
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Managing accidental arterial cannulation mishaps in hemodialysis catheter placement: A case report
Gade Sandeep1; Subrata K Singha2; Swati Vijapurkar3*; Shobika Sridhar4; Keerthi Chinnadurai4
1Department of Cardiac Anaesthesiology, All India Institute of Medical Sciences, Raipur, India.
2Professor, Department of Anaesthesiology, All India Institute of Medical Sciences, Raipur, India.
3Senior Resident, All India Institute of Medical Sciences, Raipur, India.
4Junior Resident, All India Institute of Medical Sciences, Raipur, India.
*Corresponding Author : Swati Vijapurkar
Senior Resident, All India Institute of Medical Sciences, Raipur, India.
Tel: 9901967469;
Email: swativijapurkar24@gmail.com
Received : Sep 20, 2024
Accepted : Nov 05, 2024
Published : Nov 12, 2024
Archived : www.jcimcr.org
Copyright : © Vijapurkar S (2024).
Abstract
Accidental insertion of a hemodialysis catheter into an artery is a rare but potentially serious complication encountered during catheter placement. Hemodialysis (HD) catheters are of large caliber and direct removal of the catheter can lead to torrential hemorrhage or dislodgement of a thrombus. A multidisciplinary approach for confirmation of the location of the misplaced catheter by radiographic techniques and an appropriate plan for surgical removal must be prepared to prevent serious complications. Here we present a case of improper hemodialysis catheter placement into the artery and removal of which required a sternotomy and exploration.
Keywords: Hemodialysis catheter; Ultrasound; Exploration.
Citation: Sandeep G, Singha SK, Vijapurkar S, Sridhar S, Chinnadurai K. Managing accidental arterial cannulation mishaps in hemodialysis catheter placement: A case report. J Clin Images Med Case Rep. 2024; 5(11): 3337.
Introduction
Hemodialysis (HD) catheters are artificial conduits used to access intravascular or intraperitoneal space. These are an essential part of renal replacement therapy and are usually made of polyurethane or silicone [1]. The placement of these catheters, their utilization and removal have associated risks and complications. These are double-lumen catheters and are usually placed at the bedside in an inpatient setting, using the Seldinger technique. The most preferred access site is the right Internal Jugular Vein (IJV) with the advantage of its straight trajectory and shorter distance to the right atrium [2]. Other venous sites include the left IJV and the common femoral veins. Complications of hemodialysis catheter insertion may be acute or chronic. Acute complications include vascular injury and bleeding, hematoma, pneumothorax, accidental arterial puncture/cannulation and arrhythmias. Accidental puncture or cannulation of an artery (1 in 100 incidence) with a large caliber cannula can lead to serious complications like bleeding, hematoma leading to airway obstruction, pseudo-aneurysm, arteriovenous fistula and stroke [3]. Here we present a case of improper HD catheter placement into the artery and removal of which required a sternotomy and exploration.
A written consent has been obtained by the patient’s family to publish this case report.
Case presentation
An 11-year-old girl child was admitted to the paediatric intensive care unit with complaints of fever and altered behaviour for the past two days. The child’s Glasgow Coma Score (GCS) at the time of admission was E4V2M5. The child was initially managed with intravenous fluids and Inj. Paracetamol and pertinent investigations were ordered and performed. On ICU Day 2, the child developed shortness of breath and tachypnea for which the child was put on Non-Invasive Ventilation (NIV) by face mask. The child was noncompliant with the NIV and a decision was soon made to intubate and mechanically ventilate the child. Lumbar puncture was performed, and the Cerebrospinal Fluid (CSF) was analyzed for encephalitis or meningitis. The CSF was negative for bacterial, viral and tuberculosis. With a working diagnosis of autoimmune encephalitis, the child was started on Inj. Methylprednisolone at 2 milligrams per Kilogram (mg/Kg) for 5 days.
As there was no improvement, plasma exchange was planned as the next therapeutic intervention. This required the insertion of a hemodialysis catheter, and the right internal jugular vein was selected for the insertion. Under landmark guided technique and Seldinger’s approach, 12 French (Fr) HD catheter (Arrow-Clark VectorFlow) was inserted by the pediatric resident. The puncture was performed directly with the large bore needle. Post insertion of the catheter, upon removal of the guide wire, a bright red spurt of blood was noted. Suspecting intra-arterial placement of the catheter, a sample was immediately sent for arterial blood gas analysis and a pressure monitoring line was connected to the catheter to confirm the position. Both the arterial blood gas analysis and pressure transduction confirmed an intra-arterial position of the catheter.
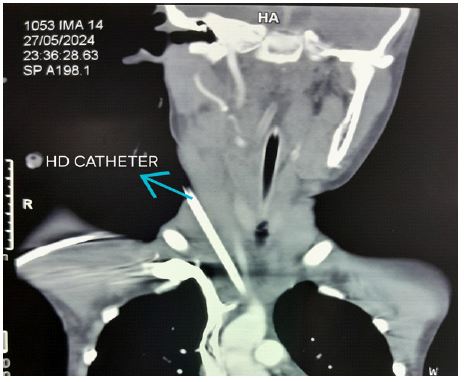
The catheter was left in situ and the patency of the catheter was maintained with continuous unfractionated heparin flush solution to prevent thrombus formation. In the following hour, Contrast-Enhanced Computed Tomography (CECT) (Figure 1) of the neck and thorax and a chest X-ray (Figure 2) was done to find out the exact location of the catheter. CECT showed the presence of the catheter in the junction of the right subclavian and the right common carotid artery.
The opinion of the Cardiothoracic and vascular surgeons was taken in view of further management. Given the posterior position of the catheter in the subclavian-carotid junction and the possibility of shearing of the vessels and torrential haemorrhage, hence, direct removal of the catheter was not advised. A decision was taken to remove the catheter in the Operation Room (OR) on the next day with the possibility of sternotomy and exploration.
In the OR, the child was connected to the ventilator and monitors were attached as per the American Society of Anaesthesiologists standards. Titrated doses of propofol (10 mg) and fentanyl (10 microgram) were administered. Muscle relaxation was achieved with the injection of atracurium (10 milligram). Anaesthesia was maintained with a combination of oxygen with air (50:50) and sevoflurane at a MACage of 0.6-0.7. Post induction, a 5 Fr. Central venous catheter (Multicath 3 UP, Vygon, Ecouen) was secured in the left femoral vein and an arterial cannula was secured in the left radial artery. Intraoperative neuromonitoring could not be performed due to non availability.
A midline full sternotomy was performed to adequately expose the field for exploration and for the exact location of the site where the catheter entered the artery to avoid shearing of the artery and torrential hemorrhage, which would be difficult to manage without sternotomy. A sternotomy was done because of a better control of the insertion site rather than through the neck alone. As the entry site of the catheter could not be visualized, the incision was extended into the neck to adequately expose the right brachiocephalic artery and itsbranches. The catheter was then visualized at the junction of the subclavian artery and the common carotid artery as mentioned in the CECT report (Figure 3).
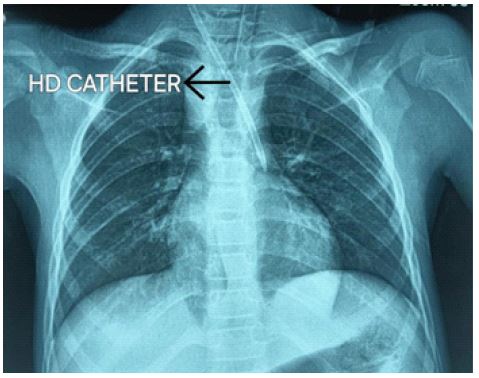
HD: Hemodialysis; AP view: Antero-posterior view.
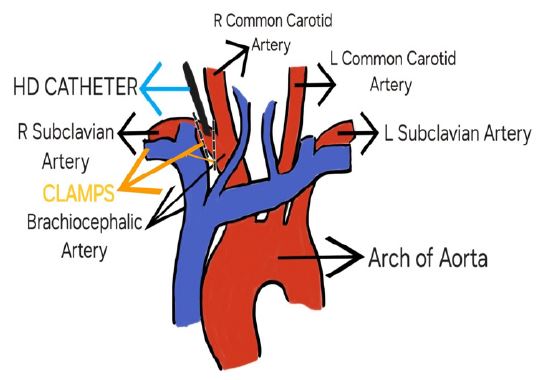
HD: Hemodialysis; R: Right; L: Left; Dotted line shows the position of the clamps.
Note: This Illustrative diagram was created by the authors Dr Swati Vijapurkar and Dr Subrata K. Singha and has not been taken from any source and does not require any permissions.
Unfractionated heparin at a dose of 1 mg/Kg (20 mg) was given before the application of clamps to prevent thrombosis. A clamp distal to the tip of the catheter was applied over the right subclavian artery and the catheter was pulled out from the insertion point in the neck by the attending anesthesiologist. Following the removal of the catheter, to control the bleeding, a proximal clamp was placed over the right subclavian artery, and the rent was secured using purse string sutures (prolene 5.0). The clamps were removed, and the radial artery pulse was checked by palpation. After achieving hemostasis, the closure was performed, and the child was shifted back intubate to the paediatric intensive care unit for the management of the primary condition and mechanically ventilated electively for further management of the primary condition.
Post-procedure, a hemodialysis catheter was inserted in the right femoral vein. Five cycles of plasma exchange was performed but unfortunately the child did not show any improvement. Post-operative neurological examination revealed GCS of E2VTM5. Post-procedure a Non-Contrast Computed Tomography (NCCT) head was performed and did not show any areas of infarct.
Discussion
Hemodialysis catheters have long and thick lumens and are of large calibre. They are associated with an increased risk of thrombotic complications [4]. Accidental arterial puncture/cannulation can lead to serious complications. This emphasizes the use of ultrasound (US) guided techniques, especially in pediatric patients. Its value has been shown not only in preventing complications of venipuncture but also in catheter placement and real-time checks for potential complications [5,6]. The advantages of using real time ultrasonography for central venous catheterisation are improved first pass success rate and fewer complications like arterial puncture, pneumothorax and hematoma formation [7].
In such instances, the direct removal of the catheter might lead to disastrous complications like shearing/ torrential haemorrhage and so must not be performed. In a study by [8] on arterial trauma during central venous cannulation, the rate of serious complications following arterial cannulation by large calibre cannulae was 47% and suggested prompt surgical or endovascular treatment to be the safest approach. In this case, surgical exploration in a controlled environment was considered the best option to remove the catheter.
Suspicion of accidental arterial puncture/cannulation must be done when there is excessive or pulsatile backflow of bright red blood or local hematoma at the site of cannulation. The catheter may also be transduced to check for arterial waveform to identify the position of the catheter. Confirmation of an intra-arterial catheter is done by CT angiography [9].
A large calibre of the HD catheter may occlude the lumen of the artery and cause thrombus formation. On removal of the catheter directly, the possibility of thrombus migration exists that may lead to the occlusion of the intracranial vessels resulting in stroke. Hence, a neurological examination must be done after the repair of the artery [10]. Radial artery pulsation was also confirmed after suturing the rent and removal of the clamp.
Early diagnosis and early removal of the misplaced catheter is crucial since the chance of thrombosis and serious complications increases with the time elapsed since catheter placement [11]. As there could be the possibility of vessel injury and haemorrhage, adequate precautions must be taken such as hemodynamic monitoring, central venous access for resuscitation and inotropic support. Post-operative monitoring of vitals, haemoglobin estimation by Arterial Blood Gas (ABG) and repeat chest X-ray were advised to look for any complications.
Conclusion
Inadvertent intra-arterial placement of the catheters is a feared complication, and precautions must be taken like use of ultrasound guided techniques. In case of an intra-arterial cannulation, early removal of the catheter must be planned, and surgical exploration is the best option as it would avoid dreaded complications like bleeding (as the control of blood loss is difficult as in the above scenario) and vascular injury and its consequent repair.
Financial disclosures: None.
Conflicts of interest: None.
References
- Beecham GB, Aeddula NR. Dialysis Catheter. In: StatPearls. Treasure Island (FL): StatPearls Publishing. 2022; 19.
- El Khudari H, Ozen M, Kowalczyk B, Bassuner J, Almehmi A. Hemodialysis Catheters: Update on Types, Outcomes, Designs and Complications. Seminars in Interventional Radiology. 2022; 39(1): 90-102. doi:https://doi.org/10.1055/s-0042-1742346.
- Bream P. Update on Insertion and Complications of Central Venous Catheters for Hemodialysis. Seminars in Interventional Radiology. 2016; 33(01): 031-038. doi:https://doi.org/10.1055/s-0036-1572547.
- Thapa S, Terry PB, Kamdar BB. Hemodialysis catheter-associated superior vena cava syndrome and pulmonary embolism: A case report and review of the literature. BMC Research Notes. 2016; 9(1). doi:https://doi.org/10.1186/s13104-016-2043-1.
- Forneris G, Marciello A, Savio D, Gallieni M. Ultrasound in central venous access for hemodialysis. The Journal of Vascular Access. 2021; 19: 112972982110194. doi:https://doi.org/10.1177/11297298211019494.
- Calvert N, Hind D, McWilliams RG, Thomas SM, Beverley C, et al. The effectiveness and cost-effectiveness of ultrasound locating devices for central venous access: A systematic review and economic evaluation. Health Technology Assessment. 2003; 7(12). doi:https://doi.org/10.3310/hta7120.
- Palepu GB, Juneja Deven, Machiraju Subrahmanyam, S Venkata Mohan. Impact of ultrasonography on central venous catheter insertion in intensive care. 2009; 19(03): 191-198. doi:https://doi.org/10.4103/0971-3026.54877.
- Guilbert MC, Elkouri S, Bracco D, et al. Arterial trauma during central venous catheter insertion: Case series, review and proposed algorithm. Journal of Vascular Surgery. 2008; 48(4): 918-925. doi:https://doi.org/10.1016/j.jvs.2008.04.046.
- Pikwer A, Acosta S, Kölbel T, Malina M, Sonesson B, Åkeson J. Management of Inadvertent Arterial Catheterisation Associated with Central Venous Access Procedures. European Journal of Vascular and Endovascular Surgery. 2009; 38(6): 707-714. doi:https://doi.org/10.1016/j.ejvs.2009.08.009.
- Yosuke Moteki, Yamaguchi K, Kawashima A, Sato S, Okada Y. Early open surgery for the accidental insertion of a hemodialysis catheter into the carotid artery: A case report. Interdisci plinary neurosurgery. 2014; 1(4): 94-96. doi:https://doi.org/10.1016/j.inat.2014.08.001.
- Hoffmann K, Schott U, Erb M, Albes J, Claussen CD, et al. Remote suturing for percutaneous closure of popliteal artery access. Cathet Cardiovasc Diagn. 1998; 43(4): 477-482. doi:10.1002/(sici)1097-0304(199804)43:4 < 477::aid-ccd30>3.0.co;2-e.