain radiotherapy using an external beam from a Cobalt-60 source, with 2D simulation performed. The plan was to deliver 50 Gray in 25 fractions at a rate of 2 Gray per fraction, with 5 fractions per week, along with a capsule of TMZ 100 mg taken orally one hour before radiotherapy. The patient was also started on injectable mannitol and dexamethasone for cerebral decompression. After ten fractions of radiotherapy combined with TMZ, the patient reported headache which was acute in onset, as well as erythematous, annular, targetoid, and purpuric macules covering the back and torso. She had erythematous scaly lesions with skin peeling involving the scalp, ears and nape of the neck which further deteriorated and escalated to necrosis over the scalp (Figure 1). She also experienced lip oedema, widespread scaling, serous and purulent discharge from lesions over buccal mucosa (Figure 2), eye redness and congestion in both eyes, eyelid oedema, pus discharge, crusting and conjunctivitis (Figure 3). Additionally, she had vomiting after meals, RTOG grade 3 mucositis [10], dermatitis and urethritis (Figure 4). All of these symptoms appeared suddenly and worsened within a day. The patient was also hypotensive. Her condition was suspected to be Stevens-Johnson Syndrome (SJS), and immediate dermatology consultation was requested. A skin biopsy was advised for the same but the patient declined to give consent for the procedure. Within a span of 24-48 hours, SJS progressed to TEN, characterized by flaccid bullae and large, painful erosions with a positive Nikolsky sign, affecting more than 40% of her body surface area (Figure 5). The patient had developed pustular and bullous erythematous lesions associated with skin peeling over the face and bilateral arms and other sites (Figure 6). The patient was treated intensively with topical ointments and regular dressing was done for the lesions, along with antibiotic coverage. It was suspected that TEN was a side effect of a medication the patient was currently taking. The suspected offending drugs namely phenytoin and levetiracetam were discontinued. After 2 days when the patient’s condition was not improving, radiotherapy along with TMZ were put on hold. Upon clinically diagnosing the condition to be SJS/TEN, the dermatology department advised initiating treatment with tablet Cyclosporin at a dose of 100 mg per oral daily. By that time, TEN had affected over 70% of the body surface area (Figure 7). On the commencement of TEN-specific treatment, the patient’s condition gradually improved, and she recovered within four weeks (Figure 8). After four weeks, when all the lesions had dried up and the patient’s general condition had improved, radiotherapy was resumed, but without concurrent TMZ. The patient subsequently completed all 25 fractions and has been on follow-up since then. She is now fully healed, with no relapses of the disease observed. Her performance status is good, and she continues to have regular follow-ups.







Discussion
Temozolomide (TMZ) is a drug known for its excellent penetration into the central nervous system and is one of the few medications demonstrated to significantly enhance survival in patients with GBM when used in combination with cranial irradiation [1]. TMZ happens to be the sole chemotherapeutic agent recommended for adjuvant therapy in GBM. The “Stupp protocol” refers to the combination of radiation therapy with TMZ, and has become the standard of care for the treatment of high-grade astrocytoma and glioblastoma since its publication in 2005 and has led to significant survival improvements [11,12]. In accordance with the common consensus and protocol, we also took our patient, a known case of high-grade glioblastoma, for whole brain radiotherapy along with concurrent TMZ [13]. TMZ, an analog of dacarbazine, possesses antineoplastic properties. Due to its small and lipophilic nature, TMZ can cross the Blood-Brain Barrier (BBB), making it one of the few drugs effective within the central nervous system [14]. TMZ is an alkylating agent prodrug that transfers a methyl group to purine bases in DNA, specifically targeting O6-guanine, N7-guanine, and N3-adenine. The main cytotoxic damage, O6-meth methylguanine (O6-MeG), can be repaired by the protein Methylguanine Methyltransferase (MGMT) in tumors that express it, or it may be tolerated in tumors deficient in Mismatch Repair (MMR) [15]. As a result, the presence of MGMT or MMR deficiency leads to resistance against TMZ. The standard treatment for GBM involves surgical removal of the tumor, followed by chemoradiotherapy as an adjuvant therapy [16]. It is also recommended to test for GFAP (glial fibrillary acidic protein), IDH (isocitrate dehydrogenase) mutation status, and O6-methylguanine-DNA methyltransferase (MGMT) promoter methylation status. The molecular profile encompasses both IDH-mutant and IDH-wild type variants, which can be identified through immunohistochemistry. GBM typically shows positivity for GFAP, vimentin, and S100, along with varying Ki-67 indices [17]. The toxicity profile of TMZ includes hematologic conditions such as thrombocytopenia, anaemia, and elevated AST/ALT levels. The most frequently observed non-hematologic side effects include nausea, vomiting, and loss of appetite [3]. There are no fatalities attributed to TMZ. Despite the presence of various toxicities, most are manageable and of lower severity. In the literature regarding TMZ, reports of SJS or TEN as side effects are quite rare. In our long clinical experience, this was the first time that a patient with GBM on TMZ and concurrent radiotherapy developed such a severe skin reaction, prompting us to go into depths and look into its literature.
SJS is an uncommon but severe and potentially life-threatening skin condition characterized by extensive loss of skin and mucous membranes affecting < 10% of body surface area, along with systemic symptoms, which can rapidly progress to TEN which covers more than 30% body surface area. The diagnosis of the same can be made clinically as well as histopathologically. Skin histology shows keratinocyte necrosis, necrosis of the epidermis (or epithelium), and mild infiltration of lymphocytes in the dermis. Direct immunofluorescence testing is negative [4]. However, in our case the patient refused skin biopsy, hence, the diagnosis was made clinically. Medications are responsible for over 80% of cases of SJS or TEN, mostly linked to hypersensitivity. While there are several drugs linked to TEN, we would like to highlight the potential role of the oral alkylating agent, TMZ, as a possible cause in this patient.The patient had also been taking oral phenytoin and levetiracetam for two months following surgery, which are also known to be linked with SJS [18], however, there were no signs of SJS during that period, and the rashes developed only within the first week of starting TMZ. In the second week of treatment by TMZ, the patient exhibited severe systemic symptoms consistent with TEN. Despite the prompt discontinuation of the suspected medications, namely, phenytoin and levetiracetam, the condition continued to deteriorate. It was only after the cessation of TMZ, that the condition stopped worsening. All these instances strongly indicate and also lead to our conclusion, that the condition is likely related to TMZ. The exact mechanism by which TMZ causes TEN is not known, but thought to involve an immune-related hypersensitivity response. This reaction leads to the activation of cytotoxic T cells and NK cells, which trigger keratinocyte apoptosis via the perforin-granzyme and Fas-FasL pathways. Additionally, reactive metabolites generated during TMZ metabolism, along with certain genetic predispositions like specific HLA alleles, may contribute to the risk and severity of TEN. While the precise cause varies, immune system dysregulation is believed to be central to the development of TMZ-induced TEN [19]. In a study this was established via patch test and controlled drug administration that TEN was in fact caused due to hypersen sitivity [7,20]. It remains unclear whether TMZ alone caused SJS or if its occurrence was influenced by the concurrent use of radiotherapy. While some researchers have suggested that the combination of radiotherapy and these drugs may have contributed to the development of TEN, this has not been definitively established. Case reports by Howell WR et al, Ferreira MR et al, and Yoshitake T et al suggest that radiotherapy could be a rare trigger for SJS [21-23], but the extremely rare occurrence of such adverse effects prevents a definitive causal relationship. A report by Sarma N. described a 46-year-old man who developed SJS and TEN overlap, resulting in significant localized skin loss on the head and neck after undergoing radiotherapy and TMZ for GBM [6]. Another case, reported by Pérez-Calderón R et al, suggests that TMZ may act as a trigger for SJS. This case described the development of TEN during treatment involving chemoradiotherapy and multiple medications, with TMZ and TMP-SMX in conjunction with cranial radiotherapy identified as the triggers, confirmed through controlled administration [7]. Although TEN is an extremely rare side effect of TMZ, oncologists should remain aware of this risk and carefully monitor patients. If TEN does develop, it requires aggressive treatment because it is potentially life-threatening. Patients should also be encouraged to report any unusual symptoms after starting TMZ. In our opinion, due to the rarity of such cases, every instance of TEN induced by TMZ and cranial radiotherapy should be carefully documented and reported to promote and facilitate future research.
Conclusion
The established protocol for the treatment of GBM consists of surgical resection followed by adjuvant chemoradiotherapy, usually incorporating TMZ. While TMZ is generally well tolerated and has a safe toxicity profile, this case report aims to raise awareness among oncologists about the potentially life-threatening side effect associated with TMZ, that is SJS which can also rapidly progress to TEN. Although TEN is a rare toxicity it must always be considered during cranial irradiation and TMZ therapy. It is crucial to prioritize careful monitoring and observation of patients as well as prior counseling about the possible side effects when prescribing this medication. We hope our case expands our knowledge of this rare but possible adverse event that may arise from TMZ treatment.
Abbreviations: TMZ: Temozolomide; SJS: Steven Johnsons Syndrome; TEN: Toxic Epidermal Necrolysis; MGMT: O6-Methylguanine-DNA Methyl Transferase; GBM: Glioblastoma Multiforme; BBB: Blood Brain Brain; MMR: Mismatch Repair; GFAP: Glial Fibrillary Acidic Protein; AST: Aspartate Aminotransferase; ALT: Alanine Transaminase; CRT: Concurrent Chemo Radiotherapy; CNS: Central Nervous System.
References
- Jezierzański M, Nafalska N, Stopyra M, Furgoł T, Miciak M, et al. Temozolomide (TMZ) in the Treatment of Glioblastoma Multiforme-A Literature Review and Clinical Outcomes. Current Oncology. 2024; 31(7): 3994-4002.
- Martínez-Garcia M, Álvarez-Linera J, Carrato C, Ley L, Luque R, et al. SEOM clinical guidelines for diagnosis and treatment of glioblastoma (2017). Clin Transl Oncol. 2018; 20(1): 22-28.
- Bae SH, Park MJ, Lee MM, Kim TM, Lee SH, et al. Toxicity Profile of Temozolomide in the Treatment of 300 Malignant Glioma Patients in Korea. Journal of Korean Medical Science. 2014; 29(7): 980.
- Oakley AM, Krishnamurthy K. Stevens Johnson Syndrome (Toxic Epidermal Necrolysis). PubMed. Treasure Island (FL): StatPearls Publishing. 2023.
- Carrera D, Ulloa JG. Iodinated contrast-induced Stevens-Johnson syndrome: A report of a rare complication for a common imaging agent. Journal of Vascular Surgery Cases and Innovative Techniques. 2022; 8(3): 455-7.
- Sarma N. Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis Overlap due to Oral Temozolomide and Cranial Radiotherapy. American Journal of Clinical Dermatology. 2009; 10(4): 264-7.
- Pérez-Calderón R, Gonzalo-Garijo MA, Corrales-Vargas S, Jiménez-Ferrera G, Rodríguez-Nevado I, et al. Toxic Epidermal Necrolysis in Polymedicated Patient Treated with Radiotherapy. Allergy, Asthma & Immunology Research. 2015; 7(2): 199.
- Li C, Li B, Wang H, Qu L, et al. Role of N6-methyladenosine methylation in glioma: recent insights and future directions. Cell Mol Biol Lett. 2023; 28(1): 103.
- Kitange GJ, Carlson BL, Schroeder MA, Grogan PT, Lamont JD, et al. Induction of MGMT expression is associated with temozolomide resistance in glioblastoma xenografts. Neuro-Oncology. 2009; 11(3): 281-91.
- The Radiation Therapy Oncology Group (RTOG) scoring criteria for. ResearchGate. 2021.
- Fernandes C, Costa A, Osório L, Lago Rc, Linhares P, et al. Current Standards of Care in Glioblastoma Therapy. Glioblastoma. 2017; 197-241.
- Rong L, Li N, Zhang Z. Emerging therapies for glioblastoma: current state and future directions. J Exp Clin Cancer Res. 2022; 41(1): 142.
- Stupp R, Hegi ME, Mason WP, van den Bent MJ, Taphoorn MJ, et al. European Organisation for Research and Treatment of Cancer Brain Tumour and Radiation Oncology Groups. National Cancer Institute of Canada Clinical Trials Group. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009; 10(5): 459-66.
- Ortiz R, Perazzoli G, Cabeza L, Jiménez-Luna C, et al. Temozolomide: An Updated Overview of Resistance Mechanisms, Nanotechnology Advances and Clinical Applications. Current Neuropharmacology. 2021; 19(4): 513-37.
- Zhang J, FG Stevens M, D Bradshaw T. Temozolomide: Mechanisms of Action, Repair and Resistance. Current Molecular Pharmacology. 2012; 5(1): 102-14.
- Kaina B. Temozolomide, Procarbazine and Nitrosoureas in the Therapy of Malignant Gliomas: Update of Mechanisms, Drug Resistance and Therapeutic Implications. Journal of Clinical Medicine. 2023; 12(23): 7442.
- Tejaswi Kanderi, Vikas Gupta. Glioblastoma Multiforme. Nih.gov. StatPearls Publishing. 2022.
- Alexandru Iorga, B Zane Horowitz. Phenytoin Toxicity. Nih.gov. StatPearls Publishing. 2023.
- Chung WH, Hung SI, Yang JY, Su SC, Huang SP, et al. Granulysin is a key mediator for disseminated keratinocyte death in Stevens-Johnson syndrome and toxic epidermal necrolysis. Nat Med. 2008; 14(12): 1343-50.
- Harr T, French LE. Toxic epidermal necrolysis and Stevens-Johnson syndrome. Orphanet Journal of Rare Diseases. 2010; 5(1).
- Howell Wr, Knight Al, Scruggs Hj. Stevens-Johnson Syndrome After Radiotherapy. Southern Medical Journal. 1990; 83(6): 681-3.
- Miguel Reis Ferreira, Amado A, Jorge M, Isabel Monteiro Grillo. Stevens Johnson Syndrome in a patient undergoing gynaecological brachytherapy: An association or an incident? Reports of Practical Oncology & Radiotherapy. 2011; 16(3): 115-7.
- Tanaka N, Nakatani S, Chisato Yahiro, Takai T. Erythema multiforme associated with cancer radiotherapy: A single‐institution case series and literature review. Journal of dermatology. 2022; 50(5): 656-63.