
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Severe brucella endocarditis on native tricuspid valve with a good outcome: A case report
Badra Bahri1,2*; Chemsi Anissa1,2; Touj Hager1,2; Brahmi Wala1,2; Belgacem Ines1,2; Garbaa Yesmine1,2; Yesmine Benzarti1,2; Sedghiani Ines1,2; Ennaceur Manel1,2; Zaghdoudi Imen1,2; Nebiha Borsali-Falfoul1,2
1Faculty of Medicine, University of Tunis El Manar, Tunis 1006, Tunisia.
2Emergency Department, Habib Thameur University Hospital, Tunis 1089, Tunisia.
*Corresponding Author : Badra Bahri
Faculty of Medicine, University of Tunis El Manar, Tunis 1006, Tunisia.
Tel: +21626137531;
Email: bahribadra@gmail.com
Received : Oct 07, 2024
Accepted : Oct 29, 2024
Published : Nov 05, 2024
Archived : www.jcimcr.org
Copyright : © Bahri B (2024).
Abstract
Background: Brucellosis causes polymorphic symptoms. Infective Endocarditis (IE) remains an exceptional location. We report a rare case of tricuspid brucella endocarditis.
Case presentation: A 48 year old man, with a history of psoriasis, Intravenous (IV) opiate drug addiction and regular use of raw, unpasteurized milk, presented to the emergency department for fever, myalgia and painful urination that has been going on for three weeks. On examination: Respiratory rate was 28 cycle /minute (cpm), oxygene pulse oxymetry was at 94%, blood pressure was 108/59 mmHg, heart rate at 130 beats per minute without heart murmur, the patient had normal consciousness, hepatomegaly at 20 cm, fever at 38.8°C, bilateral edema of the lower limbs. The electrocardiogram showed sinus tachycardia. Blood test showed: leukocytosis at 11810 E/mm3, hemolytic anemia with an hemoglobin level at 7 gr/dl, C-reactive protein level was 361 mg/l, urea=32.8 mmol/l, creatinine=238 umol/l. Cytobacteriological urine exam was positive and isolated Enterobacter Cloacae. The diagnosis of urinary sepsis was made. The computed tomography showed hepatosplenomegaly with splenic infarction, bilateral nodular lesions of the pulmonary bases suggestive of septic emboli and sacroilitis. Bed side cardiac ultrasound which showed: Tricuspid vegetation with a moderate tricuspid dysfunction, the cardiac right cavities were normal. The Blood cultures were positive for Brucella Melitensis.
Antibiotic therapy targeted staphylococcus was changed to the association of rifampicin, doxycycline and cefotaxim. After six weeks of antibiotic therapy size of tricuspid vegetation on cardiac ultrasound was (31 x 21 mm). The patient had then a valve replacement with a bio prosthesis and was discharged after two months. Patient had a good outcome at 6 months control visit.
Conclusion: This case underlines that Brucella Melitensis can be the cause of a right IE on the native valve. Good outcome is based on with targeted antibiotic therapy with timely cardiac surgery.
Keywords: Endocarditis; Emergency; Brucella; Sepsis.
Abbreviations: IE: Infective Endocarditis; IV: Intravenous; CT: Computed Tomography; ED: Emergency Department.
Citation: Bahri B, Anissa C, Hager T, Wala B, Ines B, et al. Severe brucella endocarditis on native tricuspid valve with a good outcome: A case report. J Clin Images Med Case Rep. 2024; 5(11): 3327.
Introduction
Background: Brucellosis is a worldwide zoonotic infection caused by a gram-negative intracellular bacillus of the genus Brucella. Brucellosis is transmitted to humans via consumption of unpasteurized animal products or inhalation of aerosolized infected particles and through contact with skin or mucous membranes of infected animal tissue [1]. It frequently presents with polymorphic symptoms such as fever and malaise, but can lead to multiorgan failure [2].
In this article, we report an observation of tricuspid native brucella endocarditis which needed surgical treatment.
Case presentation
A 48 year old north african man, with a history of psoriasis and Intravenous (IV) opiate drug addiction, presented to the Emergency Department (ED) for fever, myalgia and painful urination that has been going on for three weeks. The patient reported the regular consumption of raw, unpasteurized milk.
On examination: Respiratory rate was 28 cycle /minute, oxygene pulse oxymetry was at 94%, blood pressure was 108/59 mmHg, heart rate at 130 beats per minute without heart murmur, the patient had normal consciousness, no sensorimotor deficit, hepatomegaly at 20 cm, fever at 38.8°C, bilateral edema of the lower limbs.
The electrocardiogram showed sinus tachycardia
Blood test showed: Leukocytosis at 11810 E/mm3 with predominantly polynuclear neutrophiles, hemolytic anemia with hemoglobin level at 7 g/dl, with schizocytes and with positive coombs test, platelets Level was 124000 E/mm3, C-reactive protein level was 361 mg/L, acute kidney failure, urea = 32.8 mmol/l, creatinine = 238 μmol/l.
Cytobacteriological urine exam was positive and isolated Enterobacter Cloacae. The diagnosis of urinary sepsis was made.
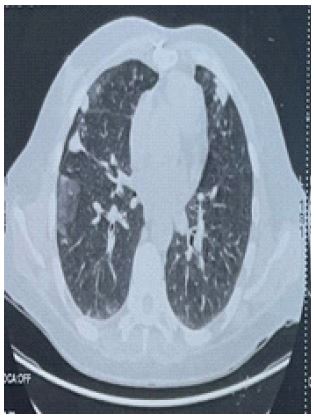
The computed tomography showed hepatosplenomegaly with splenic infarction, bilateral nodular lesions of the pulmonary bases suggestive of septic emboli (Figure 1) and sacroilitis (Figure 2).
Given the context of drug addiction, prolonged fever, areas of splenic infarction and septic emboli, we performed a bed side cardiac Ultrasound which showed: Tricuspid vegetation (34 x 24 mm) with a moderate tricuspid dysfunction, the cardiac right cavities were normal (Figure 3).
The Probabilistic initial antibiotic therapy targeted Staphylococcus aureus based on oxacillin, gentamycin and ciprofloxocin.
The Blood cultures which were done on specific medium (Colombia agar) were positive for Brucella Melitensis, Wright, Rose Bengal and hepatitis B serologies were positive.
Antibiotic therapy was changed to the association of rifampicin, doxycycline and cefotaxim. Solumedrol bolus corresponding to 1 mg/kg/day have been prescribed for hemolytic anemia.
After six weeks of antibiotic therapy size of tricuspid vegetation on cardiac ultrasound was (31 x 21 mm). The patient had then a valve replacement with a bio prosthesis after fifty one days of antibiotic therapy. He was discharged after two months. Patient had a good outcome after 6 months at follow-up visit.


Discussion
Infective Endocarditis (IE) is an exceptional location of brucella. In a multicenter Greek study over 20 years from different centers reported an incidence of IE localisation up to 4% among all Brucella infection [3].
Brucella endocarditis involves the aortic valve in 75% of the cases followed by an equal 8.3% involvement of each of the following: mitral valve alone, aortic along with mitral valve and prosthetic valve [4].
In IV drug users, like our patient, the tricuspid valve is the most affected valve. Injection of drugs results in entry of particulate into the circulatory system resulting in structural damage to the endothelium of the valve.
Right IE on the native tricuspid valve in IV drug users are frequently due to staphylococcus [5]. Systemic review of the literature reported the occurrence of Brucella endocarditis in prosthetic valves or in the left heart but not in a native tricuspid valve [6]. The germ isolated in our case was Brucella Melitensis, making our observation extremely rare.
The most common presenting complaint of brucellosis is a fever of unknown origin associated with night sweats, malaise, asthenia and arthralgia. About one-third of patients with brucellosis develop focal osteoarticular complications with complications accounting for more than half of cases [7,8].
The sign suggestive of brucellosis in our case was sacroiliitis, the symptoms were confused with those of the urinary infection. The diagnosis of Brucella infection relies on blood cultures and serological tests. In the literaure blood cultures are positive only in 40-70% of cases [9]. Microbial identification in our case was obtained on blood cultures which was done on specific medium (Colombia agar) and on serology. The microbiologist must be involved in sacroiliitis to initiate the necessary identification techniques, such as oxidase, catalase and urea tests.
Medical treatment of brucella IE is based on antibiotic therapy adapted to microbiological data [10]. Mentionned that large, persistent tricuspid valve vegetations (>20 mm) is an indication of surgical treatment given the risk of recurrent pulmonary emboli with or without concomitant right heart failure. Our patient size vegetation was (31 x 21) mm after six weeks of antibiotic therapy. Surgical treatement was then indicated. The best results are obtained if valve replacement is combined with antibiotic therapy [11]. Keshtkar-Jahromi et al. conducted an extensive review of Brucella IE cases between 1966 and 2011 and concluded that patients who did not undergo surgery have an increased risk of mortality [12]. However, only a few studies report successful treatment of native or prosthetic valve IE with antibiotics alone [13-15].
Although it is rare to have endocarditis caused by Brucella, nearly 80% of mortality in brucellosis is secondary to endocarditis [16]. In our case the patient had a good outcome after six months follow up when combining medical and cardiac surgery.
Conclusion
Endocarditis is a rare focal complication of brucellosis, with a poor prognosis. It can involve prothetic valve, mitral valve but also native tricupsid valve. Cardiac Bed side ultrasound realised in the ED allowed quick diagnosis of endocarditis. Emergency physician should be aware of this rare entity and perform blood culture as soon as possible and collaborate with microbiologists at the slightest clinical suspicion.
Treatment often requires a multidisciplinary approach, including long-term combination antibiotic regimen and cardiac surgery.
Declarations
Acknowledgments: Not applicable.
Author contribution: BB drafted the case report, reviewed litterature, and wrote the manuscript, CA, TH, BI, BW, BY, ZI, BY, SI cared for the patient, and reviewed literature, NBF revised and supervised the manuscript. All authors read and approved the final manuscipt.
Funding: Not applicable.
Availability of data and materials: All data generated and analysed during this study are included in this published article.
Ethical approval and consent to participate: Not applicable.
Consent for publication: Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the editor-in-chief of this journal.
Conflict of interest: All the authors certify that they have no affiliations with/or involvement in any organization or entity with any financial interest in the subject matter or materials discussed in this manuscript.
References
- Pappas G, Akritidis N, Bosilkovski M, Tsianos E. Medical progress brucellosis. N Engl J Med. 2005; 352(22): 2.
- Muhammad A Raza, Komal Ejaz, Daniel Kazmierski. Brucella Endocarditis of the Native Mitral Valve Treated with Antibiotics. Cureus. 2020; 12(5): e8167.
- Hadjinikolaou L, Triposkiadis F, Zairis M, et al. Successful management of Brucella melitensis endocarditis with combined medical and surgical approach. Eur J Cardiothorac Surg. 2001; 19(6): 806-10.
- Reguera J, Alarcon A, Miralles F, Pachon J, Juarez C, et al. Brucella endocarditis: Clinical, diagnostic, and therapeutic approach. Eur J Clin Microbiol Infect Dis. 2003; 22: 647-650.
- Frank Seghatol, Isaac Grinberg. Left-sided endocarditis in intravenous drug users: A case report and review of the literature. Echocardiography. 2002; 19(6): 509-11.
- Brucella Prosthetic Valve Endocarditis: A Systematic Review journal of the Saudi Heart Association. J Saudi Heart Assoc. 2021; 33(3): 198-212.
- Dahouk SA, Schneider T, Jansen A, et al. Brucella endocarditis in prosthetic valves. Can J Cardiol. 2006; 22(11): 971-4.
- Franco MP, Mulder M, Gilman RH, Smits HL. Human brucellosis. Lancet Infect Dis. 2007; 7(12): 775-86.
- Yagupsky P. Detection of brucellae in blood cultures. J.Clin.Microbiol. 1999; 37: 3437-3442.
- Shmueli H, Thomas F, Flint N. Right-Sided Infective Endocarditis: Challenges and Updates in Diagnosis and Treatment. J Am Heart Assoc. 2020; 9(15): e017293.
- M O Jeroudi 1, M A Halim, E J Harder, M B Al-Siba’i, G Ziady, et al. Brucella endocarditis. Br Heart J. 1987; 58(3): 279-83.
- Keshtkar-Jahromi M, Razavi S-M, Gholamin S, Keshtkar-Jahromi M, Hossain M, et al. Medical versus medical and surgical treatment for Brucella endocarditis. Ann Thorac Surg. 2012; 94(6): 2141-6.
- Lee SA, Kim KH, Shin HS, Lee HS, Choi HM, et al. Successful medical treatment of prosthetic mitral valve endocarditis caused by Brucella abortus. Korean Circ J. 2014; 44(6): 441-3.
- Mert A, Kocak F, Ozaras R, et al. The role of antibiotic treatment alone for the management of Brucella endocarditis in adults: A case report and literature review. Ann Thorac Cardiovasc Surg. 2002; 8(6): 381-5.
- Murdaca G, Colombo BM, Caiti M, Cagnati P, Massa G, et al. Remission of Brucella endocarditis in a patient with mitral valve mechanical prosthesis by antibiotic therapy alone: A case report. Int J Cardiol. 2007; 117(1): e35-6.
- Peery TM, Belter LF. Brucellosis and heart disease: II. Fatal brucellosis: A review of the literature and report of new cases. Am J Pathol. 1960; 36(6): 673-97.