
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Persistance of uterine arteriovenous malformation after embolization: Case report
Salma Tahri Jautei1*; Nada Douraidi1; Mohamed Elfarjani1; Fatima Elhassouni1; Pr. Samir Bargach2
1Department of Obstetrics and Gynecology, Oncology and, High-Risk Pregnancies, Maternity Souissi Ibn Sina, University Mohammed V Rabat, Morocco.
2Chief, Department of Obstetrics and Gynecology, Oncology and, High-Risk Pregnancies, Maternity Souissi Ibn Sina, University Mohammed V Rabat, Morocco.
*Corresponding Author : Salma Tahri Jautei
Department of Obstetrics and Gynecology, Oncology and, High-Risk Pregnancies, Maternity Souissi Ibn Sina, University Mohammed V Rabat, Morocco.
Email: salma-tahri@hotmail.com
Received : Oct 11, 2024
Accepted : Nov 01, 2024
Published : Nov 08, 2024
Archived : www.jcimcr.org
Copyright : © Jautei ST (2024).
Abstract
Uterine arteriovenous malformation is an abnormal connection between the arterial and venous system. The early diagnosis of the AVM in hemodynamically stable patient can dictate the management and prevent from a life threatening condition.
In this report, we describe a case of uterine arteriovenous malformation and its management.
Keywords: Uterine arteriovenous malformation; Embolization.
Citation: Jautei ST, Douraidi N, Elfarjani M, Elhassouni F, Bargach S. Persistance of uterine arteriovenous malformation after embolization: Case report. J Clin Images Med Case Rep. 2024; 5(11): 3332.
Introduction
Uterine arteriovenous malformation AVM is a potentially rare and life threatening condition, due to abnormal vascular connections, characterized by severe per vaginal bleeding [1]. Its either congenital or acquired. Color doppler ultrasound is a crucial tool for diagnosis. With the evolution of trans-catheter uterine embolization in the last decades, conservative treatment is more used with high success rate.
Case report
This is a case report for a 24-year-old G4PtiAti healthy woman who developed heavy vaginal bleeding aOer dilatation and suctioning of the conception product. Her first pregnancy was a spontaneous miscarriage at 10 weeks of gestation.
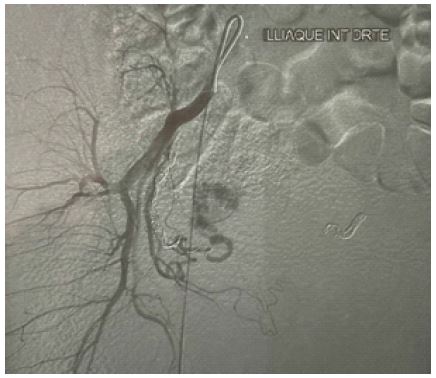
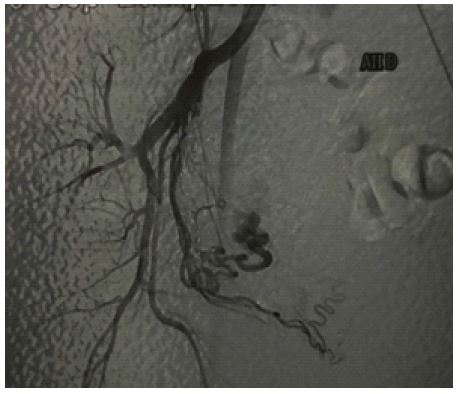
She got pregnant for the second time 6 months later and her doctor has a doute about a trophoblastic gestational disease, so he referred her to an OB who performed an ultrasound which showed a non-viable pregnancy at 7 weeks of gestation. She was then admiXed to the OR where she was treated by an aspiration of the conception product. After 2 months, the patient was admixed to the hospital for heavy bleeding where an ultrasound with doppler was performed showing a uterine arteriovenous malformation. Arteriography confirmed a right latero-uterine AVM, showing a myometrial component extending within the endometrial cavity with a large feeding artery coming from the right uterine artery. After 1 week of her admission, she was treated by super selective uterine artery embolization. Arteriography was performed 3 months after showing a residual AVM and a second embolization was suggested to the patient who consent to it.
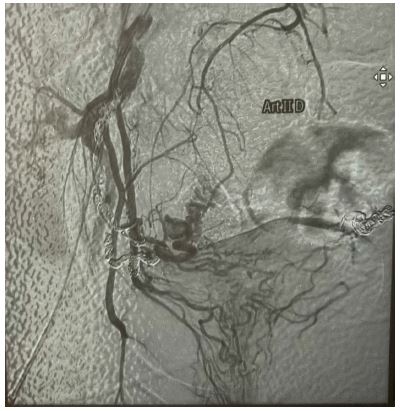
Before the second embolization, an ultrasound showed a gestational sac and a hCG dosage confirmed a third pregnancy but unfortunately was miscarried at 12 weeks of gestation. The second embolization was not a complete success either and arteriography showed the persistence of the AVM. However, the symptomatology of the patient decreased considerably and didn’t present any abnormal vaginal bleeding.
Actually, the patient is pregnant for the fourth time with twins at 34 weeks with no manifest complication and programmed to cesarean section at 38 weeks.
Discussion
Uterine Arteriovenous Malformations (AVMs) is a rare life threatening disease both on the vital and functional level [2], du to an abnormal connections between myometrial arterial and venous system of the uterus. They are classified into two categories: congenital and acquired.
The congenital category is a rare condition that occur to failure of differentiation during the embryogenesis of primitive vascular structure. The acquired AVM is usually manifest an reproductive age woman, du to trauma to the uterine vasculature. Such as dilatation and curetage, gestational trophoblastic disease, cesarean section, uterine infection, myomectomy and gynecological malignancy [3-5]. Even that the incidence of uterine AVM is only 0.1%, in literature, acquired uterine AVMs are more frequently presented [6].
In this case, the patient had a history of one prior aspiration abortion, but was asymptomatic prior to her presentation.
Patients commonly present with bleeding which can be intermittent or heavy. Causing a serious morbidity such as life-threatening hemorrhage, and hypovolemic shock due to severe bleeding.
The diagnosis of uterine AVM is made on the abdominal, trans-vaginal ultrasound and color doppler imaging, showing a hyper vascular area with turbulent flow and multiple tortuous feeding vessels with high velocity and low resistance in the myometrium of the uterus is specific for the uterine AVM [7,8]. However, the ultrasound coud be nonspecific, leading to differential diagnosis such as retained products of conception, cesarean scar pregnancy, abnormal placentation. Therefore the angiography is considered the gold standard for the diagnosis and determination of feeding vessels in AVM [9]. In our case, the ultrasound suggested an arteriovenous malformation, which was confirmed by a CT angiography and guided the treatment and surveillance of the patient.
The management of uterine AVM is determined by the hemodynamic stability of the patient also their fertility project. Since the late 80s, the endo-vascular embolization treatment has become the first choice for conservative treatment of AVMs [10]. In the other hand the surgical treatment by an hysterectomy is reserved to either patients who completed their fertility project or in the facilities with limited access to interventional radiology, or is some cases to patient with unstable hemodynamic statuts. The embolization can be repeat to some certain patient due to continued symptoms, with a high success rate considered to patient undergoing just one trans-catheter uterine artery embolization ranging from 69% to 95% [11,12].
In the presented case, due to residual AVMs and persistance of the symptoms. The patient underwent a second trans-catheter uterine embolization. Three months later, the patient presented a viable a bichorial biamniotic twin pregnancy of 11 weeks gestation. With a closer monitoring of this pregnancy and explanation of the risks, the patient consented to complete the pregnancy.
Conclusion
Medical management is effective partially or completely resolving uterine arteriovenous malformation, also the treatment of choice for preserving the fertility.
Potential conflicts of interest: The authors declare no conflicts of interest.
References
- Habte R, Yosef A, Bedaiwy M. Medical Management of Uterine Arteriovenous Malformation: A Case Series. Eur J Obstet Gynecol Reprod Biol. 2022; 274: 48-55. doi:10.1016/j.ejogrb.2022.05.005.
- Peitsidis P, Manolakos E, Tsekoura V, Kreienberg R, Schwentner L. Uterine arteriovenous malformations induced after diagnostic curettage: A systematic review. Arch Gynecol Obstet. 2011; 284(5): 1137-1151. doi:10.1007/ s00404-011-2067-7.
- Yazawa H, Soeda S, Hiraiwa T, et al. Prospective evaluation of the incidence of uterine vascular malformations developing after abortion or delivery. J Minim Invasive Gynecol. 2013; 20(3): 360-367. doi:10.1016/ j.jmig.2012.12.008.Yazawa H, Soeda S, Hiraiwa T, et al. Prospective evaluation of the incidence of uterine vascular malformations developing after abortion or delivery. J Minim Invasive Gynecol. 2013; 20(3): 360-367. doi:10.1016/ j.jmig.2012.12.008.
- Yammine K, Osman D, Daher J, Salha M, Mouawad S. Acquired uterine arteriovenous malformation treated with superselective embolization: Case report. Radiol Case Rep. 2023; 18(6): 2204-2208. doi:10.1016/ j.radcr.2023.03.018.
- Yoon DJ, Jones M, Taani JA, Buhimschi C, Dowell JD. A Systematic Review of Acquired Uterine Arteriovenous Malformations: Pathophysiology, Diagnosis, and Transcatheter Treatment. Am J Perinatol Rep. 2015; 06: e6-e14. doi:10.1055/s-0035-1563721.
- Yazawa H, Soeda S, Hiraiwa T, et al. Prospective evaluation of the incidence of uterine vascular malformations developing after abortion or delivery. J Minim Invasive Gynecol. 2013; 20(3): 360-367. doi:10.1016/ j.jmig.2012.12.008.
- Grivell RM, Reid KM, Mellor A. Uterine arteriovenous malformations: A review of the current literature. Obstet Gynecol Surv. 2005; 60(11): 761-767. doi:10.1097/01.ogx.0000183684.67656.ba.
- Timor-Tritsch IE, Haynes MC, Monteagudo A, Khatib N, Kovács S. Ultrasound diagnosis and management of acquired uterine enhanced myometrial vascularity/arteriovenous malformations. Am J Obstet Gynecol. 2016; 214(6): 731.e1-731.e10. doi:10.1016/j.ajog.2015.12.024.
- Giurazza F, Corvino F, Silvestre M, et al. Uterine Arteriovenous Malformations. Semin Ultrasound CT MRI. 2021; 42(1): 37-45. doi:10.1053/ j.sult.2020.08.002.
- Forssman L, Lundberg J, Scherstén T. Conservative treatment of uterine arteriovenous fi stula. Acta Obstet Gynecol Scand. 1982; 61(1): 85-87. doi:10.3109/00016348209156958.
- O’Brien P, Neyastani A, Buckley AR, Chang SD, Legiehn GM. Uterine arteriovenous malformations: from diagnosis to treatment. J Ultrasound Med off J Am Inst Ultrasound Med. 2006; 25(11): 1387-1392; quiz 1394-1395. doi:10.7863/jum.2006.25.11.1387.
- Kim T, Shin JH, Kim J, et al. Management of bleeding uterine arteriovenous malformation with bilateral uterine artery embolization. Yonsei Med J. 2014; 55(2): 367-373. doi:10.3349/ymj.2014.55.2.367.